


Abstract
Objectives To investigate barriers related to prenatal care utilization among women.
Methods Data was collected in both English and Persian databases. English databases included: the International Medical Sciences, Medline, Web of Science, Scopus, Google Scholar. The Persian databases included: the Iranmedex, the State Inpatient Databases (SID) with the use of related keywords, and on the basis of inclusion-exclusion criteria. The keywords included are barrier, prenatal care, women, access, and preventive factors. OR and AND were Boolean operators. After the study, articles were summarized, unrelated articles were rejected, and related articles were identified. Inclusion criteria were all published articles from 1990 to 2015, written in English and Persian languages. The titles and abstracts are related, and addressed all subjects about barriers related to prenatal care utilization. At the end, all duplicated articles were excluded. There were no restrictions for exclusion or inclusion of articles. Exclusion criteria were failure in reporting in studies, case studies, and lack of access to the full text.
Results After searching various databases, 112 related articles were included. After reviewing articles’ titles, 67 unrelated articles and abstracts were rejected, 45 articles were evaluated, 20 of them were duplicated. Then, the qualities of 25 articles were analyzed. Therefore, 5 articles were excluded due to not mentioning the sample size, mismatches between method and data, or results. Total of 20 articles were selected for final analysis. Prenatal care utilization barrier can be divided into various domains such as individual barriers, financial barriers, organizational barriers, social, and cultural barriers.
Conclusion To increase prenatal care coverage, it is necessary to pay attention to all domains, especially individual and financial barriers.
Health care is continuous care from childhood to adulthood and prenatal care is one of the care chains.1,2 Prenatal care has been identified as services before birth and performed in various forms by different providers in the world.2 According to the World Health Organization, prenatal care includes integrated approaches to medical care, psychological and social support and its optimal conditions start before pregnancy and continues after birth. This comprehensive program includes: early detection of pregnancy, the first visit for prenatal care and follow-up visits after childbirth.3 The purpose of antenatal care during pregnancy and after delivery is the healthy birth without harm to the mother’s health.4 The World Health Organization emphasized that prenatal care in achieving the Millennium Development Goals (reduction of child and maternal mortality) plays an important role, also said that all women should have access to proper care during pregnancy until 2015.5 Since the maternal and child health promotion is Millennium Development Goal, the estimates of maternal mortality by international agencies of the United Nations shows the reduction in maternal mortality in all over the world, but it seems that the speed of the progress in achieving the Millennium Development Goals has been inadequate.6 During 2013, Approximately 800 women in the world died daily due to complications of pregnancy and childbirth. The risk of women’s death in a developing country due to complications of pregnancy and birth is 23 times higher than a developed country.7 At a global rate, 83% of pregnant women who are living in the developing countries have received prenatal care only once.8 Women living in developed countries received more prenatal care than those who are living in the developing countries.9 Access barriers, inequitable and low coverage of health services in developing countries include political, financial, operational, and socio-cultural barriers.10 Health care is one of the largest service sectors.11 There is no accepted definition of access to health care.12 Access to health services means the appropriate use of individual health services to attain the best health consequences.13 Access barriers to health services can be divided into 2 categories: supply and demand barriers. Effective factors on demand barriers are the inability to use health services on individuals, family or society, while the supply barriers involve inherent aspects of health system which can prevent the use of services by individuals, families and society.14,15 Low-level access may be due to lack of awareness, information, resources, facilities, health care providers, and cost of services. Costs can include the cost of supplies, medicine and transportation. In many cases, the family will be poor because of the cost.16,17 Affecting factors on supply and demand of health services include demographic characteristics, gender distribution, age pyramid, population growth rate, disease incidence, health policy, health insurance expansion, GDP, per capita income, science and technology development, medical and cultural characteristics.13,18 In the review articles, the latest scientific information is evaluated. The purpose of these articles is not only to gain information but also to evaluate and interpret them. Systematic review helps the readers to make decisions about agreements and disagreements and, if necessary, refer them to key resources in articles for more information.19 Based on our review, there was no written systematic review about the present title. Due to the importance of prenatal care utilization by women, and the outcomes of not using it, which may cause maternal and child mortality, the purpose of this study is to investigate barriers related to utilization of prenatal care services among women.
Methods
This study is a systematic review of data collected in both English and Persian databases. The English databases are International Medical Sciences, Medline, web of science, Scopus, Google Scholar. The Persian language databases are Iranmedex, SID with the use of related keywords and on the basis of inclusion-exclusion criteria. Keywords include: “barrier”, “prenatal care”, “women”, “access to healthcare” and “preventive factors”. Boolean operators were OR and AND. After study, articles were summarized, unrelated articles were rejected and related articles were identified. Search was performed by three researchers independently from April to August 2015. Inclusion criteria were all published articles from 1990 to 2015, which were written in English and Persian languages, the titles and abstracts are related, and addressed all subjects about barriers related to prenatal care utilization. And, at the end, all duplicated articles are excluded. There were no restrictions for exclusion or inclusion of articles. Exclusion criteria were failure of reporting in studies, case studies and lack of access to the full text. Studies, which did not meet criteria, were excluded after the search. Exclusion criteria were unrelated topics or availability of abstracts only. To analyze the standard reporting of quantitative article, STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist was used and COREQ (Consolidated criteria for reporting qualitative research) checklist was used for qualitative articles.20,21 The papers that were selected were those whose quality was confirmed by these checklists. The risk of bias was determined independently by two external observers using the Newcastle-Ottawa Scale.22 To assess the risk of bias in studies, Newcastle Ottawa scale was used. This checklist was used in case-control, cross-sectional and cohort studies. Maximum point in Newcastle Ottawa scale is 9. In our assessment, if the study had 7 points or more, it would be considered highly qualified.
Results
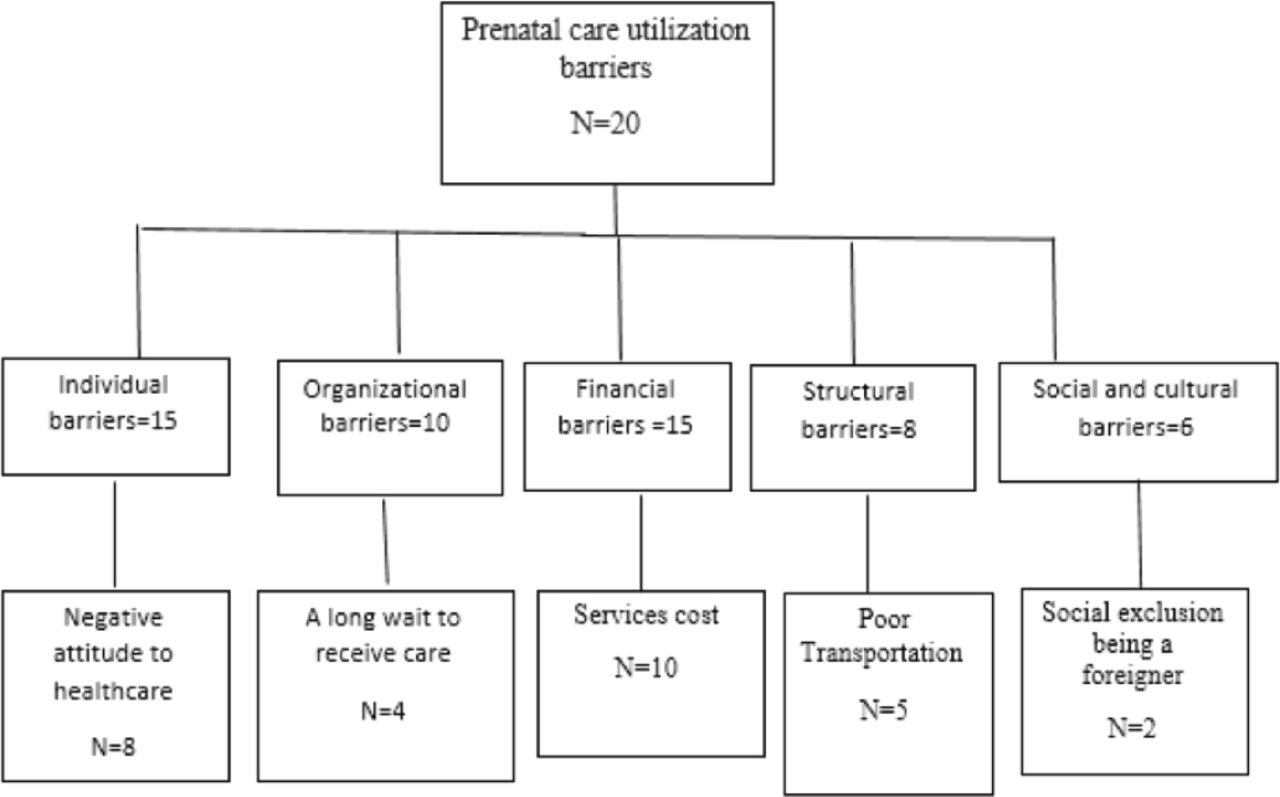
After searching in various databases, 112 related articles were found. After reviewing article titles, 67 unrelated articles and abstracts were excluded, 45 articles were evaluated, 20 of them were duplicated, and the quality of 25 articles were analyzed. Therefore, 5 articles were excluded due to not mentioning the sample size, mismatches between method and data or results. At last, 20 articles were selected for final analysis (Figure 1). Prenatal care utilization barrier is summarized in the following sections (Table 1). Barriers were divided into 5 groups. Individual barriers were related to women and family, organizational barriers were related on health system, financial barriers were economic status of women, structural barriers were related to organizations that affected on health indirectly.23 Social and cultural barriers have focused on languages, different conceptions of gender and sexuality and specific ethnic groups.24 Among the above mentioned barriers, individual barrier,25-31 and financial barriers32-37 are more observed. Other barriers were in the next ranks.38-44

Study selection diagram of 112 related articles regarding barriers related to utilization of prenatal care services among women.
Studies in barriers related to prenatal care utilization.
Discussion
Individual barriers
In our study, women negative attitude to health care was one of the most important prenatal care utilization barrier (Figure 2). The relationship between pregnant women and health care providers is very important and in early pregnancy can affect subsequent prenatal care. When a woman thinks that next prenatal care is carried out by the prior provider, the relationship is formed, it can be important for after care utilization by women.45 Public awareness promotion on the importance of prenatal care and its benefits for the child and mother’s health care may eliminate negative attitude toward health care. Encouraging Factors for pregnant women to prenatal care utilization include awareness promotion about the need to be healthy, disease complications, prenatal care importance.23,46 The use of health systems from media, which emphasizes health value in prenatal care, may make women’s negative attitude to prenatal care positive. The innovative strategies suggested group prenatal care (with additional services) and use of health information technology to reduce inequalities, and to promote the qualities of prenatal care.47

Most of prenatal care utilization barriers.
Financial barriers
Financial barriers are the result of the family’s economic situation. It appears poverty is to be most harmful for inadequate access to health care during pregnancy,23,48 in many federal and states financial barrier eliminating policy to prenatal care for eligible women (family income below poverty line) is free.49 These actions provide help to many pregnant women with problem insurance. Insurance of eligible women increases prenatal care access in other countries.47 Governmental and non-governmental financial support affected to health care access. In other words, the public and private support through insurance in community increases health care access. However, there is little suggestion that eliminating financial barriers alone increases health care access.23,50
Organizational barriers
Most studies showed a long waiting period to receive prenatal care, which is a barrier. The problem of midwifery service providers is the high numbers of clients, which cause lack of concentration and attention, fatigue in midwives and increase waiting time for pregnant women. On the other hand, lack of adequate skills in providing services could increase waiting time. Research results indicate that the change in health center working hours and the decrease of the gap between acceptance and examination of patients at the health center can reduce the waiting time.51 Some studies suggested the increase in human and physical resources..52 An appropriate time schedule can reduce patient waiting time without the need additional resources.53,54 By creating small changes to existing processes such as the reduction of time of diagnostic and treatment services at some stations, waiting time for clients will be significantly reduced without additional cost and human resources. Not admitting a large number of clients at the same time, on time presence of staffs, the increase in the number of staff and facilities, appropriate schedule and planning table, the improvement of staffs’ skills, experience and training, suitable information, may reduce waiting time in health services.
Structural barriers
Many women said transportation is a barrier to care. Therefore, ensuring the clinic is near public transportation centers or clinic setting time can reduce transportation problems.55 The community health center model is another proposed solution for access to prenatal care. This model allows women to have access to local health centers that adjust its services to specific communities. Women would be able to seek treatment in their own neighborhoods and have access to staff members that understand their needs such as language barriers and location issues. By using local and community-based health centers, child care problems will be resolved.23
Social and cultural barriers
In this study, social and cultural barriers had less effect on prenatal care utilization. Effective strategies to eliminate the psychological, social, and attitudinal barriers are solved by local community-based services, focus on communications, respect for indigenous peoples and their culture. Respect to family involvement in health issues is important.
More studies were descriptive or qualitative. The number of case-control studies was very limited and consolidated exploratory study was not seen in studies. Access limitation to journals and articles was another research limitation. The strength of this study is its subject. Prenatal care utilization barriers identification and minimizing could have an effective role in reducing mother’s morbidity and mortality. The results of this study can provide basic information and accurate identification about barriers related to prenatal care utilization services for researchers. This result can be useful to design the effective strategies to increase prenatal care coverage and reduce maternal mortality in the future.
In conclusion, this study provides a systematic review of barriers related to use of prenatal care services for the first time. These barriers can be divided into various domains such as individual barriers, financial barriers, organizational barriers, structural barriers and social and cultural barriers. Most studies have been referred to women negative attitude to health care, services cost, financial problems, having a long waiting time to care and poor transportation as prenatal care barriers. To increase prenatal care coverage, it is necessary to pay attention to all domains, especially individual and economic barriers. Further studies should evaluate the effects of education and encouragement of women to reduce barriers and increase prenatal care coverage.
Acknowledgment
The authors would like to thank the Research Deputy of Shahid Beheshti University of Medical Sciences, Tehran, Iran for allowing us to access the electronic journals and databases.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 17, 2016.
- Accepted May 31, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.