


In the practice of infectious diseases, we are reminded daily that the presentation of illness and associated symptomatology can vary from one individual to another despite the identical causative pathogens. This variability reflects an amalgamation of several factors including comorbid diseases as well as genetic polymorphisms. Personalized medicine builds on the concept that we all harbor unique biological variables that orchestrate our response to disease and leverages these differences for the purpose of improved diagnostics and therapeutics. To date, the best studied application of personalized medicine is the field of oncology. Personalized cancer therapy is now common vocabulary and we can find opinion articles in the lay press that focuses on the innovation of personalized medicine for specific malignancies.1 In 2016, literature searches using key terms including “personalized” or “precision” and “cancer” yielded approximately 10,000 articles. A personalized approach to malignancy has been successful and more academic centers have integrated precision methods in their routine care of cancer.
In the United States, the call to launch personalized or precision medicine (both terms are often used interchangeably) for the general population use has come from high ranking leadership. In January 2015, President Barack Obama announced a Precision Medicine Initiative as part of his State of the Union Address.2 One month later, the director of the National Institutes of Health (NIH) authored a perspective piece in the New England Journal of Medicine supporting a personalized approach to disease therapeutics.3 The main focus and centerpiece of these initiatives is malignancy. That said, other diseases are amenable to a very similar approach, including infectious diseases.
There is strong evidence that a precision medicine approach in infectious diseases would be quite effective. In fact, the evidence stems from our daily practice of infectious diseases; why do some individuals present with lepromatous versus tuberculoid leprosy? Why do certain human immunodeficiency virus (HIV) infected individuals spontaneously control infection to very low viral loads such as elite controllers? Why do some individuals reactivate herpes family infections such as cytomegalovirus (CMV) with devastating outcomes while others maintain herpetic latency? Even in our immunocompromised patient population, we experience dramatic breadth of clinical infectious complications. For example, in the leukemic population, we continue to measure approximately an 8% rate of invasive fungal disease;4 why do certain patients, with seemingly similar and identical risk factors, develop fungal complications, yet others do not?
As we formulate treatment plans for our patients, we wonder about unmeasured variables that may exist in the individuals before us; will our patient respond to the treatment we are proposing? Can they afford to suffer a clinical treatment failure? What are the factors that allow one patient to control infection, but another to fall gravely ill? Inherent to these issues are 2 key variables, the pathogen and the host. Over decades, we have invested a significant amount of research effort in the pathophysiology of many pathogens and while we have more to learn, equal focus must now be placed on host immunity. The advances of genetic sequencing have provided us with illustrative cases to rationalize some of the unique clinical differences. Certain genetic polymorphisms essential for pathogen recognition by immune cells have been shown to result in aberrant immunity that clinically result in severe infections within kindred family members; recurrent fungal infections in the setting Dectin-1 and CARD9 polymorphisms are such examples.5 Identifying genetic polymorphisms is an excellent “first-step” towards dissecting the intricacies of host immunity. However, to address the full complexity of these host-pathogen systems, we need to return to basic translational research and adopt an unprejudiced, systematic approach, which allows us to decode these networks in a clinically meaningful manner.
Through the spirit of international collaboration, several projects sponsored between the King Faisal Specialist Hospital and Research Centre (KFSHRC) and the Massachusetts General Hospital (MGH)/Harvard Medical School (HMS) take unbiased research approaches to address infectious complications in the growing immunocompromised patient population. We will briefly discuss 3 of these projects that are actively ongoing between both our institutions.
In 2015, the Fungal Immune Reserve (FIRE) trial was launched to define the fungal immune reserve in high-risk leukemic patients undergoing hematopoietic stem cell transplantation. The scientific strategy collects immunological data derived from individual patients through ex-vivo assays. Algorithms based on cytokine profiling as well as whole genome expression will be used to predict the risk of invasive fungal disease, ideally prior to the onset of chemotherapy. The leukemic and bone marrow transplant populations are heterogeneous with some patients possessing more anti-fungal immune reserve than others.4 A personalized medicine approach stratifying those patients with the lowest fungal immune reserve and at highest risk for invasive fungal infection will allow healthcare providers to adopt a more rational and effective preemptive treatment and surveillance strategy in order to avoid the morbidity and the unacceptable mortality rate of fungal disease. That said, we strongly believe that this approach can be adopted for many types of infectious complications ranging from viral, bacterial or parasitic (Figure 1).

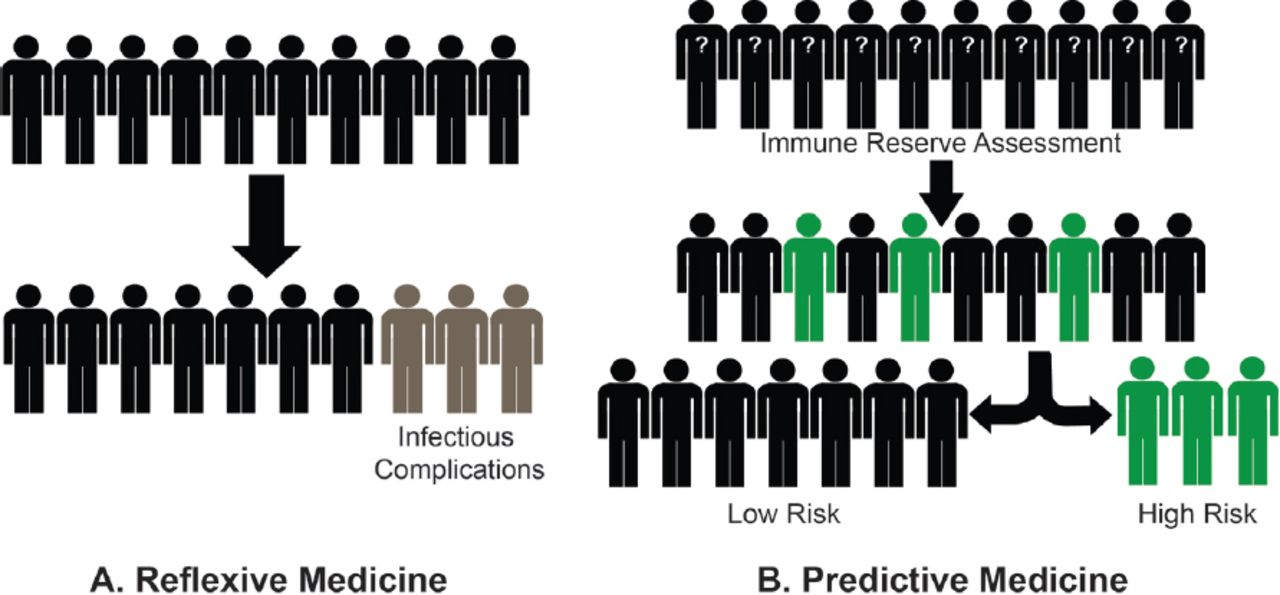
Personalized infectious disease approach in high risk patients. Panel A. The current state of practice: Reflexive medicine. Patients undergoing immunomodulating therapy are monitored for infectious complications. Once an invasive infection is identified, treatment is initiated, although significant delay occurs to essential, life-saving chemotherapy or transplantation with higher burden of morbidity and mortality. Panel B. Future approach using personalized medicine: Predictive medicine. The ability to measure immune reserve prior to immunomodulating treatment identifies patients with low reserve and at highest risk for infectious complications. More intensive surveillance and prophylactic strategies can be designed specifically for this pre-identified population. In addition, adjustments in immunosuppressive regimens can be factored, thus reducing the morbidity and mortality as patients undergo treatment for their underlying disease.
In the same vein, a second collaborative study aspires to determine the quantitative “depth” or intensity of pharmacologic immune suppression in solid organ transplant recipients. Transplant patients typically require a lifelong regimen of immunosuppressive drugs to prevent rejection of their grafted organ. Unfortunately, these immune suppressive drugs also render them vulnerable to infections. The aim of this project is to define and determine the variables required to accurately measure the degree of pharmacologic immune suppression and subsequent risk for infection.
A third program investigates predictive modelling to guide therapy in infectious diseases. Using HIV-infected individuals, this evidence-based quantitative frame evaluates candidate strategies based on samples of “virtual” patients to identify the most promising designs. This modelling simulation approach can be translated into a system of differential equations whose solution characterizes the disease “state” at any point in pathogenesis. Through this form of translational research, we will be able to use mathematical algorithms to predict outcome of therapies, potentially avoiding the morbidity of clinical failure.
These studies serve as examples, the beginning steps, towards understanding the complex intricacies that govern host immune responses. The questions posed by these studies start to decipher the essential variables in host immunity by building a map from which we can design smarter diagnostics and predictive algorithms. Through deeper understanding of host immunity, not only will we be able to 1) identify those at higher risk for infection, 2) predict individuals who will have poorer outcomes with immune modulating therapy, and 3) determine who is destined for therapeutic failure therefore allowing healthcare providers to adjust therapy in time, but we may also see the rise of immunotherapeutics tailored specifically for infectious diseases. In an era where T cells can now be genetically fitted for specific chimeric anti-tumor targeting receptors (Chimeric Antigen Receptor, also known as CAR-T cells), why not expect CAR-T cells specific for infectious pathogens? In fact, the first generation of CAR-T cells specific for HIV have already been described and show a modest reduction in viral load indicating anti-viral activity.6 Should additional cellular therapies be developed for other high disease burden pathogens? The answer to this question will require additional foundational research similar to that being described here.
One thing is clear, as we embark into an era of increasing antimicrobial resistance coupled with the routine use of advanced immune modulating agents delivering deep, potent immune suppression, the role of personalized medicine to better understand the clinical outcomes of infectious complications becomes more critical. Efforts to fund and support this nature of clinical and translational research is imperative. Finally, research into personalized medicine will serve as the foundation to develop cellular and immunotherapies specific for infectious pathogens.
Footnotes
Disclosure. This study was supported, in part, by the National Institutes of Health (NIH), National Institute of Allergy and Infectious Diseases, Bethesda, Maryland, United States of America (Grant# K08AI110655 to M.K.M.).
- Received September 20, 2016.
- Accepted October 19, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Related Articles
Cited By...
- No citing articles found.