


Abstract
Objectives: To report our experience in sentinel lymph node biopsy (SLNB) in early breast cancer.
Methods: This is a retrospective study conducted at King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia between January 2005 and December 2014. There were 120 patients who underwent SLNB with frozen section examination. Data collected included the characteristics of patients, index tumor, and sentinel node (SN), SLNB results, axillary recurrence rate and SLNB morbidity.
Results: There were 120 patients who had 123 cancers. Sentinel node was identified in 117 patients having 120 tumors (97.6% success rate). No SN was found intraoperatively in 3 patients. Frozen section results showed that 95 patients were SN negative, those patients had no immediate axillary lymph node dissection (ALND), whereas 25 patients were SN positive and subsequently had immediate ALND. Upon further examination of the 95 negative SN’s by hematoxylin & eosin (H&E) and immunohistochemical staining for doubtful H&E cases, 10 turned out to have micrometastases (6 had delayed ALND and 4 had no further axillary surgery). Median follow up of patients was 35.5 months and the mean was 38.8 months. There was one axillary recurrence observed in the SN negative group. The morbidity of SLNB was minimal.
Conclusion: The obtainable results from our local experience in SLNB in breast cancer, concur with that seen in published similar literature in particular the axillary failure rate. Sentinel lymph node biopsy resulted in minimal morbidity.
Breast cancer (BC) is the top cancer in women both in the developed and developing world.1 In the USA, nearly 230,000 BCs are diagnosed annually.2 The population of Kingdom of Saudi Arabia (KSA) is approximately 30 million, 65% of them are below the age of 30.3 In KSA, the total number of patients diagnosed to have BC in the year 2010 was 1,473 patients, which constituted 27.4% of all newly diagnosed female cancers in the year 2010. The Age Standardized Rate was 24.9/100,000 for female population. The median age at diagnosis was 49 years. More than half of BC patients in KSA presented with locoregional or distant disease.4 In KSA, there is no national screening program for BC and the Saudi Cancer Registry does not include ductal carcinoma in situ (DCIS) cases in their capture form, which may explain the low number of DCIS cases reported from local centers. It is clear that, KSA is among countries with low disease burden, but it is expected that this burden will increase in the years to come.5 Axillary lymph node status is considered the most important prognostic factor for patients with BC, and it participates largely in the decision regarding subsequent adjuvant systemic treatment.6,7 Axillary lymph node dissection (ALND) for patients with BC was introduced more than 200 years ago for staging and local control.8,9 It is associated with an increase risk of adverse outcomes, including lymphedema in 14% of cases, limited shoulder motion in 28% of the cases and neuropathic pain in 31% of the cases.10 The therapeutic advantage of removing negative nodes with respect to axillary control and survival remains questionable.11-14 At the present time, most BC patients receive some sort of adjuvant systemic therapy irrespective of their lymph node status.15 Based on that, minimally invasive procedures for staging the axilla have been introduced. Sentinel lymph node biopsy (SLNB) in BC, a minimally invasive procedure, was first described in 1994.16 Since then, it has been widely practiced with a wide literature to support its reliability for ascertaining the status of the axillary lymph nodes. Currently, SLNB is accepted as the standard of care for axillary staging in early BC.17-19 In this paper, we are documenting the beginning, development, results and follow up of patients who underwent SLNB for BC at King Khalid University Hospital (KKUH), Riyadh, Saudi Arabia.
Methods
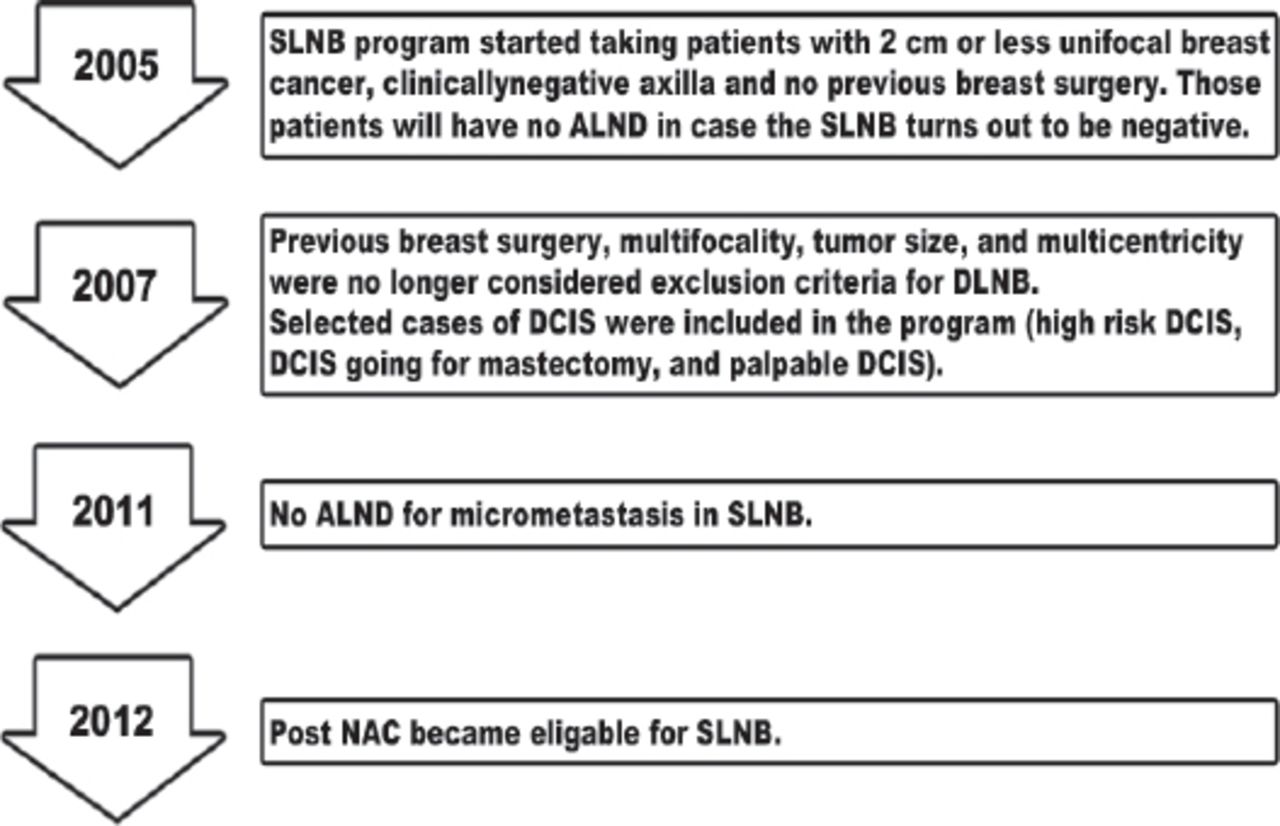
Over a 10-year period (January 2005 to December 2014), a total of 916 BC patients were diagnosed and treated at KKUH (6 patients with pure DCIS and 910 patients with invasive disease). Of those 916 patients, there were 120 patients who fulfilled the criteria to undergo SLNB procedure, 3 of them had bilateral disease. The inclusion criteria were set at the beginning of the experience and changed as time passed by, the changes in the inclusion criteria were based on cumulative scientific evidence favoring the change (Figure 1). The Institutional Review Board, College of Medicine, King Saud University (Ethical Review Committee) approved this study.
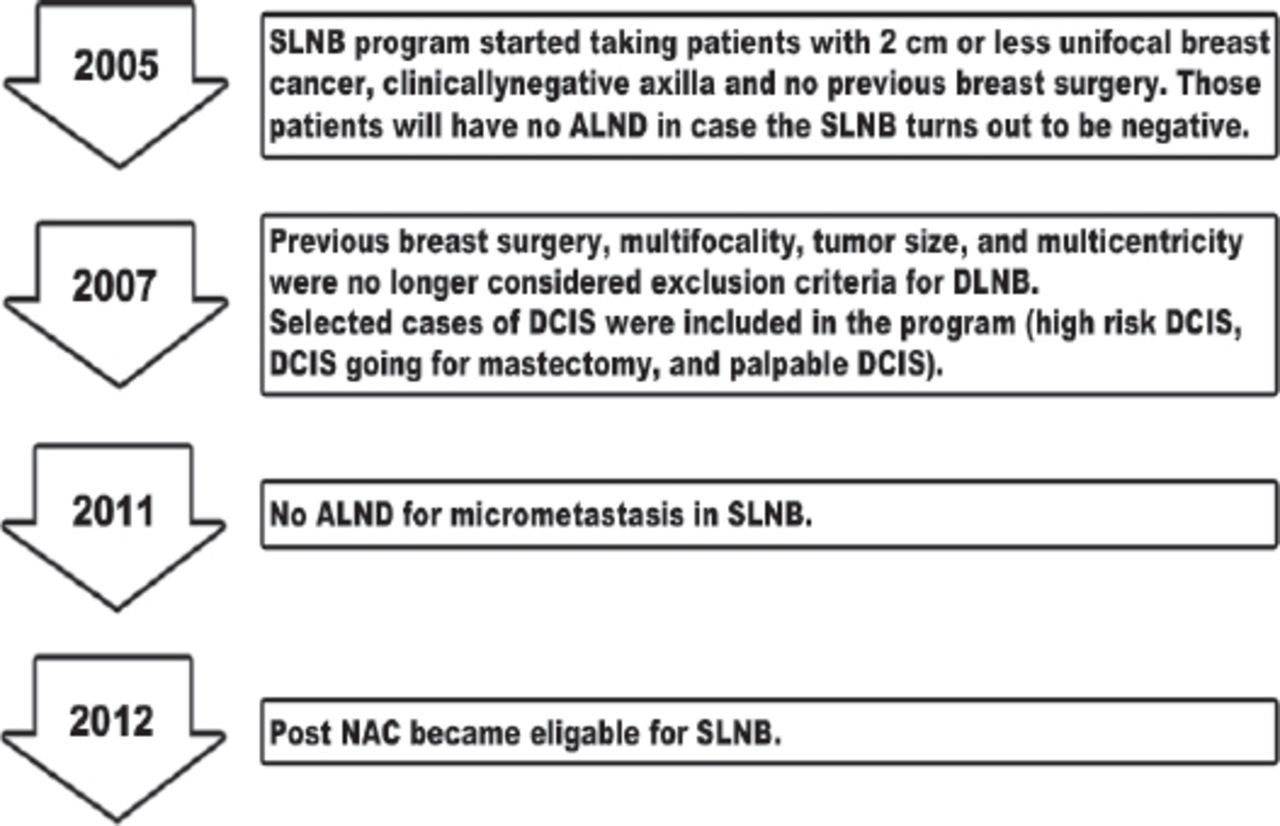
Beginning and development of sentinel lymph node biopsy (SLNB) program at King Khalid University Hospital, Riyadh, Saudi Arabia. ALND - axillary lymph node biopsy, DCIS - ductal carcinoma in situ, NAC - neoadjuvant chemotherapy
We conducted the study by reviewing the data of 117 patients who had 120 SLNB procedures, of them, 85 sentinel node (SN) negative patients who had only SLNB with no further ALND and 10 patients who had negative SN on frozen section (FS), doubtful hematoxylin & eosin (H&E) result, but turned out to have micrometastasis on immunohistochemistry (IHC) testing, ALND was performed to 6 of the 10 patients, but no ALND was performed on the remaining 4 patients. Twenty-five patients in this series had positive SN on FS, so immediate ALND was performed to them. At KKUH, the first case of SLNB in BC was carried out in 2005 by one of the surgeons who had formal overseas training on the procedure where he attained the initial learning phase and validation of the procedure.
Patient’s characteristics were age, gender, bilaterality, and hormonal status. Tumor characteristics were histological type, tumor size, lymphovascular invasion, tumor grade, perineural invasion, hormonal receptors. Sentinel node characteristics were number of SN removed, FS result, H&E result, IHC result, and ALND result (in case of positive SN). Tumors were classified histologically according to the American Joint Cancer Commission Staging System.20
Sentinel lymph node identification procedures
Sentinel lymph node biopsy was performed using isotope and blue dye together, and were all carried out under general anesthesia. The radiotracer is injected early in the morning when the procedure is planned to be performed in the afternoon same day or late afternoon the day before the procedure when the SLNB is planned to be carried out in the early morning next day. The blue dye is injected just after induction of anesthesia. One-and-a-half ml Tc99m sodium pertechnetate (GE Healthcare Limited, HP7 9LL, United Kingdom) with activity ranging from 5-100 mCi (185-3700 MBq) is introduced in a vial. Four syringes are prepared from this vial, each syringe contains 0.1-0.2 ml Tc99m albumin colloid containing 0.2-0.4 mCi (7.4-14.4 MBq). The material is injected at 4 peritumoral sites or in the periareolar area in cases with multifocal or multicentric cancers, then the nurse performs gentle breast massage for 30 minutes to facilitate migration of the particles toward the axilla. Post injection imaging is performed using gamma camera (Phillips SPECT-CT system, Andover, Massachusetts, USA 01810-1099). Anterior and lateral views are obtained 15 minutes post injection and continued until the SN is visualized or the study is declared negative from imaging point of view. Two-and-a-half ml of sterile saline plus 2.5 ml of the blue dye (Bleu Patente V, Sodique Guerbet 2.5%, France) are mixed and injected subdermally peritumorally just after induction of anesthesia, followed by breast massage for 5 minutes. The axilla is explored 10-15 minutes after the blue dye injection and massaging. A lymph node is called SN when it is blue stained or there is a blue lymphatic channel leading to it, or when it is a hot node by using the gamma detector probe (GPS Navigator GPS-9100-00 Dynasil, USA). After the removal of the SN, the axillary basin is checked for residual radioactivity, a count less than 10% of the hottest SN is considered a background activity. The SN(s) is/are sent for FS. At the FS laboratory, each lymph node is sliced perpendicular to its long axis, touch preparation are submitted from the cut surfaces and stained with modified giemsa stain (Diff Quick). The entire lymph node(s) is/are submitted after slicing for FS, the slices are performed in an equidistant manner of 2mm thickness for each slice. Immunohistochemistry is used for doubtfully negative H&E cases. Macrometastases are defined as metastatic lesions larger than 2.0 mm, whereas micrometastases is defined as metastatic lesions between 0.2-2.0 mm. In case the SN is positive for metastasis by FS, ALND is carried out immediately (level 1 & level 2), but if the SN is negative by FS, no ALND is performed. When no axillary SN is identified by both modalities, an axillary lymph node dissection is carried out immediately. While waiting for the FS result, the planned breast procedure is performed.
Statistical analysis
All data collected were encoded into a Microsoft Excel program and analyzed using Predictive Analysis for Social Sciences (PASW) Version 19.0 (IBM SPSS Inc., Chicago, IL, USA). Results are presented as frequency (number) and percentages.
Results
Between January 2005 and December 2014 (10 years period), a total of 916 BC patients were diagnosed and treated at KKUH. Of those 916 patients, 120 female patients were seen to be suitable for SLNB procedure. The median age was 48 years, the mean age was 49.2 ± 10.4 years. Patients in this series are mostly pre-menopausal (65%). Infiltrating ductal carcinoma was seen in 106 of our patients (86.2%), whereas lobular carcinoma was seen in 11 patients (8.9%). There were 6 cases of DCIS (4.9%). The tumor size was T1 in 40 patients (32.5%), T2 in 79 patients (64.2%), and T3 in 4 patients (3.3%). Grade 2 tumors were seen in 82 patients (66.7%), grade 3 tumors in 30 patients (24.4%), and grade one tumors were seen only in 11 patients (8.9%). Lymphovascular invasion was seen in 21.1% and perineural invasion was seen in 12.2%. There were 20 patients with multifocal disease (16.7%) and 10 patients with multicentric disease (8.3%). Eighteen patients (15.4%) received NAC prior to SLNB procedure. Almost 70% of our patients were estrogen hormone positive and 20.3% were Her2 positive (Table 1). In the first few years of this study, the number of recruited patients was very little due to the low volume of BC patients referred to our center and also due to the strict inclusion criteria for the study, but as time passed by the number of BC patients referred to our center has increased and our inclusion criteria was modified to include more patients (Figure 1).
Patients’ demographic and tumor characteristics (120 patients, 3 of them having bilateral cancer).
The SLNB procedure was successfully carried out in 117 out of 120 patients (97.6% success rate).3 Of the 117 patients, 3 had bilateral disease, so there were 120 SLNB procedures performed. A combination of radiolabeled technetium and patent blue dye were used to map and localize the SN in all patients. In 3 cases, the SN was not identified by both modalities; thus, ALND was performed immediately on these 3 patients.
Intraoperative SN identification
Sentinel node was identified intraoperatively in 120 out of 123 tumors (97.6% success rate). Three patients had bilateral disease. Ninety-six percent of SN were identified by lymphoscintigraphy, while 92% was identified by the patent blue dye method. The number of SN harvested was one in 36 cases (30%), 2 in 60 cases (50%), 3 in 19 cases (15.8%), 4 in 3 cases (2.5%), and 5 in 2 cases (1.7%) (Table 2).
Details of sentinel lymph node (SLN) findings in 120 patients who underwent SLNB.
Sentinel node results
Of the 120 SLNB’s, FS examinations resulted in 25 positive SN (20.8%), all had immediate ALND. The remaining 95 cases (79.2%) were reported as negative SN by FS and consequently, no ALND was performed on them. Hematoxylin & eosin staining of SN revealed results similar to that of FS. Cytokeratin immunohistochemistry (IHC) staining was carried out to doubtfully negative H&E results, which revealed positivity in 10 out of 95 SN (10.5%). These 10 SN’s contained micrometastases (cancer deposits from 0.2-2.0 mm). Of these 10 SN’s containing micrometastases, 6 patients were subjected to delayed ALND (early phase of study), whereas the other 4 patients did not have delayed ALND (late phase of study) (Table 2).
Axillary lymph nodes status of patients submitted to ALND for a positive SN
In 6 patients who had micrometastases, the positive SN was the only positive lymph node in the axillary basin, but in the macrometastases patients (25 cases), only 8 patients had positive lymph nodes in the axillary basin other than the positive SN (25.8%). We opted not to do ALND for the other 4 cases of micrometastases, so there were 31 ALND for a positive SN. Only 8 cases (25.8%) showed positive lymph nodes in the axillary basin other than the positive SN (Table 3).
Axillary lymph nodes status of patients submitted to ALND after a positive SLNB.
Table 4 shows the characteristics of all the SN’s obtained in this series. There were 35 positive SN’s (25 macrometastases and 10 micrometastases). In 21 cases (60%), there was only one positive SN, in 11 cases (31.4%) there were 2 positive SN’s, and in 3 cases (8.6%) there were 3 positive SN’s. All the SN’s in this study were obtained from the ipsilateral axilla. In 23 out of 31 ALND cases (74.2%), the SN was the only positive node in the axillary basin. There was a discordance between FS and final pathology result, which was seen in 10 cases (the micrometastases cases by IHC).
Characteristics of 120 sentinel nodes (SN) from studied patient.
Table 5 shows that 71 patients (59.2%) had breast conservative therapy followed by whole breast irradiation. Forty nine patients (40.8%) had mastectomy. In the late phase of the study, we included 18 patients (15.4%) who received NAC prior to having SLNB.
Treatments and events outcome in 120 patients who underwent SLNB.
Events in the study group
At a median follow up of 35.5 months, none of the patients who had SLNB (only) developed lymphedema, arm numbness, or shoulder joint dysfunction of the operated side, yet there were 2 wound infections and 3 seromas which were treated conservatively. There were 2 deaths in this series; one was due to BC (T3, triple negative young patient), and the other was due to cardiac condition. There was one axillary recurrence, this patient had negative SN by all testing modalities, and had mastectomy as a primary breast procedure, thus ALND was carried out to deal with her recurrence. There were 2 ipsilateral breast recurrences (both had breast conservative therapy as a primary breast procedure followed by whole breast irradiation), and both patients subsequently had completion mastectomy. Bone metastasis was seen in one patient 3 years after the SLNB procedure. We lost follow up of 14 patients out of 117 (11.9%).
Discussion
This is a descriptive analysis of our experience with 120 cases of SLNB in BC covering 10 years (2005-2014). The SLNB program for patients with BC at our institution started in 2005 in a multidisciplinary setting with strict inclusion criteria. The program was initiated by one of the surgeons who had formal overseas training on SLNB in BC where he attained the initial learning phase and validation of the procedure. At the beginning our program, there was a scientific evidence to support our plan of not performing axillary lymph node dissection for patients with negative SN.21-23 Sentinel lymph node biopsy in BC, a minimally invasive procedure, was first described in 1994,16 since that time, it gained a substantial ground and it is now accepted as the standard of care for axillary staging in clinically negative axilla BC patients.17-19,24
To maximize our SN identification rate, we used the dual method (radioactive tracer and patent blue dye).25-29 Our identification rate was 97.6%, which is in accordance with most of the published literatures.26,27,30
Tumor multifocality and multicentricity are no longer contraindications to perform SLNB. Current point of view suggests that there is/are specific SN(s) for the whole breast gland. It has been shown that success rates and false negative rates of SLNB in multifocal and multicentric cancers are similar to those for unifocal cancers.31-35 In the past, big tumor size was one of the limiting factors to do SLNB, but this has changed recently. Nowadays, SLNB is being performed to patients with tumor size as big as 5 cm or more as long as the axilla is clinically negative, although the chances of finding a positive SN increases as the tumor size increases.24,36,37 It has been thought before that any past surgical procedure in the breast would alter the lymphatic channels and drainage and consequently make SLNB inaccurate. This concept has been challenged and at the present time, SLNB is being carried out for patients who even had excisional biopsy for the index tumor.38-40 The number of documented cases of DCIS in KSA is low, may be one of the reasons is the absence of a national screening program for BC and the fact SCR does not register premalignant conditions. In this series, we performed SLNB in patients diagnosed to have DCIS and were high risk, or going for mastectomy or had a palpable disease.41-44
Since the introduction of SLNB in the management of the axilla in early BC patients, there has been a growing interest in the clinical significance of micrometastasis detected in the SN, but it seems now that ALND can be safely avoided in patients with early BC and limited SN involvement, as the survival outcomes are similar between patients with negative and micrometastatic axillary lymph nodes.45-48
The rationale for giving neoadjuvant chemotherapy (NAC) to patients with large operable tumors is the potential downstaging of tumors, providing the alternative of breast-conserving surgery instead of mastectomy. In patients with clinically negative axilla, SLNB following NAC is considered an acceptable option, largely based on retrospective studies demonstrating a high identification rate of SN intraoperatively and false negative rates comparable to that seen in patients who undergo SLNB prior to chemotherapy.49-52 In our series, almost 96% of patients had one to 3 SN removed at the time of SLNB. Studies have shown that the average number of SN removed at the time of SLNB is 3.53 The identification of more than one SN may be attributed to migration of isotope or blue dye from the true SN to second line nodes or just a normal anatomic variation in which the lymphatics of a given site in the breast drain simultaneously.53 We performed intraoperative FS for all the SN in this series. It allowed us to do immediate ALND for the SN positive cases which was approximately 21% of the patients in this study.
There was an agreement between FS results and H&E results, yet there were 10 doubtful cases in H&E reading, for which we performed IHC. All of the 10 cases showed micrometastasis (between 0.2 and 2.0 mm cancer deposits), 6 of the 10 cases had delayed ALND, with negative harvested lymph nodes other than the SN. Histologically, the negative SN that were re-examined with serial sectioning and IHC, detected an additional 10-16% with occult metastases. Sentinel node metastases detected by IHC did not appear to have a significant impact on 5-year overall survival.47,54
In this series, the SN was the only positive lymph node(s) in the axillary content in 74.2% of cases, which ended up by doing ALND. It is worth mentioning that 19.4% of them were micrometastasis. This issue has been looked at in the literature and there were evidences that in up to 60% of cases, the SN is the only metastatic lymph node in the axillary basin.55,56 A nomogram has been published to predict non-SN metastasis in patients with positive SN using nuclear grade, lymphovascular invasion, multifocality, estrogen receptor status, number of positive SN, tumor size, and method of detecting positivity in SN.57 However, this nomogram was not reliably predictive for positive non-SN in cases with micrometastatic positive SN plus the fact that it is not always reproducible in every center. In a recent study, ACOSOG Z0011, in which patients with clinical T1-2 N0 M0 BC having a positive SN were randomized to have ALND or no further axillary surgery, results showed no trend toward a clinical benefit of ALND for patients with limited nodal disease.19,58 In this series, we observed one axillary recurrence (1.2%) after a negative SN, which occurred 2 years from surgery. A meta-analysis of 48 studies that included almost 15,000 SN negative patients followed for a median of 34 months demonstrated an axillary failure rate of 0.3%.59 Other studies in the literature showed failure rate ranging from 0 to 1.4% at 14-46 months of follow up.60-62
In conclusion, despite the low number of patients and short follow up of this study, the obtainable results from our local experience in SLNB in BC, concur with that seen in published similar literature in particular the axillary failure rate. Sentinel lymph node biopsy resulted in minimal morbidity. A large local multicentric similar study is needed to know more about breast cancer in Saudi Arabia with special emphasis on the applicability and suitability of sentinel lymph node biopsy technique in our patients.
Acknowledgment
The author would like to acknowledge the efforts of Dr. Massouma Alnasser (Surgical resident) and Dr. Hend Alidress (Senior Surgical Registrar) in data collection.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 10, 2015.
- Accepted August 3, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.