


Clinical Presentation
A 32-year-old male, driver by occupation, presented to the orthopedic outpatient department with complaints of acute exacerbation of a chronic pain along the lateral aspect of the elbow. Pain was relieved on rest and aggravated on strenuous activities such as weight lifting and throwing objects. There was no history of trauma or infection. On clinical examination, tenderness was present along the lateral condyle of the humerus with restriction of terminal flexion and extension of the forearm. The tenderness was more prominent in compression of the radio-capitellar compartment (valgus stress test). There was no crepitation or instability of the elbow joint. An antero-posterior and oblique radiograph of the elbow was obtained (Figure 1) followed by MRI of the elbow (Figure 2) to investigate the extent and stability of the lesion.
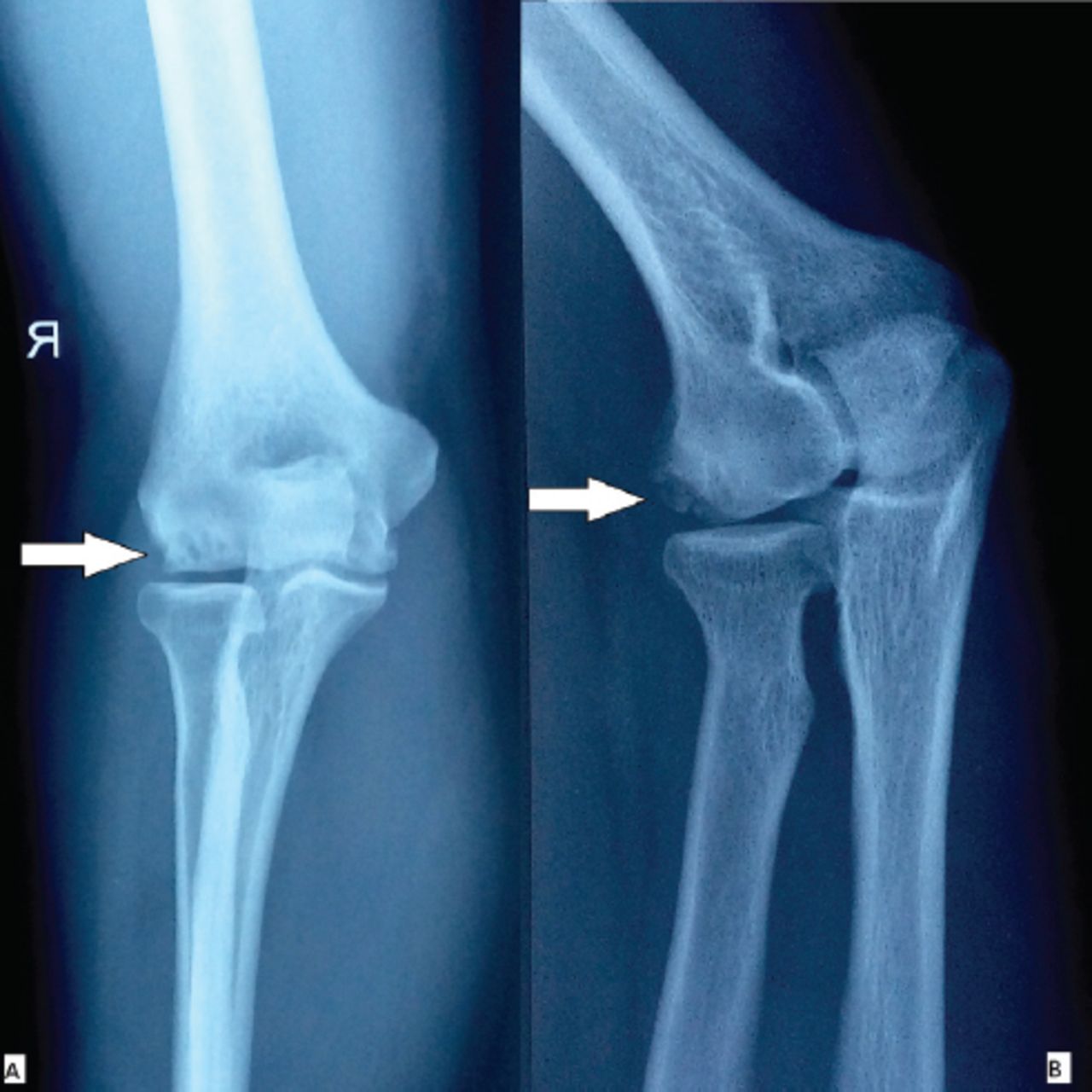
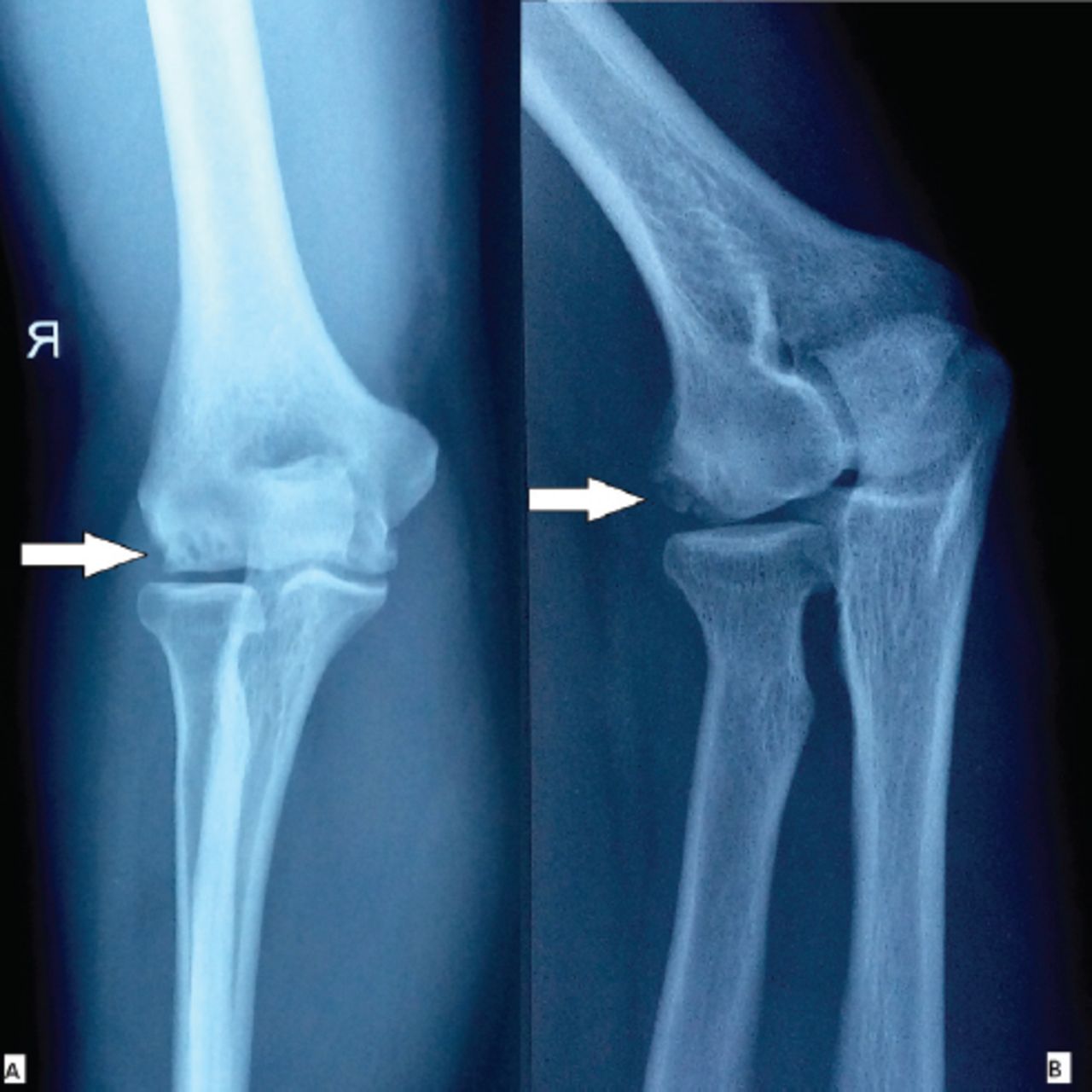
Radiograph showing the A) anteroposterior and B) oblique view of the elbow.
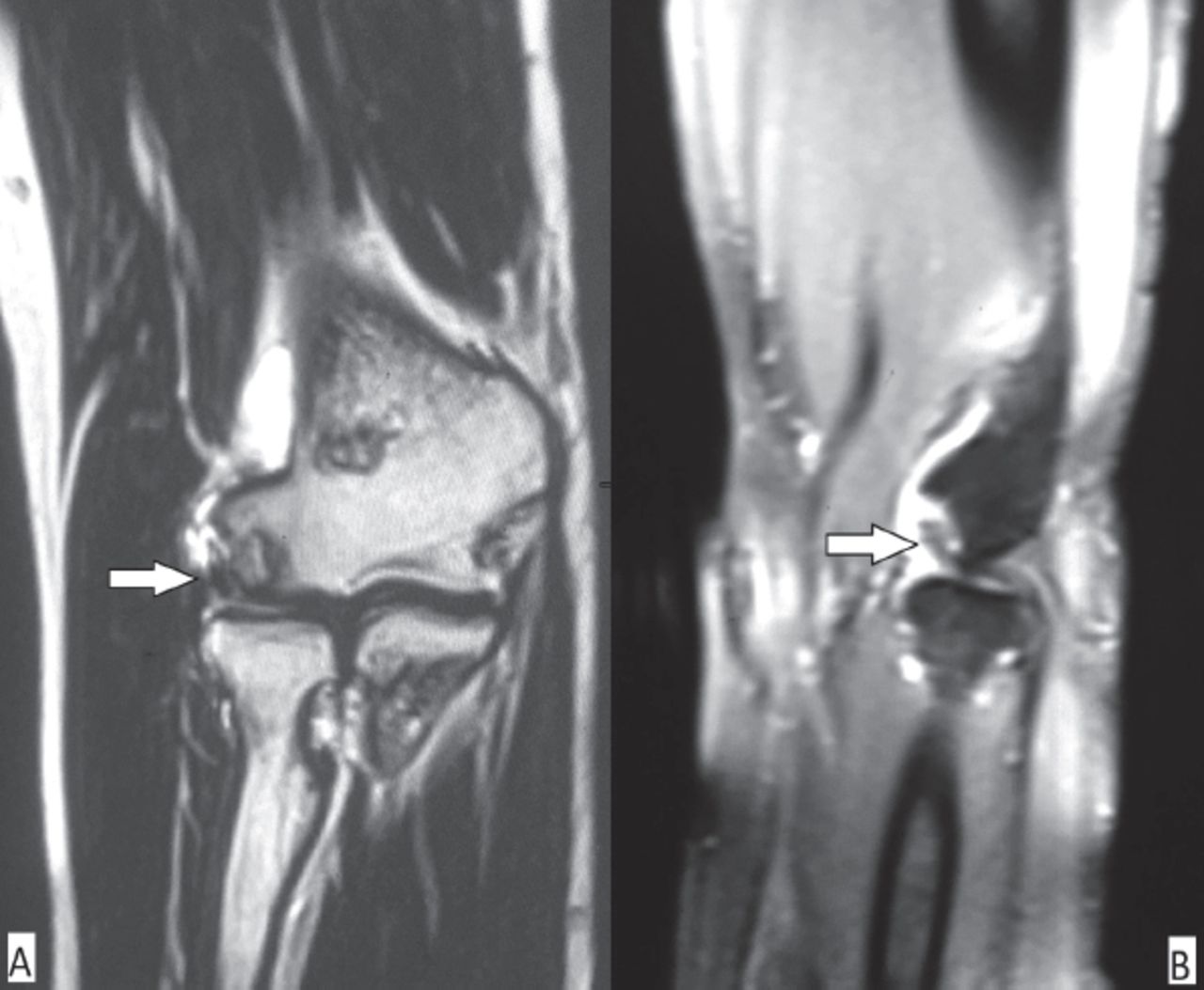
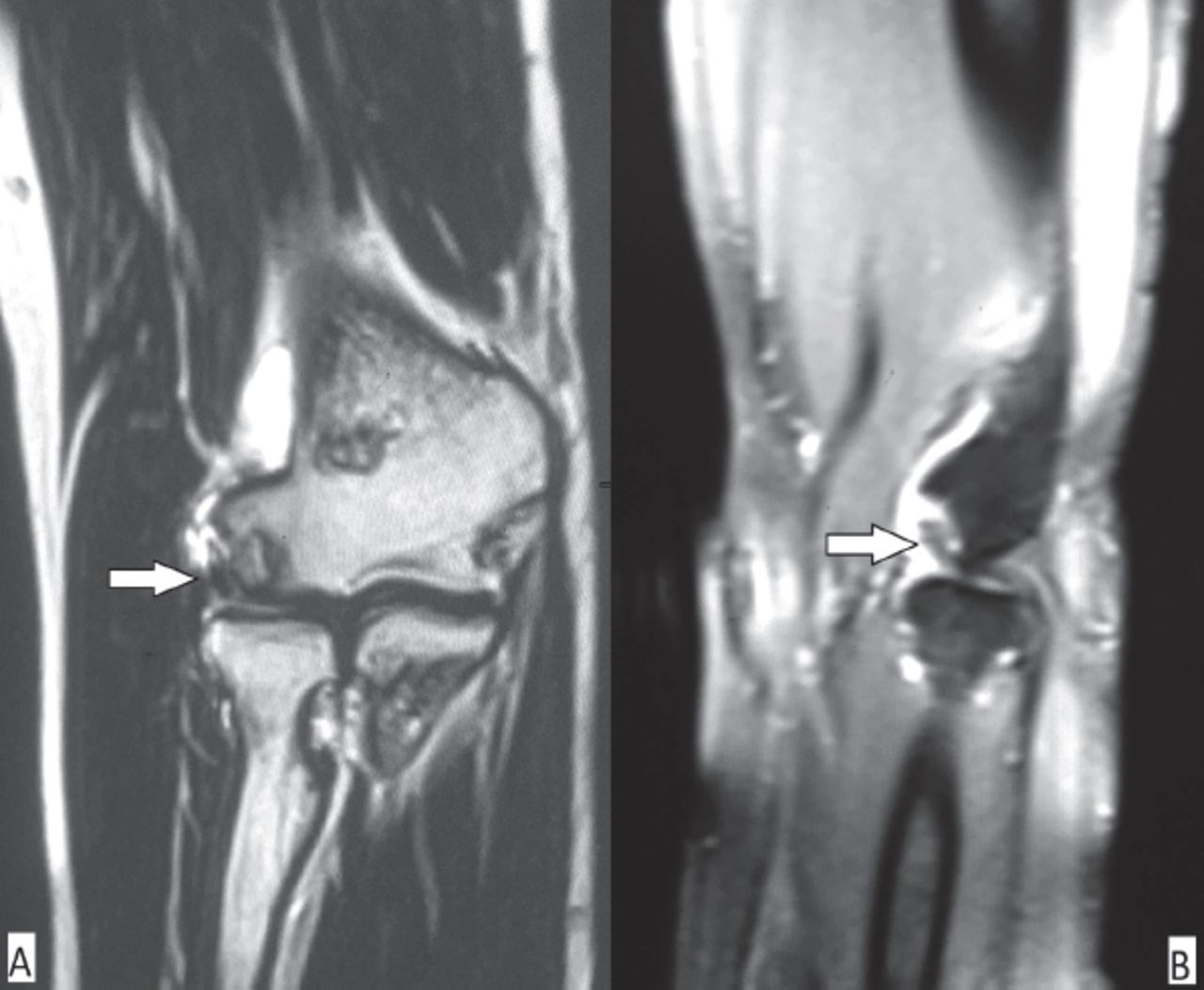
Magnetic resonance imaging showing the A) anteroposterior and B) oblique view of the elbow.
Questions
What are the findings on plain radiography and MRI?
What is the diagnosis?
Discuss the management of this condition.
Answers
The anteroposterior (Figure 1A) and oblique (Figure 1B) radiograph of the elbow joint showed few round radiopaque lesions with surrounding radiolucency (white arrow) with subtle flattening and density change along the articular surface of capitellum. On MRI (Figure 2), the Coronal T2W sequence showed (A) a hypointense lesion in the lateral articular surface with a defect in the capittelum. Also there was a mild flattening with hyperintensity within the capitellum. On sagittal proton density (PD) fat sat (Figure 2B), there was a hyperintense lesion in the lateral articular surface of capitellum with surrounding hyperintensity giving the rim sign. Post contrast, there was enhancement of the capitellum with no enhancement of the lesion.
Clinico-radiological diagnosis: unstable osteochondral defect of the capitellum.
Arthroscopic debridement with drilling.
Discussion
Osteochondral defect (OCD) is one of the entities in the wide spectrum of osteochondral lesions of bone. There is no consensus on the etiology of OCD. The cause appears to result from direct repetitive micro trauma, overuse (in athletes), or secondarily from loss of blood supply to the subchondral bone. The most common location for an OCD is the knee joint followed by the ankle and elbow joints. The role of imaging in osteochondral injury is first to diagnose the abnormality, and then characterize it according to the extent of involvement, stability of the lesion, and any associated complications. Magnetic resonance imaging is the most sensitive and reliable imaging technique for the assessment of osteochondral lesions, but plain radiography is usually the first imaging that was carried out.1 The diagnosis of OCD is made on 2 standard views; plain radiograph of the involved joint with oblique views taken if necessary. Osteochondral defect is seen as a focal radioopaque lesion with perilesional radiolucency disrupting the subchondral cortical line. Fragmentation of the articular surface and presence of articular bodies suggest an unstable lesion on plain radiography.
The diagnosis is suggested on MRI by identifying signal changes, or morphologic changes at the articular surface. The presence of a focal articular surface defect with high signal intensity between the lesion and normal bone on fluid sensitive sequence indicates an unstable lesion on MRI. These findings can be noted in our case on T2W and PD sequence images (Figure 2). The unstable lesion identified on MRI can remain attached, or can detach and appear as a separate displaced articular body, usually adjacent to the defect. In such cases, MR arthrography can improve the staging accuracy for osteochondral lesions.2
Treatment for an osteochondral defect depends on the status of the articular surface and underlying bone. The aim of treatment should be to achieve painless range of motion and to preserve chondral integrity. Conservative treatment in the form of an extended period of rest with non-steroidal anti-inflammatory drugs; active physiotherpy is reserved for patients with a stable and viable lesion. The success rate of nonoperative treatment for stable lesions is 50%.3 A spectrum of surgical treatments are available for patients with failed conservative treatment, and unstable or nonviable lesions. Surgical options ranges from arthoscopic debridement to osteochondral autograft transfer. Other surgical options include internal fixation of the fragment using bioabsorbable screws if the size of the fragment is enough for screw purchase, debridement of the nonviable fragment with microfracture of the underlying subchondral bone, or the use of an osteochondral graft.4 Very little literature is available, which suggests that the preferred treatment is arthroscopic debridement with, or without drilling.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.