


Abstract
Objectives: To assess knowledge regarding the management of odontogenic infections by dentists in Jeddah, Kingdom of Saudi Arabia.
Methods: In this cross-sectional study, 150 practitioners responded to a 26-item paper-based questionnaire between August and December 2014. The questionnaire evaluated knowledge and current clinical practices in managing odontogenic infections, as well as the attitude towards antibiotic use and resistance in the community. Basic medical knowledge (BMK) and critical knowledge (CK) scores were calculated from the dentists’ response to these questions and were compared according to educational level (bachelor and postgraduate degree holders).
Results: The mean BMK score was 1.98 ± 0.4 and CK score was 1.89 ± 0.3. Dentists with bachelor’s degrees had higher BMK scores than those with a postgraduate degree (p=0.005), but CK was not significantly different (p=0.400). Most dentists (77%) would prescribe antibiotics after a routine dental extraction, and would undertake definitive surgical treatment (49.2%) only after a localized space infection developed. Although 82.2% agreed that routine prescription of antibiotics increases bacterial resistance in the community, 71% believe that prescribing an antibiotic after routine oral surgical procedures prevents odontogenic infections.
Conclusion: Dentists in Jeddah require further education through lectures and workshops to stay up to date on current concepts in odontogenic infection management.
Orofacial infections can be classified as odontogenic or non-odotongenic. The most common source of odontogenic inections is the dental pulp or periapical region caused by severe dental decay. When odontogenic infections are not treated promptly and appropriately, the infection can spread into the fascial spaces, for example, the submandibular, sublingual, submental, buccal, and canine spaces.1-3 This may lead to airway involvement or obstruction, requiring prolonged intubation. In severe cases of fascial space infection, such as Ludwig’s angina, a surgical airway is required. Moreover, an untreated infection could spread to the orbit, neck, or mediastinum, and hence may become life threatening.4,5 Involvement of these critical structures and/or the airway makes odontogenic infections one of the most difficult dental problems to manage. Appropriate treatment starts with thorough examination and proper radiographic examination. The host defense response must be evaluated in order to determine the need for referral to an oral and maxillofacial surgeon. Treatment must include airway support, extraction of the causative tooth or removal of the offending source, incision and drainage, medical support of the patient with fluids, and systemic antibiotic therapy.6 Many misconceptions exist among the dental community with regards to the timing of incision and drainage and antibiotic therapy. It is prudent that general medical and dental practitioners become aware of the new era in microbiology, surgical treatment, and antibiotic therapy for odontogenic infections. This is of utmost importance because the complications of severe odontogenic infections are preventable. This can only be achieved if the general dental and medical community provide the latest information with the current state of knowledge and understand newly discovered concepts in the field of odontogenic infection. A comprehensive literature search using the Medline and PubMed databases (from 1990 to 2014) revealed that there are no studies in the Kingdom of Saudi Arabia (KSA) that evaluate the knowledge of general dentists, specialists, or oral and maxillofacial surgeons regarding odontogenic infections. In addition, the common practice of over-prescribing antibiotics by dentists may have increased antibiotic resistance in this community. Furthermore, there is no consensus on how these infections should be managed by dental health professionals. The aim of this study was to establish a baseline of the knowledge and practice of managing odontogenic infections and the principles of antibiotic therapy use by general dentists and specialists in different sectors in Jeddah, KSA.
Methods
This cross-sectional study was approved by the Research Ethics Committee of the Faculty of Dentistry, King AbdulAziz University, Jeddah, KSA. The study was conducted in accordance with the World Medical Association Declaration of Helsinki.
Subjects
Subjects targeted in this study were general and specialist dentists working in Jeddah from private clinics and governmental hospitals. Subjects from the governmental hospitals included a population of dentists who work in the primary care, secondary care, and tertiary care centers of the Ministry of Health and university hospitals. Inclusion criteria were dentists from the government or private sectors who have at least a Bachelor of Dental Surgery degree or its equivalent. Dental students and dental assistants were excluded. Three hundred questionnaires were hand-delivered to the general dentists and specialists in the private and the governmental sector in Jeddah. The survey included a cover letter explaining the aim of the study and requesting voluntary participation of the dentist. After allowing sufficient time for the participants to thoroughly read the questionnaire and completed it, the questionnaires were collected directly from the respondents.
Survey
The validated questionnaire was a 26-item pre-tested that was developed with the assistance of a dental public health professional. Dentists participated in the study on a voluntary basis were assured of their anonymity and the confidentiality of their responses. The survey sought information on the following items: 1) The clinician’s demographic data: age, years of experience, specialty and type of practice (government or private), and degree (bachelor’s degree and postgraduate degree). The latter included clinical residency training, master’s, and doctoral degrees; 2) The clinician’s frequency of attendance of continuing education lectures, workshops, and conferences; 3) The scope of oral surgery practice procedures implemented in their practice; 4) Knowledge: This section of the survey was split into 2 components, basic medical knowledge (BMK) and critical knowledge (CK), based on how relevant the knowledge is to the management of odontogenic infections. The questions that were considered critical were those that had direct implications for clinical management of odotongenic infections. A list of the questions included in the BMK and CK sections is shown in Table 1; 5) The clinician’s current practice with regards to treating patients with odontogenic infections; 6) The clinician’s attitude towards antibiotic treatment and its effect on antibiotic resistance in the community.
Questions included in the questionnaire to assess the knowledge of the surveyed dentists.
Data analysis
Data from the questionnaires were entered into a computer database and analyzed using the Statistical Package for Social Science, version 22 (IBM Corp., Armonk, NY, USA). Descriptive analyses were performed on the demographic data and general responses of the participants. Knowledge questions (BMK and CK) were isolated from the questionnaire and scored as follows: 0 = poor knowledge, 1 = below average, 2 = average, and 3 = high. A Student’s t-test was used to compare the knowledge score for the bachelor degree holders with the postgraduate degree holders in both the BMK and CK categories. A one-way ANOVA was used to compare the BMK and CK according to years of experience (>1-5 years, 5-10 years, and >10 years). The statistical significance value was set at a p<0.05.
Results
A total of 150 out of 300 surveys were retrieved, indicating a response rate of 50%.
Demographics
The demographic data for the dentists participating in the survey are summarized in Table 2. This table also shows the responses of the surveyed dentists to questions concerning regular attendance at continuing education lectures and workshops, and the scope of the practice in terms of oral surgical procedures. When asked regarding the availability of an oral and maxillofacial surgeon for referral, only 32.4% of the dentists responded “readily available for referral,” while 55.9% responded “sometimes,” and 11.6% stated lack of access to an oral and maxillofacial surgeon in their practice.
Demographic data, work sector, scope of practice, and frequency of attending continuing education of the surveyed dentists.
Knowledge of the basic principles of odontogenic infections
The mean score for BMK of the surveyed dentists was 1.98 ± 0.4 (65.9%), whereas the mean CK score was 1.89 ± 0.3 (63%). Dentists with bachelor degrees scored higher in BMK than those who held a postgraduate degree (p=0.005). However, there was no statistically significant difference in CK between respondents with only bachelor’s degrees and those with postgraduate degrees (p=0.400) (Table 3). When using the years of experience (>1-5 years, 5-10 years and >10 years), no difference was found between the mean BMK and mean CK (p>0.05 for both).
Basic medical and critical knowledge of the dentists according to educational level.
Clinical practice
Seventy-seven percent of respondents stated that they would prescribe an antibiotic after a routine surgical extraction, whereas only 12.5% stated they would do so if the patient were immunocompromised. Most respondents (64.6%) would prescribe amoxicillin and clavulanic acid, whereas only 25% would prescribe amoxicillin alone. With regard to the treatment of an indurated submandibular space infection in a child with fever and dehydration, the majority (52.3%) would prescribe an antibiotic and wait until the abscess became more localized before performing an extraction or incision and drainage. Similarly, most respondents would wait until infection in a canine space became more localized before performing an incision and drainage, or extraction (49.2%). With regard to the treatment of pericoronitis in a healthy patient without trismus, only 17% of the dentists would perform an extraction, while 33.1% would perform an operculectomy. Table 4 shows the detailed results of the dentists’ responses to the practice questions.
Responses of the surveyed dentists to questions regarding their practice, management of, and attitude towards odontogenic infections.
Attitude
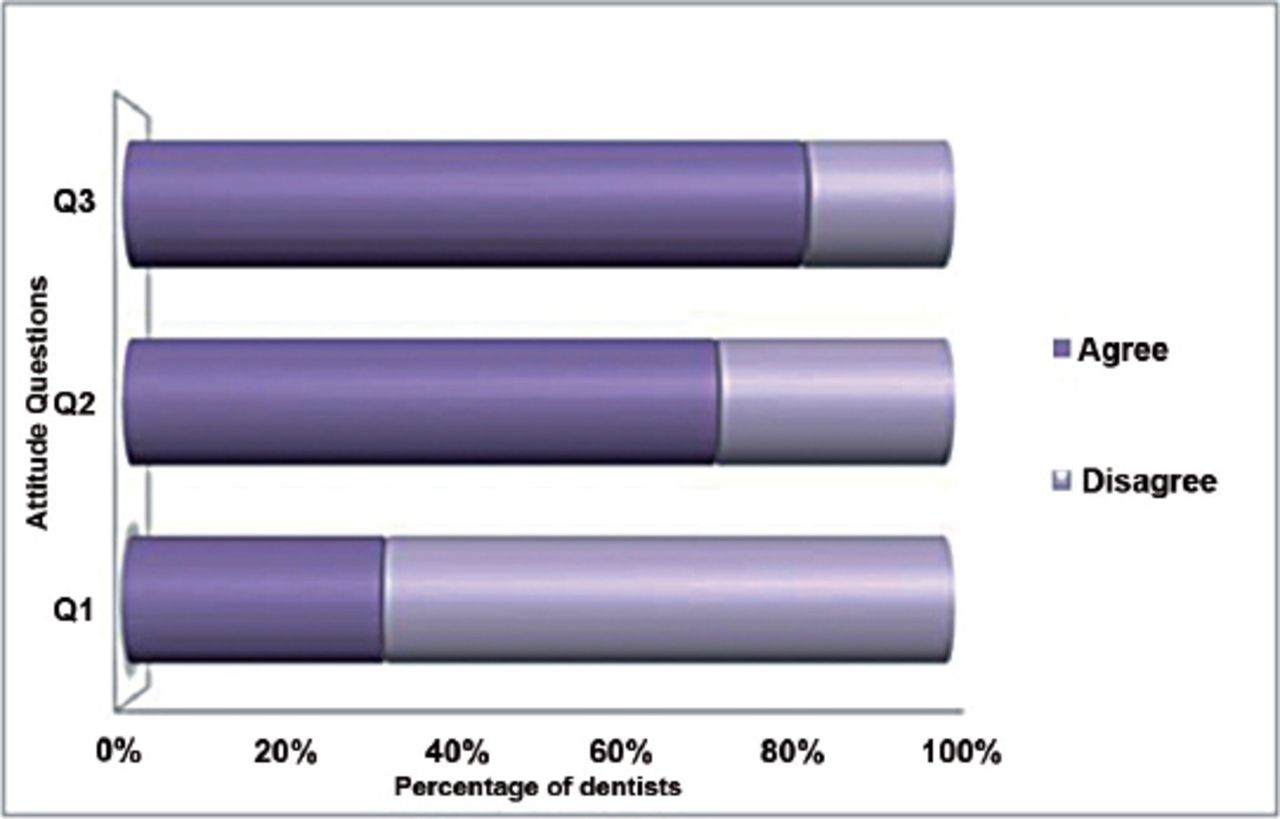
In responding to the first question, only 31% of the respondents agreed to the need for incision and drainage after failure of antibiotic therapy. Approximately 71% would prescribe antibiotics for oral surgical procedures in the absence of an odontogenic infection in order to prevent such an infection, whereas 82.2% agreed that routine prescription of antibiotics when not needed increases the resistance of bacteria in the community (Figure 1).

Attitudes of surveyed dentists towards odontogenic infection management and prescribing antibiotics.
Discussion
Our results indicate that the general medical knowledge of dentists who responded to our questionnaire is average. In light of our discovery of misconceptions regarding delaying treatment of odontogenic infections until fluctuation occurs, practitioners would need to attend updated continuing education courses in order to have the basis for treating odontogenic infections in timely manner. Delaying the treatment of odontogenic infection can reasonably be considered malpractice.
Newly graduated practitioners achieved a higher basic medical knowledge score than those with postgraduate degrees. Dental students are exposed to the fundamentals of microbiology and antimicrobial therapy in many undergraduate subjects. Therefore, bachelor degree holders are closer to their recent examination and under close supervision by academic oral and maxillofacial surgeons in dental teaching institutions. The higher the postgraduate education of the practitioner, the more likely the need for continuing education courses in the management of odontogenic infections.
More confidence and better judgment is usually attained with clinical experience; however, for the surveyed dentists, additional years of experience did not translate into superior knowledge in either the basic medical or clinical categories. This could be due to lack of interest, lack of exposure to these types of cases, or the dentists not staying updated with the latest in management of odontogenic infections and antimicrobial therapy through courses, journals, or discussion groups.
Soft tissue excision or operculectomy was the treatment of choice for pericoronitis in 33.1% of respondents, even when trismus was absent. In one study,7 pericoronitis constituted 5.8% of all dental emergencies. It is now accepted that the definitive treatment of choice should be extraction of the offending tooth; this indicates that one-third of respondents are delaying the appropriate treatment. This might be attributed to the lack of access to an oral and maxillofacial surgeon in most respondents’ practices: only 32.4% of the dentists have an oral and maxillofacial surgeon readily available for referral, and 11.6% do not have any access.
There was a general tendency to delay the treatment of odontogenic infections. In this survey, nearly half of the of respondents (49.2%) would wait for abscesses to localize before attempting to remove the source of infection, and would rather prescribe antibiotics, regardless of clear signs of severe infection. This was particularly evident in responses to the question regarding a pediatric case that presented with submandibular space infection with fever and dehydration. This is another warning signal, as severe infections in children can deteriorate rapidly and quick to spread if not treated promptly by removing the source of infection. Delayed treatment and self-medication, along with a presentation with fever, was associated with a prolonged hospital stay in a study performed in Greece.8 Early treatment was found to result in healing without a significant scar formation.9 This emphasizes the need for the governing body for health care in KSA to implement new guidelines requiring experienced older practitioners to be updated regarding new understanding in the field of odontogenic infections.
Analyzing attitude responses revealed interesting findings. Although most respondents believed that prescribing antibiotics unnecessarily increases microbial resistance in the community, a significant number of respondents still prescribe antibiotics in situations when it is not necessarily indicated. An example was tooth extraction that needed sectioning or bone removal in the absence of infection; 77% of respondents stated that they would prescribe antibiotics in this situation, with the majority prescribing amoxicillin/clavulanate. This could be attributed to the respondents’ efforts to prevent infection. However, removal of the potential source of infection is always sufficient as shown by previous studies.6,9 An exception might be a case where the immune system is compromised. This is not necessarily a problem localized in KSA, but is rather a more global issue that has been reported in the United States, Nigeria, Czech Republic, and Japan.10-13 Practitioners should be highly selective when prescribing amoxicillin/clavulanate, because there has already been some evidence of resistant strains of Escherichia coli and Salmonella spp. reported in several studies.11,13 In a study by Poeschl et al,14 the resistance rate in severe deep space head and neck infections was found to be 14% against clindamycin, 14% against macrolides, and 7% against Penicillin G.
Self-medication is probably one of the major causes of developing antibiotic resistance in KSA.15,16 Amoxicillin with or without clavulanate is the most frequently self-prescribed antibiotic in Al-Ahsa region of KSA. In this study, a significant number of users took the antibiotic for only 2 days for acne or common cold, which would increase the potential for developing resistance.17 It can be safely assumed that other regions would have the same issue. Penicillin resistance is reported to be at approximately 70% of pneumococcal strains;18 these microorganisms have been cultured and isolated from odontogenic infections.19
One limitation of this study is the variation in the participant’s backgrounds. Practitioners who graduated from different education systems may have variable approaches to the management of odontogenic infections. Different teaching methods can be applied to prepare practitioners to face the challenge of managing odontogenic infections. Effective methods include invented dialogue and misconception checks. This cross-sectional study may be followed by a longitudinal study to assess the impact of these different teaching methods.
In conclusion, knowledge of the normal indications for medical and surgical treatment of fascial space infections will ensure that these cases are dealt with effectively. The knowledge of dentists in Jeddah on the principles of odontogenic infections and the basics of antibiotic therapy is generally average. This study provides evidence of lack of agreement among these practitioners on the indications for, timing, and type of antibiotic that should be used in the absence and presence of signs of infection. There is also definitive evidence of overuse of antibiotics in dental cases where antibiotics are not indicated. There is a tremendous need in the dental community for focused lectures and continuing education courses on this topic to ensure early intervention and to prevent serious life-threatening complications.
Acknowledgment
The authors gratefully acknowledge the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia for technical and financial support. The authors would like to thank Mr. Kalvin M. Balucanag for his assistance in statistical analysis.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. This project was funded by the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia (Grant no. 009/9/1430).
- Received January 31, 2016.
- Accepted February 24, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.