


Clinical Presentation
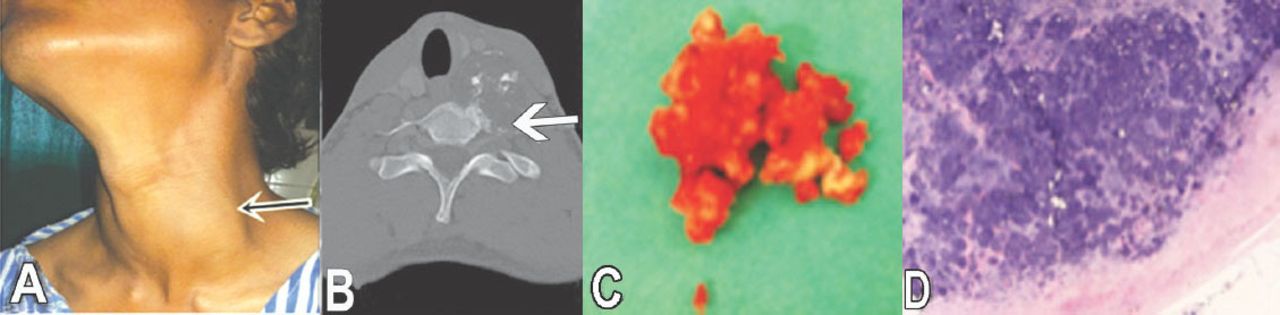
A 20-year-old male presented with painless swelling in the left lower anterior aspect of neck of one year duration Figure 1A. The swelling was well-defined, unmovable, size 8×6 cm, smooth surface, normal temperature, and firm in consistency. The swelling was not moving with deglutition and there was no pressure effect on surrounding structures. Routine biochemical and hematological tests including hemogram with erythrocyte sedimentation rate, total leucocyte count, and differential leucocyte counts were normal. Plain radiograph, MRI, contrast enhanced (CE) CT scan of the cervical spine (Figure 1B) revealed a lesion arising from the left anterior part of the C7 vertebral body with evidence of multiple foci of calcification.

Clinical photograph of tumor situated in the: A) lower third of the left side of neck; B) contrast enhanced CT scan of the cervical spine showing evidence of a well defined lesion with irregular lobulated margins and areas of chondroid calcification seen in axial bone window image; C) gross surgical specimen after excision and photomicrograph; and D) shows a cap of normal hyaline cartilage with lacunar cells bearing eosinophilic inclusions in the cytoplasm.
Questions
What is the diagnosis?
What is the management?
Answers
On the basis of plain radiograph, CECT, and MRI, a provisional diagnosis of benign cartilaginous neoplasm was made. The fine needle aspiration cytology and trucut biopsy from the lesion revealed it to be a cartilaginous tumor, which was further confirmed after surgical removal of tumor mass (Figure 1C) and histopathological examination (Figure 1D).
A complete surgical excision of the tumor was planned. He was placed supine; we approached the tumor through an anterior approach retracting the sternocleidomastoid and carotid sheath laterally, and the esophagus and trachea medially. The deep cervical fascia was divided, and the longus colli muscles were reflected subperiosteally. The tumor was excised completely, and adjacent structures were found free from any infiltration. The wound was closed after achieving hemostasis. He was completely free from disease after one year of follow up.
Discussion
Chondroma is a benign cartilaginous neoplasm.1 Small bones of the hands and feet are most commonly involved, sometimes it may also occur in the ribs and pelvis, and rarely in the intracranial bones.2 Enchondromas are rarely present in the spine, comprising 2% of all chondromas.3 An enchondroma may occur as a single tumor or many tumors together. Chondromas are usually asymptomatic. However, proper diagnosis and total removal of the tumor are important because benign chondromas can transform into malignancy. Benign chondrogenic tumors can be classified into 4 types as proposed by Lichtenstein.3 The 4 histological types in this classification are; osteochondromas, enchondromas, chondroblastoma, and chondromyxoid fibroma. Different types have their own location of occurrence and frequency. Chondroma is the most common chondrogenic tumor, and it accounts for 2.4% of all osteocartilaginous tumors.4 Chondromas of the spinal column comprise <5% of primary spinal tumors.5 In particular, symptomatic chondromas of the cervical spine are rare, and based on a PubMed literature reviews, only 19 cases have been reported so far.
Chondromas are usually found in the 20-40 years age group.1 Symptoms are usually swelling and pain at the lesion site. Many authors have reported enchondroma of the lumbar spine presenting with sciatica.1 However, in this case, the patient presented with swelling and mild pain around the lower neck.
Chondromas can be classified into 2 types according to their site of origin: the medullary cavity (enchondroma) and the surface of the periosteum (periosteal chondroma).1 In our case, the type was periosteal chondroma. The periosteal chondromas usually do not infiltrate the adjacent soft tissue even with increase in size. Chondroma can arise from any part of the vertebra including body, lamina, pedicle, and spinous process.
Plain films of x-rays show smooth erosions of the bone structure, which are sometimes radiolucent or sometimes calcified. The CT shows a soft tissue mass with stippled calcifications. The MRI demonstrates a subperiosteal lobulated mass at the bone surface with peripheral rim enhancement on T1WI.1 Nevertheless, MRI is also important for differential diagnosis because tumor size, location, pattern, and relation of surrounding structures can also be identified. It is often difficult to differentiate chondromas from other cartilaginous tumors on the radiologic finding alone. Hence, biopsy is needed for proper diagnosis.
Chondromas, which are also known as enchondromas, consist of benign hyaline cartilage, tissues of chondrocytes and cancellous bone tissue. Enchondromas are cartilage-capped bony projections that grow from heterotopic cartilaginous cell rests of the medullary cavity of bone. These cartilaginous rests are cells that are somehow displaced from the growth plate.3 Complete involvement of the cortex and soft tissue is highly suggestive of malignancy. The most common malignant transformation of chondromas is chondrosarcoma.3 Histologically, the cells of enchondromas resemble cells of normal hyaline cartilage. Cells with large nuclei are suggestive of malignancy.
The treatment of choice for chondroma is complete surgical excision.2 Although recurrence of chondroma is rare, it can recur with incomplete removal. Nearly 10% of solitary chondromas undergo malignant transformation that requires radiation therapy.1 The malignant transformation rate is very slow, but is more than 50% as a part of Ollier’s and Maffucci’s syndromes.1
In conclusion, chondromas are rare cartilaginous neoplasms affecting the cervical spine. Meticulous preoperative and histopathological evaluation is important because these pathologies possess potential for malignant transformation.
Student Corner
We invite students from a variety of medical disciplines to submit original contributions based on their supervised research.
The Student Corner of Saudi Med J aims to help students explore research opportunities and network with other peers and mentors in the same field.
Submission Guidelines
Submitted Abstracts should include the following:
Title should be descriptive
Author’s names and affiliation(specify college level/year, academic degree of Senior Author)
Abstract must be structured and not more than 300 words
The following are the typical headings:
Objectives (background, why the study was done, specific aims)
Methods (setting, date of study, design, subjects, intervention and analysis)
Results (findings, data and statistical tests) and
Conclusion (general interpretation of results)
General Information on Abstract Submission
Submitted Abstracts should be co-authored by a Senior Supervisor
Abstracts will be reviewed by Student’s Corner Section Editor
There is no fee to submit an Abstract
Ethical Approval should be provided
Acknowledgment
The author would like to thank Dr. Mehtab Ahmad, Assistant Professor, for reporting the radiology films.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42846.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.