


Abstract
Objectives: To develop and test the psychometric properties of an Arabic version of Fatigue Severity Scale (FSS-Ar) that can be used to measure fatigue in Arabic patients with disorders where fatigue is a major symptom.
Methods: Forward and backward translations of FSS were undertaken to develop an Arabic version. The validity and reliability of the FSS-Ar was then tested on 28 patients with systemic lupus erythematosus (SLE), 24 patients with multiple sclerosis (MS), and 31 healthy subjects. Exploratory factor analysis and hypothesis testing methods were used to examine construct validity. The correlation between FSS-Ar and the vitality domain of the RAND 36-Item Health was examined to test construct validity. The study was conducted at the King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia between February and June 2012.
Results: Using a score of ≥4.05 to define fatigue, 39 of 52 (75%) participants were fatigued compared with 10 out of 31 (32%) healthy participants. The correlation between the FSS-Ar and the vitality domain of the RAND-36 was acceptable (r = -0.46). Factor analysis showed that items of the FSS-Ar measured one underlying construct, namely, fatigue. Test-retest reliability and internal consistency of the FSS-Ar was acceptable (intraclass correlation coefficient model 2,1 = 0.80; Cronbach’s alpha = 0.84).
Conclusion: The Arabic version of the FSS demonstrated acceptable psychometric properties and was able to differentiate between patients with SLE or MS, and healthy subjects.
Fatigue can be defined as a subjective experience that includes symptoms, such as rapid inanition, persistent lack of energy, exhaustion, physical and mental tiredness, and apathy.1 Fatigue manifests itself as an overwhelming sense of tiredness and lack of energy that can result in significant impairment of a person’s participation in activities of daily living and work. Fatigue is a major symptom in a variety of medical disorders, including rheumatological conditions (such as, systemic lupus erythematosus [SLE], rheumatoid arthritis, ankylosing spondylitis) and neurological disorders (such as, multiple sclerosis [MS], Parkinson’s disease).2 Although fatigue is well recognized as a major symptom in various medical conditions, it has been notoriously difficult to define or study as a distinct entity.3 A number of questionnaires, including the Fatigue Severity Scale (FSS), Multidimensional Fatigue Inventory, Fatigue Impact Scale, and Visual Analogue Fatigue Scale have been developed, and used to measure fatigue symptoms. Ideally, a short, uni-dimensional questionnaire with robust validity, reliability, and responsiveness would be considered optimal to assess fatigue, particularly in the clinical setting.2 The FSS, originally developed by Krupp et al4 for use in patients with SLE and MS, has been used to measure fatigue severity in a variety of medical conditions. The FSS is a self-reported questionnaire that is simple and easy to use. It consists of 9 statements that rate the severity of the patient’s fatigue symptoms in terms of how these symptoms affect motivation, exercise, physical function, and activities of daily living.4 Reflecting on their condition over the past week, patients score each item from 1 to 7, based on the extent, to which they agree or disagree with each statement (1 = strong disagreement, 7 = strong agreement). The FSS can be scored either by obtaining a total score, or by calculating a mean score across all 9 items, with higher scores indicating more severe fatigue. The FSS has been shown to have acceptable psychometric properties with high internal consistency, good test-retest reliability, and good concurrent validity in several clinical populations, such as SLE, MS, and spinal cord injury,2,3 and has been recommended as the most appropriate tool to measure fatigue in SLE.5 The FSS is widely used in clinical practice and research, and has been translated into a number of languages.6-15 However, to date it has not been translated into Arabic, nor has its use been validated in an Arabic population. Development of an Arabic version of the FSS-Arabic (FSS-Ar) and its validation would be of great value, as it would allow clinicians and researchers to investigate the incidence and impact of fatigue associated with rheumatological and other medical conditions in Arabic speaking patients and populations. Therefore, the aim of this study was to translate the FSS into Arabic, and to test its validity and reliability in an Arabic speaking population.
Methods
The study was prospective whereby, firstly, the FSS was translated into Arabic and pilot-tested, and then its validity and reliability investigated in a sample of convenience in an Arabic speaking sample. The clinical component of the study was approved by the Ethics Committee of King Khaled University Hospital (KKUH). The study was conducted at the King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia between February and June 2012. Steps were taken to translate and pilot-test the FSS. Permission to translate the FSS into Arabic was obtained from its original author4. Cross-cultural adaptation, a process that uses both language and cultural adaptation factors to prepare a questionnaire for another setting was used to translate the FSS into Arabic.16 First, the FSS was translated from English into Arabic by a professional translator. Then, a bilingual translator, who was unaware of the original version of the FSS, translated it back into English. The original English and back-translated versions were then compared by an independent bilingual assessor to ensure consistency of the 2 versions. Based on the independent assessor’s feedback, a few minor changes were made to the Arabic version. This revised version was then pilot tested on 5 patients with SLE or MS. After completing the FSS-Ar, these patients were interviewed to ensure they had understood all of the items, and to provide feedback regarding the questionnaire. Based on their feedback, the word ‘motivation’, which was poorly understood was changed to ‘willingness to do something’. With this change incorporated, a final version of the FSS-Ar resulted, and was used in the next phase of the study.
For the validity and reliability testing, 2 patient groups in whom the prevalence of fatigue is known to be high were included in this study: patients with SLE (diagnosed by a rheumatologist using the 1982 Revised Criteria for Classification of SLE),17,18 attending the Rheumatology Clinic at KKUH, and patients with MS (diagnosed by a neurologist using the McDonald criteria)19 attending the MS Clinic at KKUH. To be eligible for participation, the patients with SLE or MS had to have been diagnosed with the disease for more than one year, and not had any relapses during the previous 3 months. Patients were excluded if they had any other major medical or psychiatric condition, or if they had taken anxiolytics or antidepressants in the previous 3 months. A sample of healthy subjects was also recruited from an outpatient waiting area at KKUH. Healthy subjects were eligible for inclusion if they did not have any condition that might cause fatigue. Written, informed consent was obtained from all participants. A protocol for data collection was followed. Descriptive data (such as, age, gender, occupation) and information related to the underlying illness were recorded based on information retrieved from medical records, or participants’ interviews. All participants were provided with a paper copy of the FSS-Ar and were requested to complete it. The FSS-Ar overall score was the mean of the 9 items with higher score indicating more fatigue. Additionally, an accepted Arabic version of the RAND-36 Item Health Survey20 was completed by all participants. The outcome measures used in this study included the FSS-Ar and the RAND-36 (also known as the 36-item Short Form Survey [SF-36]). RAND-36 is a generic, 36-item questionnaire that measures health-related quality of life over 8 domains that include physical functioning, daily activities, social functioning, vitality, and a global health evaluation. Each domain is scored on a scale of 0-100, with higher scores indicating better health.
Data were analyzed using Statistical Package for Social Sciences version 21 statistics software (IBM Corp., Armonk, NY, USA). Data from the 2 patient participant groups (such as, SLE or MS) were combined for analyses investigating the psychometric properties of the FSS-Ar. Exploratory factor analysis and hypothesis testing methods were used to examine the construct validity of the FSS-Ar. Using this method, construct validity of the FSS-Ar would be supported if factor analysis revealed mainly one major factor underlying the items of the scale, with loading of all questionnaire items (≥0.4) on that single factor indicating that the questionnaire measures mainly one construct, fatigue. For a factor to be extracted, it should have an eigenvalue of >1, and should explain ≥10% of the variance. In addition, only factors above the point of inflexion in the scree plot were extracted.21 The principal axis factoring method was used to extract the factors underlying the scale items.22 Consensus on the number of participants needed for factor analysis does not exist, but a sample size of 52 seems to be adequate to examine the structure of a 9-item scale.23-25 In addition to factor analysis, the hypothesis testing method was used to examine the construct validity of the FFS-Ar. We hypothesized that the FSS-Ar would show moderate to strong significant negative correlation (r ≥ -0.4) with the vitality domain of the RAND-36, with Pearson’s correlation coefficient used to examine this hypothesis. Correlation coefficients with an absolute value of ≥0.4 with another outcome measuring similar construct has been suggested to be sufficient to support construct validity.26 Cronbach’s alpha was used to examine the internal consistency of the FSS-Ar. Intraclass correlation coefficient model 2,1 (ICC 2,1) was used to examine the test-retest reliability of the FSS-Ar. Standard error of measurement (SEM) was used to examine the measurement error associated with repeated measurement using the FSS-Ar. True change in FSS-Ar that is beyond the measurement error was quantified using the minimal detectable change with 90% confidence intervals (MDC90). A receiver operating characteristic curve (ROC) was used to determine the optimal cutoff of the FSS-Ar that should be used to define fatigue.
Results
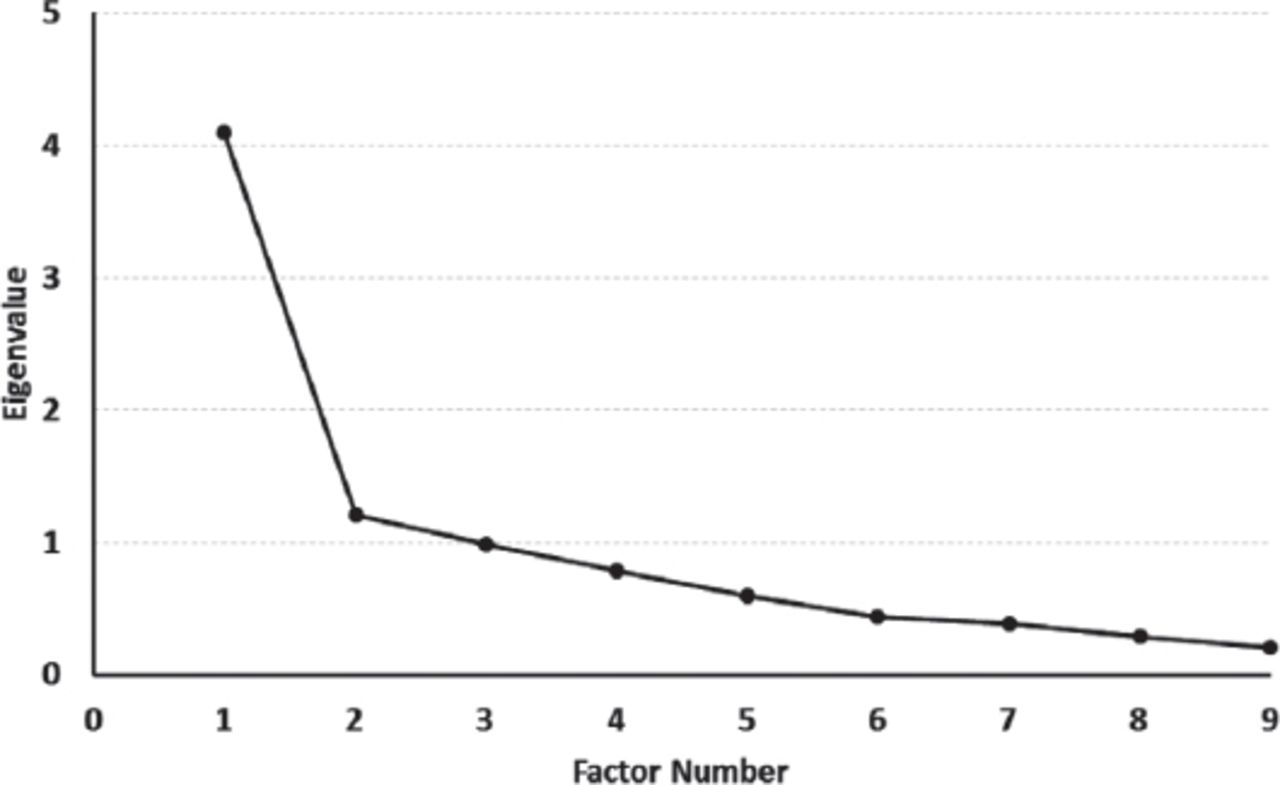
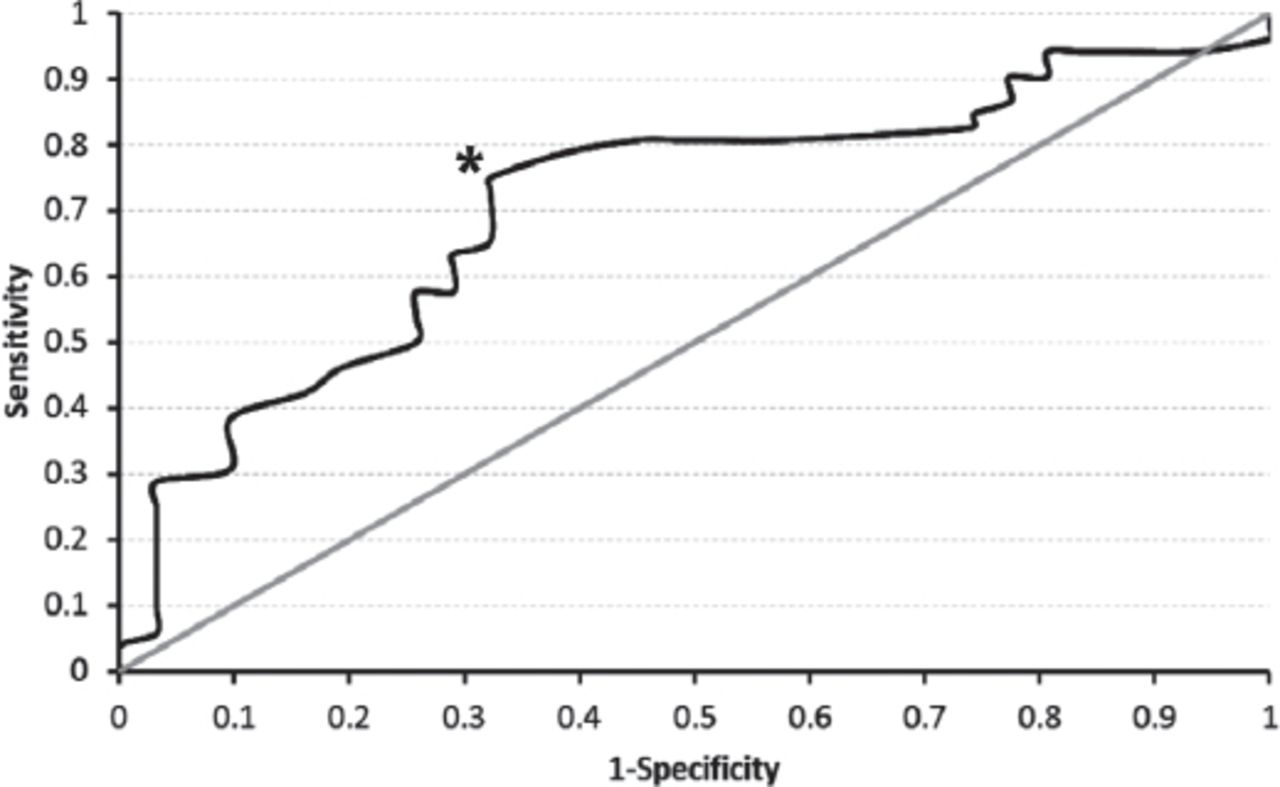
A total of 28 patients with SLE, 24 patients with MS, and 31 healthy subjects participated in the study, and are all Riyadh resident. Nineteen participants were excluded either due to having other neurological conditions, or taking antidepressants. The descriptive data of participants are summarized in Table 1. Both patient groups demonstrated significantly higher mean FSS scores than the healthy participants (p=0.005). With respect to the internal consistency of the FSS-Ar, the Cronbach’s alpha for the whole patient group was 0.84, indicating that items within the scale were homogenous and were not redundant.27 Test-retest reliability analyses, undertaken on a sub-group of 10 patient participants, demonstrated good absolute reliability (ICC 2,1 = 0.80). The SEM and MDC90 were computed based on this reliability estimate (Table 2). Factor analysis revealed 2 factors with eigenvalues >1. The first factor had an eigenvalue of 4.1 and explained 45.5% of the variance, while the second factor had an eigenvalue of 1.2 and explained 13.4% of the variance. All items had loading of more than 0.4 on the first factor while none had loading ≥ 0.4 on the second factor. Visual inspection of the scree plot (Figure 1) revealed that the point of inflexion in the plot occurred at the second factor, indicating that only one factor should be retained. Therefore, based on the three step criteria set for factor extraction used in this study, FSS-Ar mainly measures one underlying factor, namely, fatigue. The Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO) was used to examine the adequacy of the sample size used in this study to run factor analysis. The KMO statistics value was 0.77, indicating that the sample size used in the factor analysis was sufficient.23 The FSS-Ar showed a moderate negative relationship (r = -0.46) with the energy/fatigue domain of the RAND-36 supporting its construct validity. The area under the ROC curve (area under the curve [AUC]) was used (Figure 2) as a measure of the ability of the FSS-Ar to distinguish participants with SLE or MS (n=52) from healthy participants (n=31). Under the null hypothesis that the FSS-Ar score would not discriminate between patient participants and healthy participants, the AUC would be 0.5. If the FSS-Ar was able to perfectly discriminate between patient participants and healthy participants (100% specificity and 100% sensitivity) the AUC would be 1.0. An AUC of ≥0.7 or larger was considered appropriate evidence to suggest the discrimination ability of the measure.28 The point estimate for FSS-Ar AUC was 0.71 (95% CI 0.59-0.82) and this estimate of the AUC was significantly different from an AUC of 0.5 (p=0.002). Based on the results of the ROC, a FSS-Ar total score of 4.05 was determined to be the optimal cutoff point that provides the best balance between sensitivity and specificity. This score of 4.05, used as a cutoff to discriminate between patients and healthy controls, yielded 75% sensitivity and 67% specificity. When a FSS-Ar total score of ≥4.05 was used to define fatigue, 39 of 52 (75%) patient participants were classified as having fatigue, while 10 out of 31 (32%) healthy participants were classified as having fatigue (32%).
Descriptive data for all participants included in this study.
Test-retest reliability and measurement error of the Fatigue Severity Scale Arabic version (FSS-Ar).

Factor analysis scree plot showing the inflexion point at the second factor indicating that only the first factor should be retained.

Receiver operating characteristic curve used to determine the optimal cutoff of the Fatigue Severity Scale Arabic version (FSS-Ar) to define fatigue. An asterisk (*) was placed on the optimal cutoff point in the FSS-Ar that provides the best balance between sensitivity and specificity to distinguish patients with multiple sclerosis, or systemic lupus erythematosus from healthy individuals.
Discussion
In this study, an Arabic version of the FSS was developed and its validity and reliability was measured in an Arabic speaking population. We found that FSS-Ar was able to measure and quantify fatigue in a Saudi cohort. The test-retest reliability and internal consistency of the FSS-Ar were acceptable and its correlation with appropriate domains of the RAND-36 was also acceptable.
We found that the FSS-Ar had a Cronbach’s alpha value of 0.84, supporting the internal consistency of the scale and the homogeneity of the items with the scale,27 and similar to the values obtained in other studies investigating the psychometric properties of translated versions of the FSS.6-13,15 The FSS-Ar showed good relative reliability (ICC=0.8), similar to values obtained in previous studies.6,7,9,10,12 The relatively large value of MDC found in this study may reduce its clinical applicability, and suggests that another study with a larger sample size who undergo test-retesting, may be needed to establish the MDC of the FSS-Ar. The results of factor analysis in this study supports the unidimentionality of the FSS-Ar and provided evidence of the validity of the FSS-Ar since all items are intended to measure only one construct, namely, fatigue. This finding is in keeping with factor analysis undertaken with other translated versions of the FSS.7,10 The magnitude and direction of the correlation between the FSS-Ar and the vitality domain of the RAND-36 that we demonstrated (r = -0.46) provides additional evidence of the construct validity of the FSS-Ar. A higher correlation was not anticipated, as the 2 scales do not measure exactly the same constructs. Similar results were shown in other studies where translated versions of the FSS were investigated and compared with the RAND-36 or SF-36.6,7,13
This study had a number of limitations. While the sample size in this study was sufficient to examine the internal consistency and construct validity of the FSS-Ar, the overall sample size was relatively small. Thus, the results of this study should be considered preliminary, and further research with a larger sample is needed to further investigate the psychometric properties of the FSS-Ar, and to establish clinically useable SEM and MDC values, which would enhance the clinical usefulness of the scale. The ability of the FSS-Ar to detect a change in fatigue levels over time was not examined in the current study, thus, further research is required to establish the responsiveness of FSS-Ar. Future research evaluating the usefulness of the FSS-Ar for patient groups with diagnoses apart from SLE and MS where fatigue is a major symptom are required.
In conclusion, the ability to measure the prevalence and severity of fatigue in order to effectively manage patients who experience fatigue as a major symptom, such as those with rheumatological conditions, requires the use of valid and reliable measurement tools. The Arabic version of the FSS developed in this study showed evidence of internal consistency, relative test-retest reliability and construct validity, and was able to measure the presence and severity of fatigue in a sample of Arabic patients with SLE or MS, supporting its use in clinical practice and research.
Supplements
* Supplements will be considered for work including proceedings of conferences or subject matter covering an important topic
* Material can be in the form of original work or abstracts.
* Material in supplements will be for the purpose of teaching rather than research.
* The Guest Editor will ensure that the financial cost of production of the supplement is covered.
* Supplements will be distributed with the regular issue of the journal but further copies can be ordered upon request.
* Material will be made available on Saudi Medical Journal website
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received August 17, 2015.
- Accepted November 21, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.