


Preterm birth is the most common cause of perinatal morbidity and mortality.1 Prolapse of the amniotic sac through the partially dilated cervical os in pregnancy is called “hourglass membranes”. The current data suggests that emergency cerclage is a good approach and associated with a longer latency period, and most often, with better pregnancy outcomes when compared with bed rest.2 However, to date, no randomized clinical trials have been conducted to demonstrate the efficacy or safety of emergency cerclages performed for advanced cervical dilatation. Treatment with prostaglandins been also suggested as a treatment.3 Prostaglandins are intimately involved in the labor pathway and facilitate myometrial contractions. Subsequent reports have suggested that indomethacin may be associated with adverse neonatal outcomes.4 In addition, indomethacin is known to promote closure of the ductus arteriosus in newborns and in fetal life, which may be reversible.5
Here we report a case of prolapsed amniotic sac “hourglass membranes” presented at late mid trimester, which was successfully treated with indomethacin therapy without the application of emergency cerclage. The patient succeeded to carry on her pregnancy to term with good outcome. A 28-year-old (para 1 and 2 miscarriages) known case of thrombophylia (positive laboratory screening after history of 2 consecutive miscarriages at 16 weeks) and history of preterm birth at 32 weeks. She presented to the antenatal care unit at our hospital with gestational age of 26 weeks complaining of fullness in her vagina.
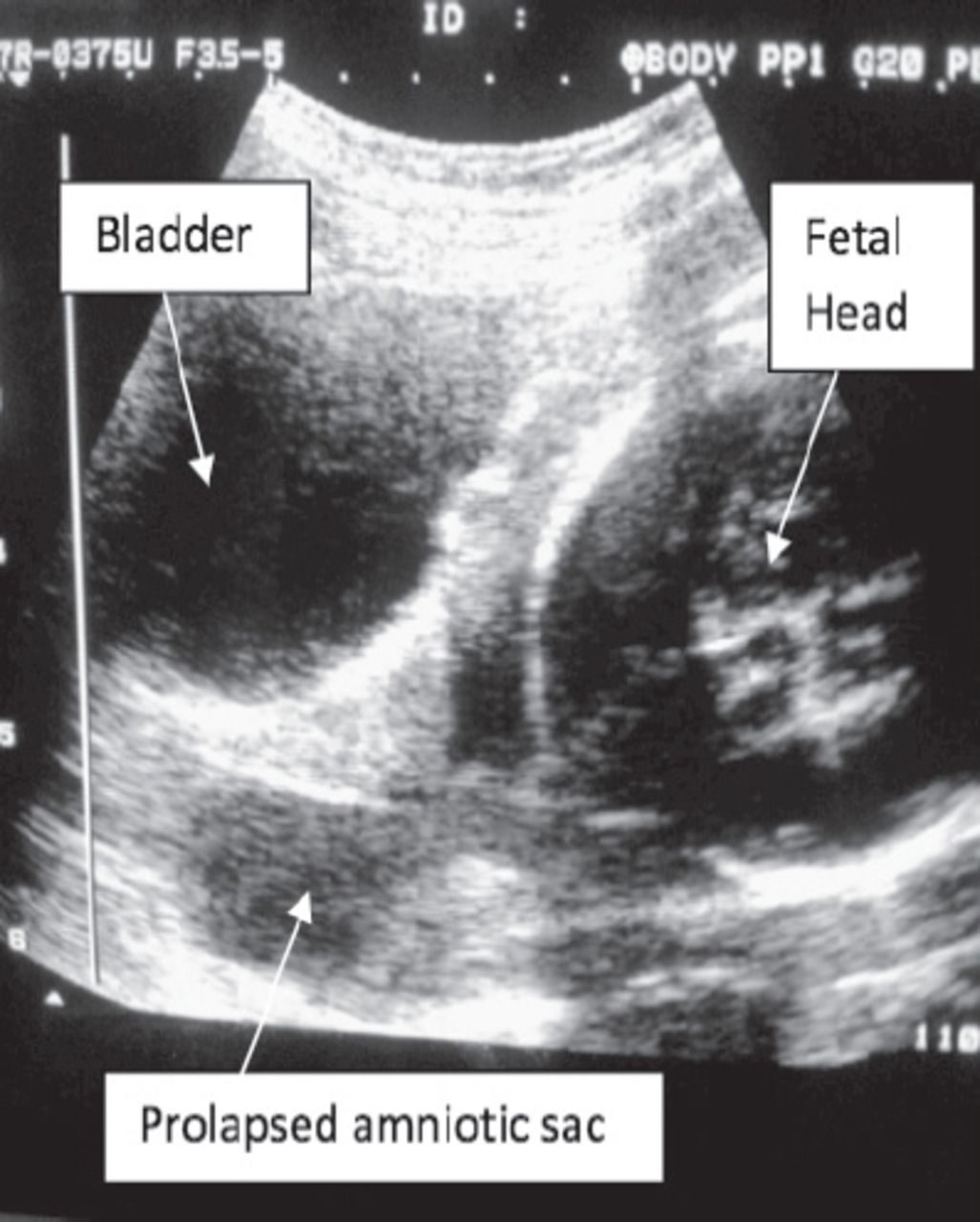
On examination, she had stable vital signs. Abdominal examination revealed abdominal symphysis/fundal height of 24 weeks in cephalic presentation with positive fetal heart beat and no uterine activities. On ultrasound scan, an alive fetus of 26 weeks in cephalic presentation with a prolapsed sac into vagina and short cervix <25 mm with no cord presentation within the sac (Figure 1) was seen, and with amniotic fluid index (AFI) of 15, and placenta was fundo-posterior. Speculum examination showed a prolapsed sac of bulging fetal membranes “hourglass membranes” in the vagina with no signs of amniotic fluid leak. She was on clexane 4000 IU subcutaneous daily, dydrogesterone 10 mg 4 times daily, baby aspirin once daily, and iron and calcium supplements. She was offered either emergency cerclage or indomethacin therapy after thorough counselling regarding risks and benefits of both options. She agreed to undergo indomethacin therapy and declined the cerclage. Twelve mg betamethasone was administered intramuscularly with an additional dose 24 hours later. Vaginal swabs revealed no infection. However, she was started on erythromycin 400 BD oral tablets. She also underwent serial U/S examinations in 48 hours intervals. After 48 hours from the start of indomethacin in a dose of 100 mg rectal suppositories, the sac disappeared from the vagina as seen on U/S scan. After 10 days, the AFI was <5 and the indomethacin therapy stopped while she continued with dydrogesterone plus anticoagulation therapies as outpatient with complete bed rest. On the fourth day after discontinuation of indomethacin, the AFI was 10 and stabilized until the end of her pregnancy. She underwent biweekly clinical evaluations, including serial U/S until 34 weeks to assess cervical length.

Trans-abdominal ultrasound scan image of prolapsed sac at presentation.
Formal biophysical profiles (BPP) began at 28 weeks, when the estimated fetal weight was 1150 g and the BPP score was 8/8 (normal range: 8-10). She underwent a fetal anomaly scan at 32 weeks, which revealed a fetus in breach presentation with no abnormalities. At 34 weeks, aspirin and erythromycin were stopped. She reached 37 weeks and elective cesarean section (as the baby was on breech presentation) was carried out with a very good outcome of a female baby, 3 kg, and normal Apgar score. Both were discharged after 3 days in good health. She had no uterine activity at all, and seems that indomethacin therapy worked through decreasing the internal pressure of the amniotic sac by reducing the amount of the amniotic fluids by reducing the urine production of the fetus by affecting the renal blood vessels resulting in oligohydramnios; thus, reforming the sac into the uterine cavity back from the vagina.
Recently, a review article6 concluded that when indomethacin was used between 28 and 32 weeks, it is more effective than placebo and other tocolytics in delaying delivery for at least 48 hours and 7 days, but not beyond 37 weeks. Even though maternal side effects are minimal, neonatal side effects are multiple, and increases when this drug is used beyond 32 weeks of gestation. It is recommended to use it for 48 hours or less, and at the lowest possible dose to allow time for corticosteroid treatment, but minimize neonatal complications.6
In conclusion, indomethacin therapy for the treatment of prolapsed amniotic sac “hourglass membranes” presented at late mid trimester, may be an option that we should be explored in further studies with larger numbers. The need for proper counseling of patients and vigilant follow up of fetal well-being by U/S scans for AFI may be of great value in such cases. Patients should have the choice of deciding what they think the best for their health issues during pregnancy. The use of indomethacin therapy in selected cases of prolapsed amniotic sac “hourglass membranes” in the second trimester may be of great benefit and safe, provided the patient receive good counselling and thorough follow-up.
Related Articles
Salih MA, Murshid WR, Seidahmed MZ. Epidemiology, prenatal management, and prevention of neural tube defects. Saudi Med J 2014; 35 Suppl 1: S15-S28.
Salih MA, Murshid WR, Seidahmed MZ. Classification, clinical features, and genetics of neural tube defects. Saudi Med J 2014; 35 Suppl 1: S5-S14.
Ulkumen BA, Pala HG, Baytur Y, Koyuncu FM. Retrospective analysis of fetal anterior abdominal wall defects. Saudi Med J 2014; 35: 1147-1149.
Acknowledgment
We would like to thank our patient who has given us consent to publish her case. We also thank Dr. Sultan Al-Nawayseh for his expert opinion on the image provided.
- Received July 28, 2015.
- Accepted October 14, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Related Articles
Cited By...
- No citing articles found.