


Clinical Presentation
A 4-year-old female child presented in the Emergency Department of Dallah Hospital, Riyadh, Kingdom of Saudi Arabia with a 24 hours history of foreign body ingestion associated with 2 episodes of hematemesis. The patient’s general condition was normal with stable vital signs. Antero-posterior x-ray of the chest and abdomen was carried out; however, no radiographic evidence of any radio-opaque foreign body was seen. Barium swallow was advised considering suspicion of a radiolucent foreign body (Figure 1A & 1B). Immediate esophagoscopy was performed using a flexible endoscope and a 2.5 cm star shaped plastic toy was removed from the upper oesophagus. No immediate post-operative complications were seen. Patient was discharged in stable condition the same day (Figure 2).

X-ray showing: A) barium swallow study showing a well-defined star shaped foreign body coated with barium (arrow). B) computer tomography scan of neck at the level of cervico-thoracic junction (arrows).
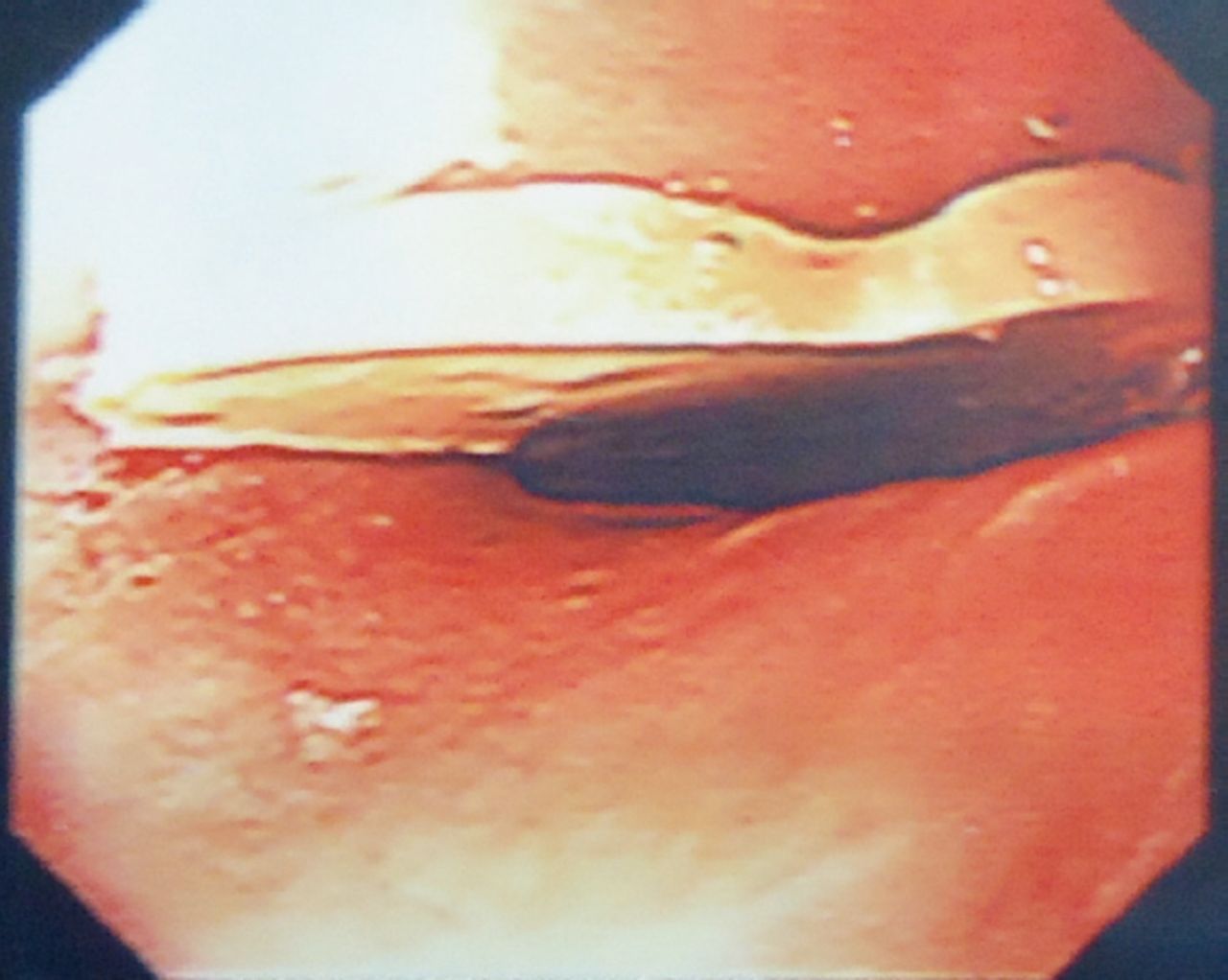
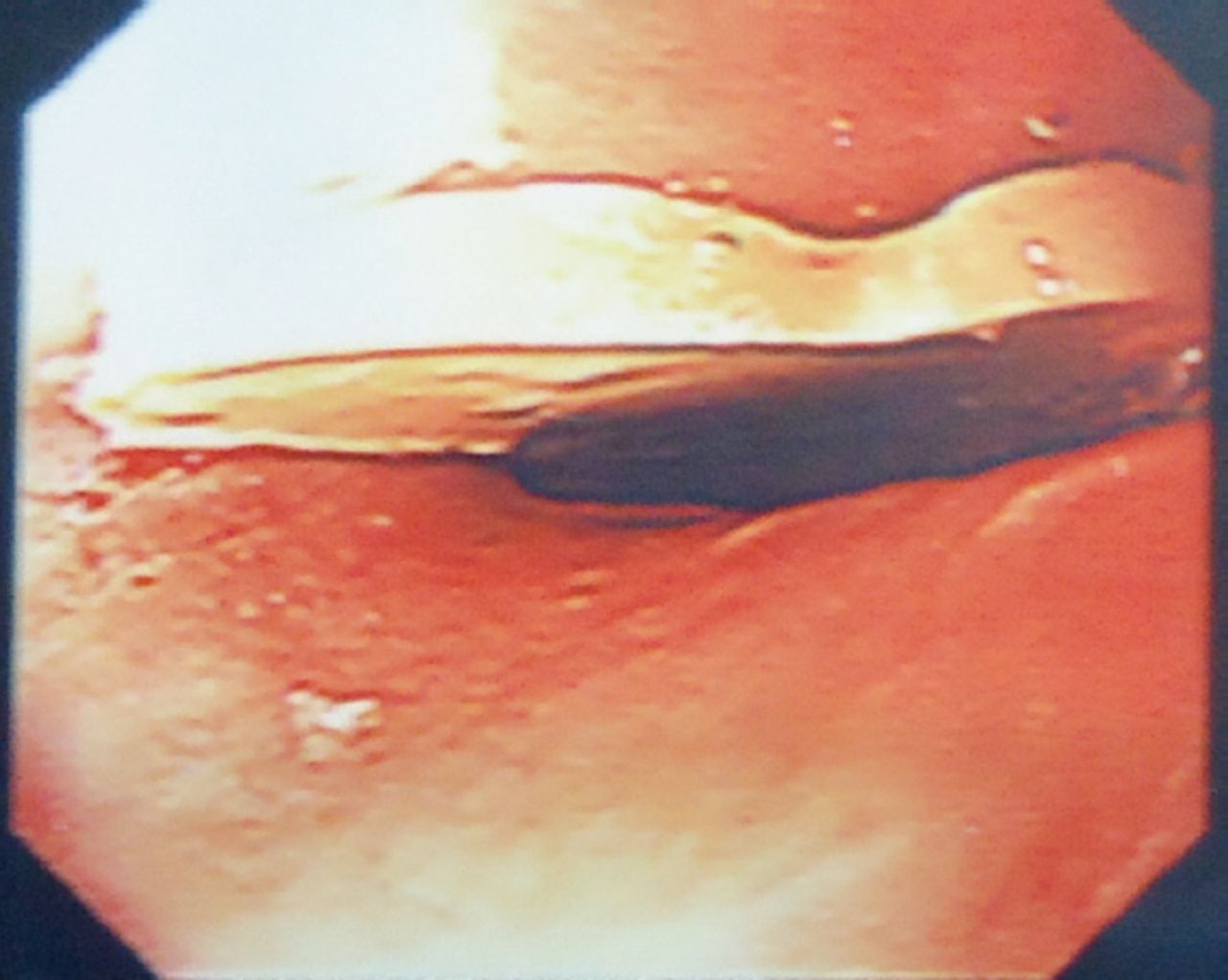
Endoscopic picture showing a star shaped plastic toy.
Questions
What are the findings on barium swallow study?
What are the findings on the CT of the neck?
What is the diagnosis?
Answers
Barium swallow study showing a well-defined star shaped foreign body coated with barium visualized in the upper oesophagus at the level of C6 through T1 vertebrae with mild transient obstruction to the flow of contrast.
A computer tomography scan of the neck at the level of cervico-thoracic junction revealed impacted oesophageal foreign body.
Impacted oesophageal foreign body.
Discussion
Foreign bodies usually pass through the oesophagus and the rest of the gastrointestinal tract uneventfully. Literature shows that endoscopic retrieval of foreign bodies are required in only 20% of the cases.1
Children are more prone to ingest or inhale foreign bodies. Impacted foreign bodies however, pose more threat, ranging from local inflammation, bleeding, scarring obstruction, and finally perforation. Most commonly ingested objects include coins, pins, and toys; however, food related foreign bodies, including bones, meat bolus, and nuts are also common.2 Presenting complaints include dysphagia, diffuse chest pain, vomiting, and coughing. In pediatric foreign body ingestion, history is usually not available or not helpful, which can lead to a delay in the diagnosis ending with complications. A multidisciplinary approach with a team, including a gastroenterologist, radiologist, and an otorhinolaryngology surgeon should be included for prompt management.3
Three sites of anatomical narrowing prone for oesophageal foreign body impaction are; cricopharyngeal ring, arotic arch narrowing, and lower oesophageal sphincter.4 The foreign body in our patient was impacted in the upper oesophagus where flexible endoscopic treatment is considered difficult.
Radiological assessment has a pivotal role in the diagnosis of oesophageal foreign bodies. Plain x-ray of neck and chest are first-line of investigation, however, if the foreign body is radiolucent, barium swallow is considered the imaging modality of choice. Finally, CT scan is not only used to confirm the presence of oesophageal foreign body, but also details the possible associated complications. In our case, the x-ray of the chest and upper abdomen was unremarkable because the foreign body was radiolucent. Barium swallow suggested presence of a foreign body. The delayed spot film taken in our case also raised the importance of barium study as it clearly revealed a barium coated foreign body in the upper oesophagus. As the foreign body was ingested more than 24 hours ago, a CT scan was carried out to check for possible associated complications.
Longstanding esophageal foreign bodies may cause weight loss or recurrent aspiration pneumonia, due to decreased caloric intake and mishandling of oral secretions. They can also damage the mucosa and lead to strictures, or erode the esophageal wall, creating a fistula with the trachea or other nearby structures. Sharp objects may perforate the esophagus, resulting in neck swelling, crepitus, or pneumomediastinum.3
Treatment of oesophageal foreign bodies not only depend on patient’s age and general condition, but the type, size, shape, and impacted site of the foreign body also plays an important role in deciding the treatment option. Endoscopy is considered to be the gold standard in retrieving foreign bodies with a reported positive extraction in 83% of the cases. Both rigid and flexible endoscopic extraction can be used, however, in case of sharp objects, the earlier is the method of choice. The failure of endoscopic approach leads to laparoscopic and other surgical maneuvers.5 The flexible endoscopy was successfully used to remove the ingested plastic toy in our case.
In conclusion, accurate diagnosis and early treatment of pediatric foreign bodies ingestion and oesophageal impaction are important key steps for decreasing associated morbidity. Barium study and complementary CT are important in cases with suspicion of a radiolucent foreign body.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.