


Abstract
Objectives: To compare pregnancy outcomes between high-order multiple pregnancies resulting from assisted reproductive technology (ART) reduced to twins and non-reduced pregnancies, and to evaluate indications for using ART.
Methods: This is a descriptive retrospective review of women with high-order multiple pregnancies reduced to twin carried out at the Department of Obstetrics & Gynecology, King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia between December 2010 and December 2013. The control group consisted of subjects with twin pregnancies who received their fertility treatment at the same hospital during the same period.
Results: One hundred and twelve women were included in this study. Of women reaching fetal viability, significantly more women delivered before the thirtieth week in the study group (50% versus 12%, p<0.004). Miscarriage/delivery prior to fetal viability, chorioamnionitis, and preterm premature rupture of membranes were statistically higher in the study group. A total of 83% of the miscarriages in the study group were in women carrying 4 or more fetuses initially, and 50% of women in the study group were multiparous with no clear indication for fertility treatment.
Conclusion: Although fetal reduction is a safe procedure, it is associated with complications. Primary prevention of high-order multiple pregnancy is recommended.
With natural conception, the rate of multiple pregnancy remain low, with less than 20% of high-order multiple pregnancies being conceived naturally, versus up to 40-60% as a result of assisted reproductive technology (ART).1 The incidence of adverse effects in high-order multiple pregnancy is directly related to the number of fetuses.2 Maternal complications are increased including preeclampsia, diabetes, cesarean section, and postpartum hemorrhage.3,4 Complications of prematurity remain important contributors to perinatal morbidity and mortality.1 The medical costs of caring for these children will be increased by many folds. This was found to have a negative impact on the parents, increasing the risk of depression, stress, child abuse, and even divorce.5,6 Primary prevention of high-order multiple pregnancy should be the aim of infertility treatment. Proper use of ovulation induction medications, close follow-up of ovarian response, canceling cycles, or reverting to in-vitro fertilization (IVF), and limiting the number of embryos transfer are recommended practices.7 With lack or failure of primary prevention, multifetal pregnancy reduction (MFPR) is an acceptable, yet painful alternative. First reported by Dumez and Oury8 in 1986, MFPR is a procedure that reduces the number of fetuses from a high-order multiple pregnancy to twins or less commonly, singleton. The reduced fetuses are structurally normal, and the ones reduced are usually the higher ones and easier to approach. The aim is to reduce the risk of miscarriage of the entire pregnancy, and severe prematurity, thus improving maternal and neonatal outcomes. This is different from selective reduction, first reported by Aberg et al9 in 1978 where anomalous fetuses are targeted.
In the Kingdom of Saudi Arabia (KSA), large family size is the norm. It is common for women to seek treatment for fertility even if they do not fulfil the criteria for infertility diagnosis. This demand has placed pressure on physicians to offer ovulation induction without clear indications, and without prior counseling of risks. A literature search was carried out on studies reported between 2003-2015 with the heading: embryo reduction, multifetal pregnancy reduction in Saudi Arabia, and none were found, although MFPR is routinely offered in a few hospitals including our center. The primary aim of this descriptive retrospective study was to compare maternal and fetal outcomes among ART, high-order multiple pregnancies reduced to twins, to ART non-reduced twins. The secondary aim was to evaluate the indications for fertility treatment. The study was approved by the hospital research advisory council and the research ethics unit. Specific ethical approval to perform MFPR was not needed as this was a retrospective study, and MFPR is standard care provided for high-order multiple pregnancy.
Methods
This study was conducted at the Department of Obstetrics & Gynecology, King Faisal Specialist Hospital & Research Center, Riyadh, KSA, a tertiary care center accepting referrals from all regions of KSA and the Gulf Countries. All women with high-order multiple pregnancies reduced to twins between December 2010 and December 2013 were included as the study group. The control group was a group of women with twin pregnancies who received their fertility treatment, and delivery in our hospital during the same time period. Exclusion criteria were cases of pre-implantation genetic diagnoses, monochorionic twins, fetal abnormalities on ultrasound, and pregnancies reduced to singletons. Extensive counseling regarding pros and cons of the procedure was provided to each couple, and written informed consent was obtained. Before the procedure, detailed early anatomy scan, including measurements of nuchal translucency and chorionicity assessment was performed and documented. The MFPR was performed trans-abdominally between 11 and 14 weeks of gestation by injecting potassium chloride into the fetal heart of the selected fetus(es) using a 20-gauge spinal needle. The needle was removed after asystole was observed. All procedures were performed by one experienced consultant under ultrasound guidance.
Data were collected from electronic and paper medical records. Missing data were completed by contacting the women by phone in a secure manner. Data was entered into a specified collection sheet into a personal computer. Statistical analysis was performed using the Statistical Package for Social Sciences for Windows version 20 (IBM Corp., Armonk, NY, USA) with the help of a professional bio-statistician. Chi-square, Fisher’s exact test, and standard deviation calculation were used as required. P-value <0.05 was considered significant.
Results
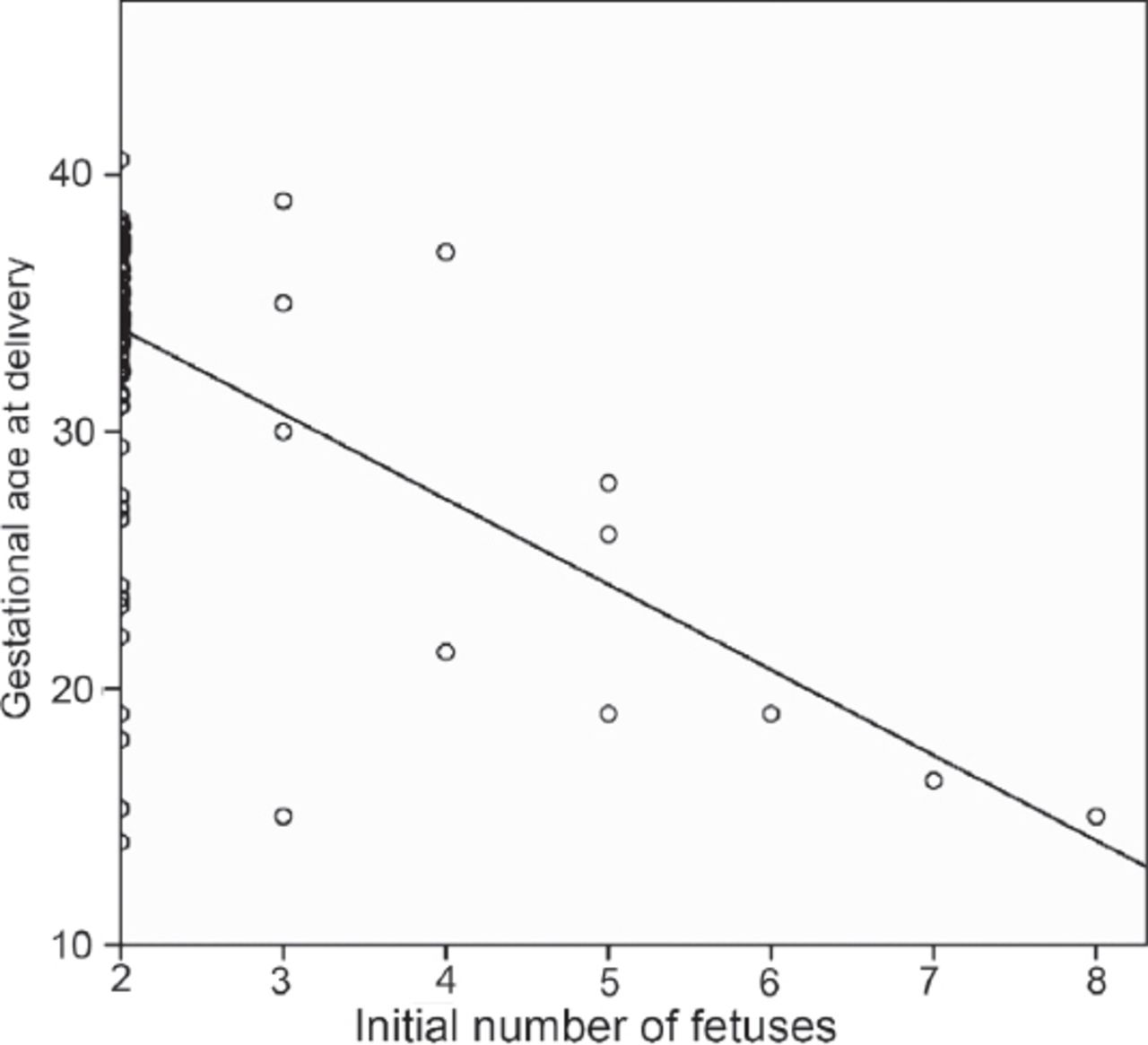
The study group consisted of 12 women who underwent the MFPR procedure, and a control group that consisted of a random sample of 100 women who conceived twin pregnancy after fertility treatment during the study period. In the control group, 90% of women were nulliparous versus 50% of women in the study group. Although this difference was not statistically significant (p=0.0604), it is noteworthy that 25% of the women in the study group were para 2 and 8% were para 5. The primary method for induction of ovulation in the study group was clomiphene citrate and human menopausal gonadotropin, which was mainly used by private, non-specialized physicians (General Obstetrics and Gynecology). There was no clear diagnosis of infertility before using ART in most of these patients. The primary fertility treatment in the control group was IVF (89%), mostly indicated by male factor. The starting number of fetuses was as follows: 4 women with triplets; 2 with quadruplets; 3 women with 5 fetuses; one woman with 6 fetuses; one woman with 7 fetuses; and one woman with 8 fetuses. Both groups were comparable with regard to mean maternal age (30 years for the control versus 27.5 years for the study group, p=0.06); body mass index (BMI) (28.5 [control group] versus 27.5 [study group], p=0.45); and previous miscarriages (0.5 versus 0.3, p=0.09). Table 1 demonstrates the pregnancy complications of both groups. Miscarriage/delivery prior to fetal viability, chorioamnionitis, and delivery before 30 weeks were statistically higher in the study group. The relation between chorioamnionitis and BMI (p=0.536), or number of reduced fetuses (p=0.80) was not significant. The preterm premature rupture of membranes (PPROM) was higher in the study group (33.3%) compared with the control group (3%). Three women in the study group had excessive bleeding necessitating blood transfusion. In the study group, 83% of the miscarriages occurred in women carrying 4 or more fetuses initially. As the initial number of fetuses increased, the risk of preterm delivery increased, and the gestational age at delivery decreased (Figure 1). Table 2 demonstrates the pregnancy outcomes of both groups. There was a significant difference between both groups regarding gestational age at delivery and birth weight for twins. When the initial number of fetuses was 3-4 fetuses, 67% of patients delivered after 30 weeks of gestation, and the risk of miscarriage before 20 weeks was 16%. When the initial number was 5 or more fetuses, all women were delivered before 30 weeks, and 4 out of 6 women miscarried at, or before 20 weeks. We had one patient each in the category of 6, 7, and 8 initial fetuses, and they all miscarried prior to 20 weeks.
Pregnancy complications in the study group who underwent the multifetal pregnancy reduction procedure and control group who conceived twin pregnancy after fertility treatment.
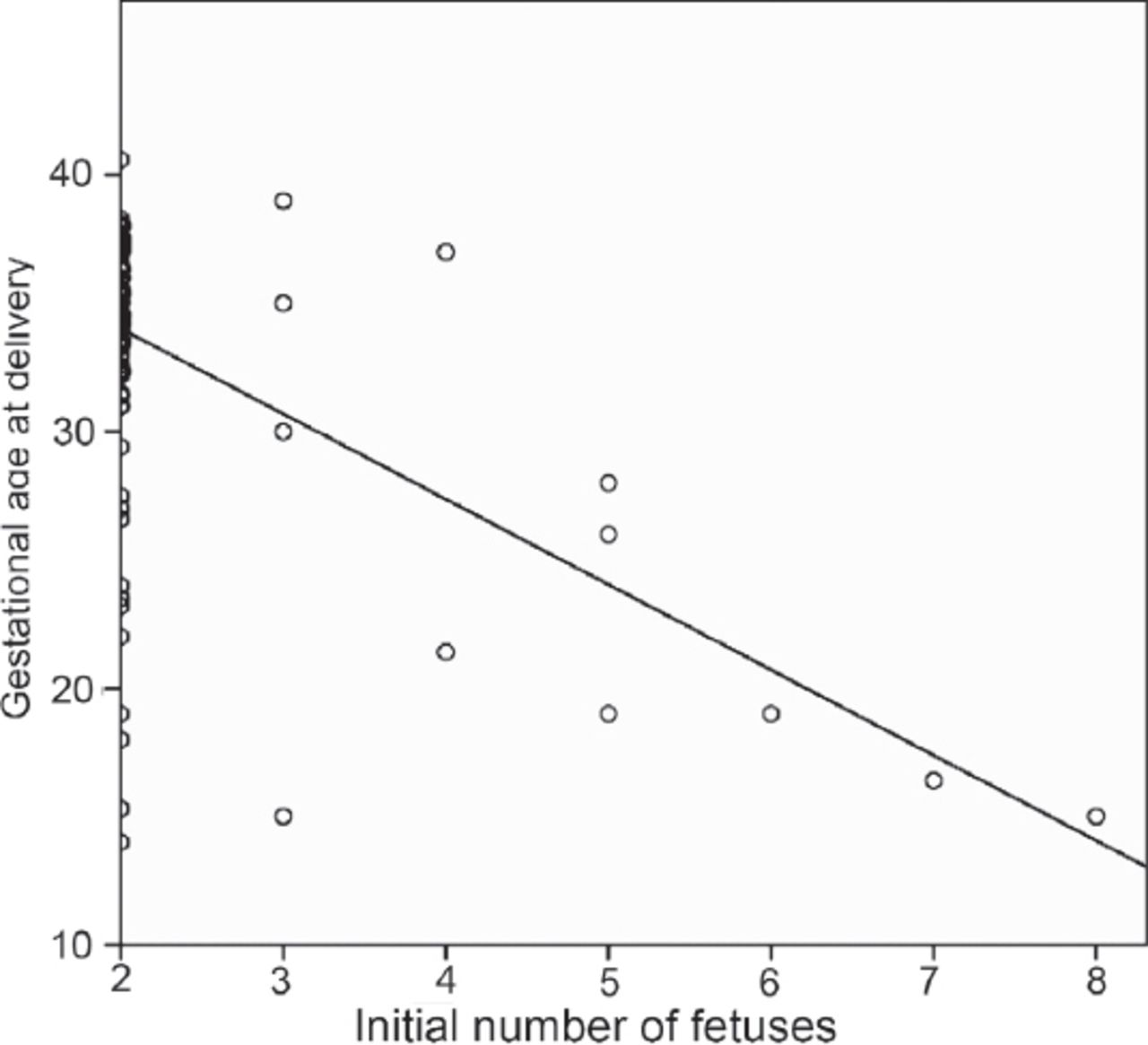
Linear regression curve demonstrating the relationship between gestational age at delivery (or miscarriage) and the initial number of fetuses.
Pregnancy outcome in the study group who underwent the multifetal pregnancy reduction procedure and control group who conceived twin pregnancy after fertility treatment.
Discussion
Multifetal pregnancy reduction as a transabdominal procedure is considered a relatively safe procedure in experienced hands. In spite of many ethical discussions regarding this topic,10 it is a widely accepted and justified procedure. However, one should not underestimate the ethical and moral dilemmas surrounding this procedure.11 There have been no published studies in KSA on MFPR, or a clear religious rule, which governs these procedures. As the aim of this procedure is to reduce the risk of prematurity complications and maternal problems related to higher-order multiple pregnancies, and thus, improve pregnancy outcome, it is not clear whether it should follow abortion laws set in countries, or new rules and regulations are required.12 Previously reported miscarriage rates following MFPR procedures have ranged between 3 and 8 percent. Our miscarriage rate within 2 weeks of the procedure was 16%, which is higher than the previously reported rates. This result could be explained by the high number of initial fetuses, which requires multiple needle introductions during the procedure, and the overall small number of patients in the study group. Studies have demonstrated better pregnancy outcomes for triplets reduced to twins than the non-reduced triplets, including lower maternal complications.13 Some studies comparing pregnancy outcomes after embryo reduction to natural twins have demonstrated similar outcomes in both groups, but most of these studies compared triplets reduced to twins,14 while others have reported worse pregnancy outcomes for the reduced pregnancies. These pregnancies also had higher complication rates (primarily higher risks of prematurity and low birth weight),13 and this was similar to our findings.
In our study, 41% of patients had a miscarriage before 20 weeks gestation. Most miscarriages occurred in women carrying 5 or more fetuses. This finding is consistent with Cheang et al15 who reported a similar observation among 372 reduced twin pregnancies, which could be explained by the effect of the starting number of fetuses on the overall pregnancy outcome. Most women in our study group were multiparous, which raises a concern of inappropriate infertility diagnosis, and use of ovulation induction. Some women received this treatment for irregular menstruation, others underwent ovulation induction without adequate medical supervision, or even counseling regarding the possible risks of high-order multiple pregnancies. In contrast, all of the women in the control group were treated in a specialized infertility unit for infertility mostly due to male factors. This is in agreement with other studies, where up to 67% of high-order multiple pregnancies resulted from ovulation induction, and not IVF.1
The limitation of our study is the small sample size, which limits the strength of our results. Some of our data was collected through phone calls, which also led to possible bias. The strength of this study is that all procedures were performed by a single operator, and that no previous similar papers were published from KSA. We are concerned with the practice of inappropriate use of ovulation induction by non-specialized physicians. We call for increasing awareness among the public and health care providers regarding the poor outcomes of such pregnancies and the associated complications. Multicenter studies are needed to appropriately evaluate the extent of the problem.
In conclusion, although fetal reduction is a safe procedure for the patient, it should not be considered a safe option for dealing with high-order multiple pregnancies. This study demonstrated an increased risk of pregnancy loss, prematurity, excessive vaginal bleeding, spontaneous rupture of membranes, and subsequent chorioamnionitis in high-order multiple pregnancies following MFPR. Primary prevention of high-order multiple pregnancies should be the primary aim of fertility treatment. Rules and regulations should be enforced among physicians using ovulation induction, and limiting the number of embryos transferred is highly recommended.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 18, 2015.
- Accepted June 24, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.