


Abstract
Venous thromboembolism (VTE) including deep vein thrombosis (DVT) and pulmonary embolism (PE) is commonly encountered in daily clinical practice. After diagnosis, its management frequently carries significant challenges to the clinical practitioner. Treatment of VTE with the inappropriate modality and/or in the inappropriate setting may lead to serious complications and have life-threatening consequences. As a result of an initiative of the Ministry of Health of the Kingdom of Saudi Arabia, an expert panel led by the Saudi Association for Venous Thrombo-Embolism (a subsidiary of the Saudi Thoracic Society) and the Saudi Scientific Hematology Society with the methodological support of the McMaster University Guideline working group, this clinical practice guideline was produced to assist health care providers in VTE management. Two questions were identified and were related to the inpatient versus outpatient treatment of acute DVT, and the early versus standard discharge from hospital for patients with acute PE. The corresponding recommendations were made following the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) approach.
Venous thromboembolism (VTE) comprised of deep vein thrombosis (DVT) and pulmonary embolism (PE) is a relatively common disease affecting approximately 100 per 100,000 people per year.1-3 It is estimated that approximately 25,000 people are affected in the Kingdom of Saudi Arabia (KSA) annually. The major risk factors of VTE include age, surgery, hospitalization, immobility, trauma, cancer, pregnancy, and puerperium, hormone use, obesity, and inherited and acquired hypercoagulable states.4 The venous thromboembolism is associated with significant morbidity and mortality,5 especially when not treated appropriately. The standard treatment of acute DVT had been hospital admission and anticoagulation with unfractionated heparin intravenously for approximately 5-7 days. With the introduction of low molecular weight heparin (LMWH), which proved to be effective when given subcutaneously, the setting for acute DVT treatment became an issue of investigation. Recent evidence supports the use of direct oral anticoagulants in the initial VTE treatment with safe outcomes compared with conventional therapy.6 Additionally, the duration of hospitalization needed to safely and successfully manage acute PE had been another area of consideration taking into account the increasing costs of health care and the need for optimal resource utilization. There is a lack of previous guidelines on VTE management from KSA. Given the importance of this topic, the Saudi Ministry of Health (MoH) produced this clinical practice guideline on the management of VTE to assist health care providers (HCP) in evidence-based clinical decision-making. In this document, we report the recommendations of the Saudi Expert Panel (SEP) for the inpatient versus outpatient VTE treatment. The full guideline is available at: http://www.moh.gov.sa/depts/Proofs/Pages/Guidelines.aspx7
Methods
This clinical practice guideline was a part of a larger initiative by the Saudi MoH to ensure quality care and reduce variability in clinical practice across the Kingdom through proper adaptation and de novo development of practice guidelines. In 2013, the Saudi MoH, through the Saudi Center for Evidence Based Healthcare, partnered with the McMaster University guidelines group and contacted the Saudi Scientific Hematology Society and the Saudi Association for VTE (SAVTE) to nominate a group of clinicians to serve as expert panelists for guideline development on VTE treatment. The methodology used to develop recommendations and grade the quality of the supporting evidence is briefly described below. Its details are available in a separate publication.8
The overall process
The guideline panel selected the clinical questions of this guideline by a formal prioritization process based on a 9-point Likert scale ranking of several questions on VTE management. The McMaster University guideline group updated the systematic reviews that were related to the selected questions by searching for trials that were subsequently published in the Cochrane Central Register of Controlled Trials, MEDLINE, and EMBASE until November 2013. When relevant, the meta-analyses were updated. The group also conducted systematic searches for information that was specific to the Saudi context, such as patients’ values and preferences, and cost. Next, the McMaster guideline leader developed a summary of findings and evidence-to-recommendation tables for each question, and shared them with the SEP members. The guideline panel was asked to provide additional information, including unpublished data. The guideline panel met in Riyadh, KSA on December 3, 2013, and developed the final recommendations using a structured consensus process with voting used to reach consensus in some cases.8 Transparent documentation of all decisions was performed. The SEP members reported their potential conflicts of interests, which were managed according to the World Health Organization guidelines.9
The selected questions
The following are the 2 clinical questions that were selected by the KSA guideline panel and addressed in this guideline. For details on the process by which the questions were selected, please refer to the separate methodology publication:10 1) Should home treatment versus hospital treatment be used for patients with acute DVT of the leg?; 2) Should early discharge versus standard discharge from hospital be used for patients with acute PE?
Grading the quality of evidence
The SEP assessed the quality of evidence using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) approach.11 The quality of evidence was classified as “high”, “moderate”, “low”, or “very low” according to the following definitions:12 High: We are very confident that the true effect lies close to that of the estimate of the effect;12 Moderate: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different;12 Low: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect;12 and Very low: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect.12
Grading the strength of recommendations
The GRADE Working Group defines the strength of recommendation as the extent to which we can be confident that desirable effects of an intervention outweigh undesirable effects.13 According to the GRADE approach, the strength of a recommendation is either strong or conditional (weak), and has explicit implications (Table 1).13 Understanding the interpretation of the strength of recommendation is important when making clinical decisions.
Interpretation of strong and conditional (weak) recommendations.
Results
This guideline, which was issued in 2014, covered outpatient versus inpatient management of VTE. The recommendations for the 2 selected questions took into consideration the available evidence, resource use, and the Saudi context.
Question 1: Should home treatment versus hospital treatment be used for patients with acute DVT of the leg?
The summary of evidence on this question was based on a systematic review by Othieno et al.14 The updated literature search identified one new study conducted in KSA by Algahtani et al.15 This new study was included in the updated meta-analysis. The summary of findings is provided in Table 2.14-23
Summary of findings on home treatment compared with hospital treatment for patients with deep venous thrombosis (DVT).
Benefits and harms of the option
The meta-analysis of 7 trials (total of 1769 participants) found moderate quality evidence that home treatment of DVT reduces recurrent VTE (risk ratio [RR] 0.65; 95% confidence interval [CI]: 0.44-0.94; absolute effect: 27 fewer events per 1000). The meta-analysis of 6 studies (total of 1708 participants) found low quality evidence that home treatment of DVT reduces major bleeding (RR 0.67; 95% CI: 0.33-1.36; absolute effect: 7 fewer events per 1000). It was unclear what the effects of home treatment of DVT on mortality (RR 0.72; 95% CI: 0.45-1.15) and quality of life were.
Values and preferences
The SEP judged that the values and preferences may vary. Some patients and carers would prefer for the patient to be admitted. Some others would prefer to be discharged if they know they could easily access a physician.
Resource use
Health economic evaluations in settings different from that of KSA conclude that home treatment is cost-saving of approximately US$500-US$2500 per patient.22-28 We identified 2 studies conducted in KSA. Algahtani et al15 conducted a prospective study of 61 DVT cases presenting to the emergency department (Aug 2009-Aug 2010) of King Khalid University Hospital. The mean outpatient cost was significantly lower (1750 versus 4338 US$).15 Al eissi Salih and Hosny29 conducted a retrospective chart analysis of DVT cases managed between 2005 and 2012 at King Abdulaziz Medical City, Riyadh, KSA. Of 190 DVT cases, 80 (42%) were eligible for outpatient management. The authors concluded that 78.75 bed days would have been saved per year and cost savings would be SR118,125 per year.29
Other considerations
The SEP judged home treatment of DVT to be acceptable to physicians and the Saudi MoH. However, they were concerned with the lack of ultrasound service after 4:30 P.M. and on weekends in emergency rooms.
Implementation considerations
The SEP thought that there is a need to have ultrasound services to diagnose DVT available 24 hours per day 7 days per week, and to have 24-hour clinic coverage for these patients (for example, thrombosis services).
Monitoring and evaluation
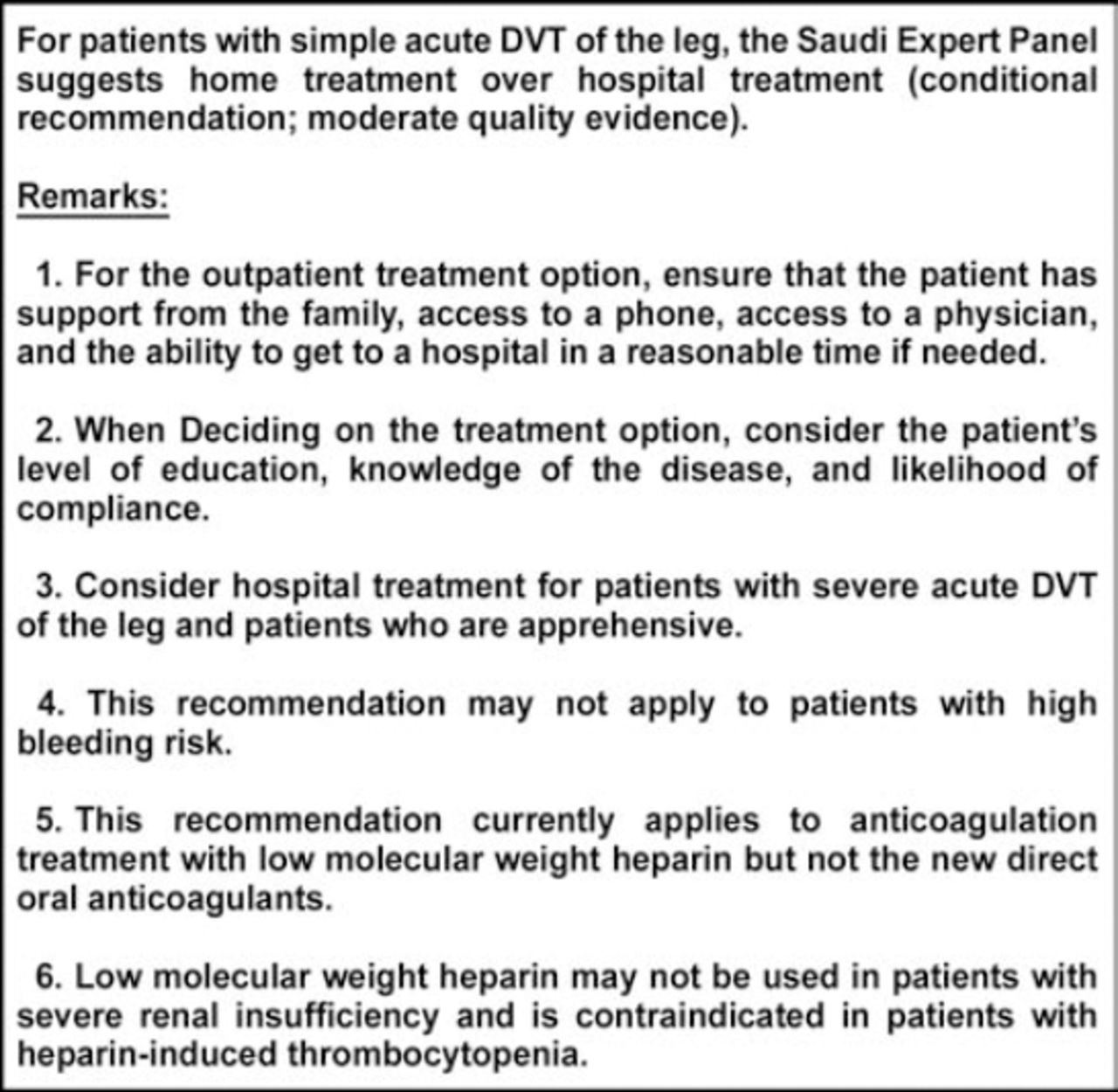
The SEP proposed monitoring the percentage of patients treated at home versus hospital and studying the impact of implementing this recommendation on outcomes and costs. The recomendation for question one is presented in Figure 1.
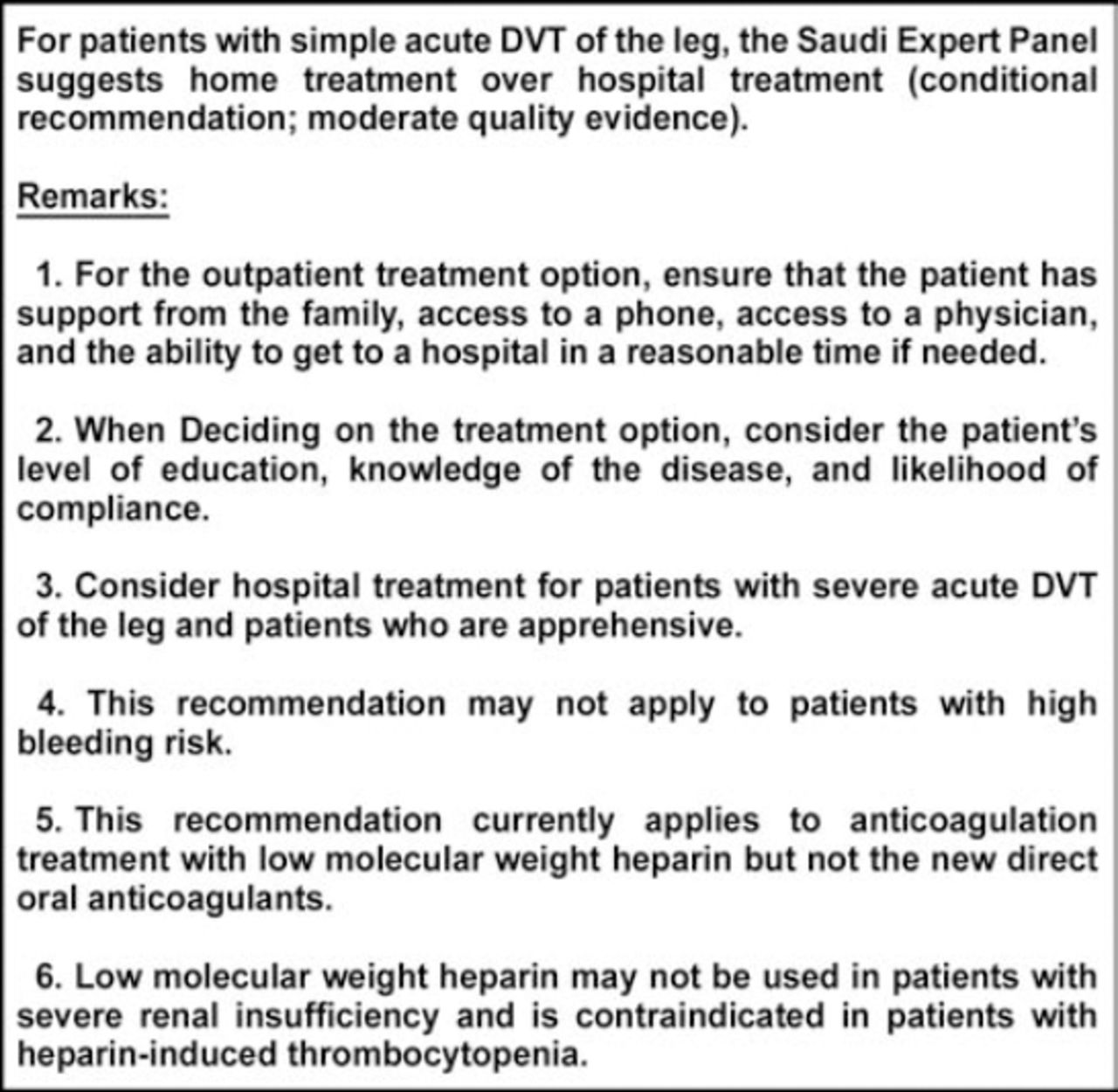
The Saudi Expert Panel recommendation for question one: Should home treatment versus hospital treatment be used for patients with acute deep venous thrombosis (DVT) of the leg?
Question 2: Should early discharge versus standard discharge be used for patients with acute PE?
The summary of evidence is based on a systematic review Otero et al,30 and a more recent trial by Aujesky et al.31 The updated literature search identified one new systematic review by Piran et al,32 which did not identify any trial not already considered. The summary of findings is provided in Table 3.30-33
Summary of findings on early discharge versus standard discharge in the treatment of acute pulmonary embolism (PE).
Benefits and harms of the option
The meta-analysis of 2 trials (total of 471 participants) found moderate quality evidence of possible increase in VTE (RR 1.23; 95% CI: 0.25-6.03) and major bleeding (RR 2.74; 95% CI: 0.45-16.71).32 However, any absolute increase in these outcomes would be of small size given the low baseline risks (2 more VTE per 1000 and 8 more major bleeding per 1000 over a 3 months period). Observational data confirm low risk of recurrent VTE in patients with low risk acute PE.32
Values and preferences
The SEP judged that values and preferences may vary. Some patients and carers would prefer for the patient to be admitted. Some others would prefer to be discharged if they know they could easily access a physician.
Resource use
We did not identify any studies directly related to PE, so the SEP relied on indirect evidence related to DVT. As stated earlier, health economic evaluations in both KSA15,29 and non-KSA settings22-28 conclude that home treatment of DVT is cost-saving.
Other considerations
The SEP advocated assessing PE severity using a validated tool such as the Pulmonary Embolism Severity Index.34 The SEP also judged that the acceptability of early discharge might vary by physician. Some of them might be apprehensive to releasing patients early given the gravity of the condition. Implementation considerations. Early discharge is potentially feasible but requires 24-hour clinic coverage for the patients (for example, thrombosis services).
Monitoring and evaluation
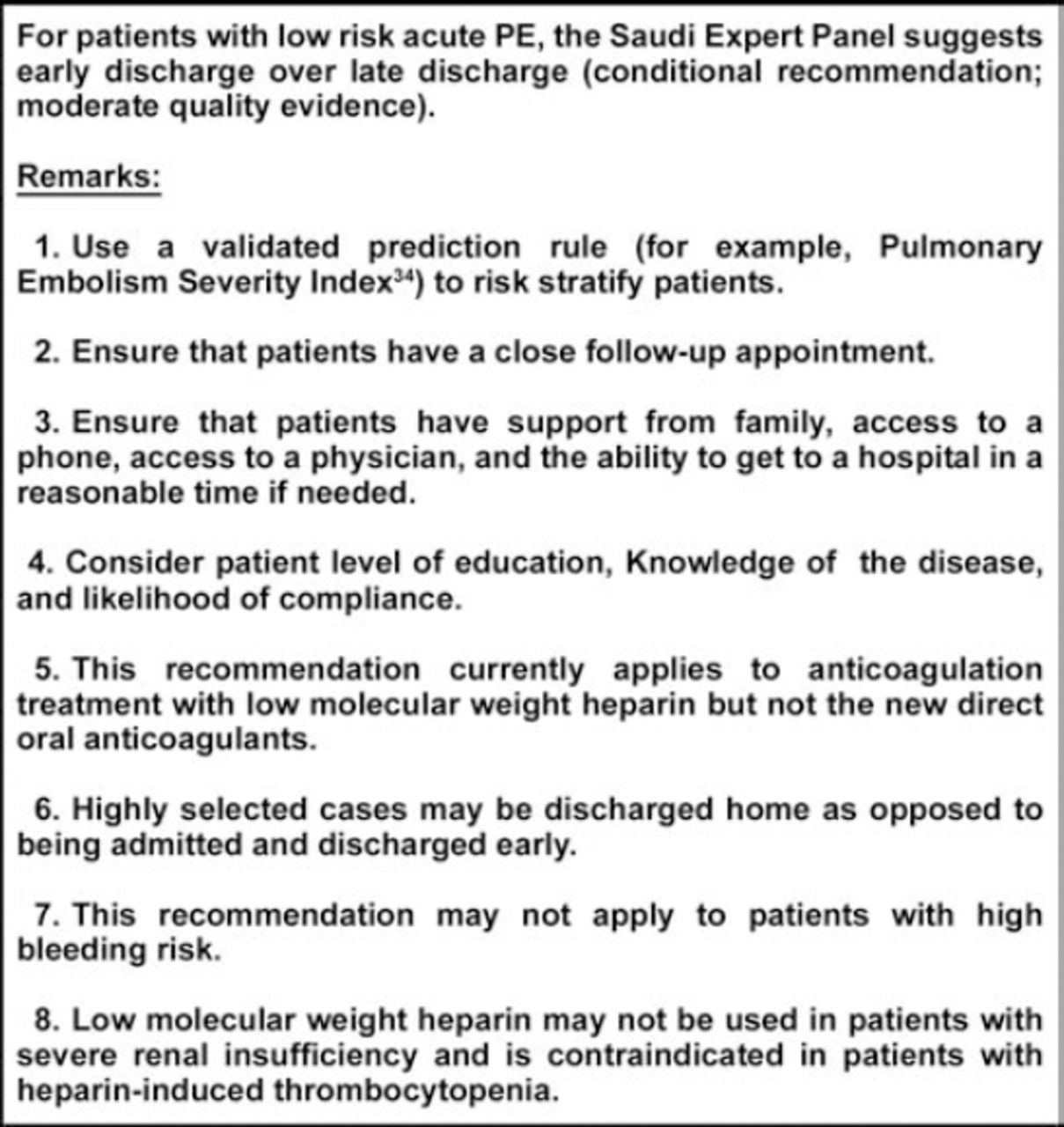
The SEP proposed auditing the percentage of patients discharged early versus late and studying the impact of implementing this recommendation on outcomes and costs. The recommendation for question 2 is presented in Figure 2.

The Saudi Expert Panel recommendation for question 2: Should early discharge versus standard discharge be used for patients with acute pulmonary embolism (PE)?
Discussion
The purpose of this clinical practice guideline is to provide guidance on selected clinical questions related to the management of acute DVT and PE, and the best and safe management settings. This guideline is a part of a larger initiative of the Saudi MoH aiming at providing evidence-based guidance for clinicians and reducing variability in clinical practice in the KSA. The target audience of the guideline includes primary care physicians and specialists in Emergency Medicine, Internal Medicine, and Hematology/Oncology in KSA. The guideline may benefit other health care professionals, public health officers, and policy makers. However, it is not intended to be a care standard. Clinicians, patients, third-party payers, institutional review committees, other stakeholders, and courts should never view the guideline recommendations as dictates as no guideline can take into account all of the unique features of individual clinical circumstances. The remarks accompanying each recommendation are integral parts, facilitate accurate interpretation, and should never be omitted when quoting or translating the recommendations.
This guideline was the first from KSA and the region on this topic. As it took into consideration the local context, it has higher chance of acceptance by HCP working in the area, which may improve health care quality and promote efficient use of the available resources. The recommendations in this guideline shared similarities with other recommendations. For example, the 9th Edition of Antithrombotic Therapy by the American College of Chest Physicians recommended initial treatment at home over treatment in hospital for patients with acute DVT of the leg, and who had adequate home circumstances (namely, strong recommendation).5 The European Society of Cardiology guideline stated that early discharge and continuation of treatment at home should be considered for patients with acute low risk PE if proper outpatient care and anticoagulant treatment can be provided.35 The 9th Edition of Antithrombotic Therapy suggested early discharge over standard discharge in patients with low risk PE and whose home circumstances are adequate (namely, conditional recommendation).5
It should be noted that this guideline did not address all the questions related to VTE treatment. For instance, the use of direct oral anticoagulants for the initial management of VTE is not addressed. Based on recent randomized controlled trials, the 2014 European Society of Cardiology guideline on acute PE treatment recommended the new direct oral anticoagulants as alternatives to the combination of parenteral anticoagulation with a vitamin K antagonist.35
In addition, the SEP suggested local research on the values and preferences of the Saudi population regarding VTE in general, its treatment with the various modalities and the potential side effects from such treatments. The SEP advocated the performance of studies that compare the impact of early versus late hospital discharge on various outcomes, such as recurrent VTE, post-thrombotic syndrome, bleeding and mortality, and the effectiveness of newer oral anticoagulants versus the different heparins.
In conclusion, this Saudi clinical practice is on outpatient versus inpatient VTE management. The SEP suggests home treatment over hospital treatment for patients with simple acute DVT, and suggests early discharge over late discharge for patients with low risk acute PE.
Acknowledgment
The authors would like to thank Dr. Mohammed Zamakhshary, Dr. Zulfa Alrayess, Dr. Yaser Adi, and the members of the Saudi Center for Evidence Based Healthcare, Ministry of Health, Kingdom of Saudi Arabia for their unlimited support.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This clinical practice guideline was funded by the Ministry of Health, Riyadh, Kingdom of Saudi Arabia.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.