


Abstract
Objectives: To perform a literature review and meta-analysis evaluating the effectiveness of medial and lateral meniscus allograft transplantation (MAT).
Methods: The literature review and meta-analysis were conducted between August and October 2015 in the People’s Hospital of China Three Gorges University, Yi Chang, China. A systematic search was performed in the Medline and EMBASE databases, and the Cochrane Library for relevant literature published through October 2015. The outcomes of the included studies were analyzed in terms of the Lysholm Score, International Knee Documentation Committee (IKDC) Score, Knee Injury And Osteoarthritis Outcome Score (KOOS), Visual Analog Scale (VAS), Tegner Activity Score, MRI results, and failure rates. An adapted version of the Newcastle-Ottawa Scale was used for the methodological quality assessment in the meta-analyses.
Results: The literature review identified 12 observational studies, including 7 retrospective studies, 4 prospective studies, and the nature of one study was not reported. Significant differences in the outcomes of the lateral MAT group and the medial MAT group were observed in the IKDC scores, KOOS pain values, KOOS activities of daily living (ADL) values, and the absolute and relative extrusions observed on MRI, which suggested that the lateral MAT patients experienced superior clinical benefits compared with the medial MAT patients. However, significant differences between the lateral MAT group and the medial MAT group were not observed with regards to the Lysholm Scores, KOOS symptom values, KOOS sports and recreations values, KOOS quality of life (QOL) values, Tegner Activity Scores, VAS for pain values, and failure rates.
Conclusion: The analysis results indicated that lateral MAT provides superior clinical outcomes compared with medial MAT according to the KOOS and IKDC scores. In addition, greater graft extrusion was observed in the medial group on MRI. Although significant differences were not detected between the 2 groups, the medial MAT patients were more prone to failure compared with the lateral MAT patients.
The meniscus plays an important role in the biological and biomechanical environment of the knee, and the load bearing, load transmission, shock absorption, joint stability, joint lubrication, joint congruity, and proprioception functions of the meniscus are well understood. Accordingly, meniscal tissue should be preserved as much as possible, especially in younger patients. However, in irreparable cases, meniscal preservation is impossible. Meniscectomy will increase the load of articular cartilage and cause degenerative changes of the knee joint, and the amount of resected tissue is proportional to the amount of degeneration.1 Furthermore, the loss of a meniscus will cause progressive pain and function losses, which lower the patient’s quality of life. After meniscus removal, meniscus allograft transplantation (MAT) has been shown to represent an effective treatment method for reducing pain and improving function in the short-, medium- and long-term follow-up periods.2-10
The meniscus is a semi-lunar biconcave fibrocartilaginous disk within the medial and lateral tibiofemoral articulations, and the anatomical structures of both meniscuses are different. The shape of the lateral meniscus is approximately an “O”, whereas the shape of the medial meniscus is a “C,” and it is larger and thinner than the lateral meniscus. The medial meniscus is securely attached along the periphery of the capsule, and the tendon of popliteus separates the lateral meniscus and the articular capsule. Because of the different anatomical structures of the meniscuses, the lateral meniscus shows a greater degree of activity compared with the medial meniscus, and the medial meniscus is more easily damaged compared with the lateral meniscus. Moreover, the medial meniscus cover 64% and the lateral meniscus 84% of the medial tibial plateau, which transmits approximately 50% and 70% of the load acting on the respective sides of the joint.11 The medial meniscus is a vital stabilizer of the knee, whereas the lateral meniscus is more important for load transmission in the knee.12 In addition, the medial tibial plateau is concave, which relatively widens the contact area between the tibial plateau and femoral condyle; however, the lateral tibia platform is convex, and the absence of a lateral meniscus results in lateral femoral condyle loads that are concentrated within a small area.13 Lesions of the lateral meniscus are more likely to induce articular cartilage degeneration and clinical symptoms. Most studies have confirmed that degenerative changes in the articular cartilage after lateral meniscectomy are more rapid and severe than those after medial meniscectomy.14-16 Moreover, studies have suggested that lateral meniscectomy patients present worse outcomes compared with medial meniscectomy patients.17-19 For patients with debilitating pain and function losses secondary to meniscectomy, medial and lateral meniscal allograft transplantation represents an acceptable surgical option. However, few randomized controlled trials have focused on evaluating the efficacy of medial and lateral MAT, and the available studies are limited by their small sample size and variable definitions and results, thereby resulting in controversy over the clinical benefits of medial and lateral meniscal transplantation. The objective of this literature review and meta-analysis was to compare the clinical outcomes of both types of MAT and determine whether medial or the lateral meniscus transplantation produces better clinical results.
Methods
Search strategy
We performed systematic searches of the relevant literature contained in Medline (PubMed), EMBASE and the Cochrane Central Register of Controlled Trials for studies published up to October 2015. The search strategy consisted of a combination of keywords related to meniscal allograft transplantation terms (“meniscal allograft transplantation” OR “meniscal allograft replacement” OR “meniscal transplantation” OR “meniscal replacement”) and anatomical terms (“medial meniscus” OR “lateral meniscus” OR “medial” OR “lateral”). The research was limited to English publications, although it was not limited to randomized controlled trials and included all study designs. In addition, the references of identified studies were manually reviewed to identify additional potentially eligible trials. This process was performed iteratively until no additional articles were identified.
Inclusion and exclusion criteria
The following inclusion criteria for the selected articles were applied: 1) The studies involved patients who had MAT; 2) at least one of the following methods of data evaluation for MAT was applied: Lysholm Score,20 International Knee Documentation Committee (IKDC) value,21 Knee Injury and Osteoarthritis Outcome Score (KOOS),22 Visual Analog Scale (VAS), Tegner Score,23 MRI, and failure rate; 3) medial and lateral meniscus comparisons of the postoperative clinical outcomes were performed; and 4) follow-up investigations occurred for at least 12 months. The main exclusion criteria included 1) animal and cadaver studies, 2) insufficient data, 3) and case reports and studies without long-term follow-up investigations.
Data collection and quality assessment
Two investigators (Wei G and Ru N) independently reviewed the full publications and extracted data from the studies using an established data extraction form. Relevant data included basic information on the included studies, demographic information, intervention characteristics, and all of the outcome parameters, which consisted of Lysholm Scores, IKDC values, KOOS values, Tegner Scores, VAS values, extrusion observed on MRI and failure rates. The extracted data were entered into a standardized Excel (Microsoft Corp) file and checked by another investigator (YPL). Inconsistencies were resolved by discussion and consensus. For the retrospective studies and prospective studies, an adapted version of the Newcastle–Ottawa Scale (NOS) was used for the methodological quality assessment. The maximum NOS score was 9. We defined a Newcastle-Ottawa Scale score of less than 4 points as low methodological quality, a score of 5 or 6 as medium quality, and a score of 7 or higher as high methodological quality.
Statistical analysis
The meta-analysis was performed using Review Manager (Version 5.2, The Cochrane Collaboration, Oxford, UK). For continuous outcomes, the mean and standard deviation (SD) were used to calculate the mean difference (MD) or standardized mean difference (SMD) and the 95% confidence interval. For dichotomous outcomes, such as in the number of events, the relative ratio (RR) and the 95% CI were calculated. When the SD was not provided, it was derived from comparable studies or original scores (namely, confidence intervals). Heterogeneity was assessed by using the χ2 test and the I2 statistic. When the p-value from the χ2 test was <0.1 or when the I2 statistic was >50%, the data were considered to be heterogeneous and a random-effects model was selected. Otherwise, a fixed-effects model was applied to estimate the overall summary effect sizes. To assess the stability of the synthesis results, a sensitivity analysis was performed by removing every single study per iteration to evaluate the influence of individual studies on the pooled result. A funnel plot was used to explore the potential publication bias. At values of p<0.05, the differences were statistically significant.
Results
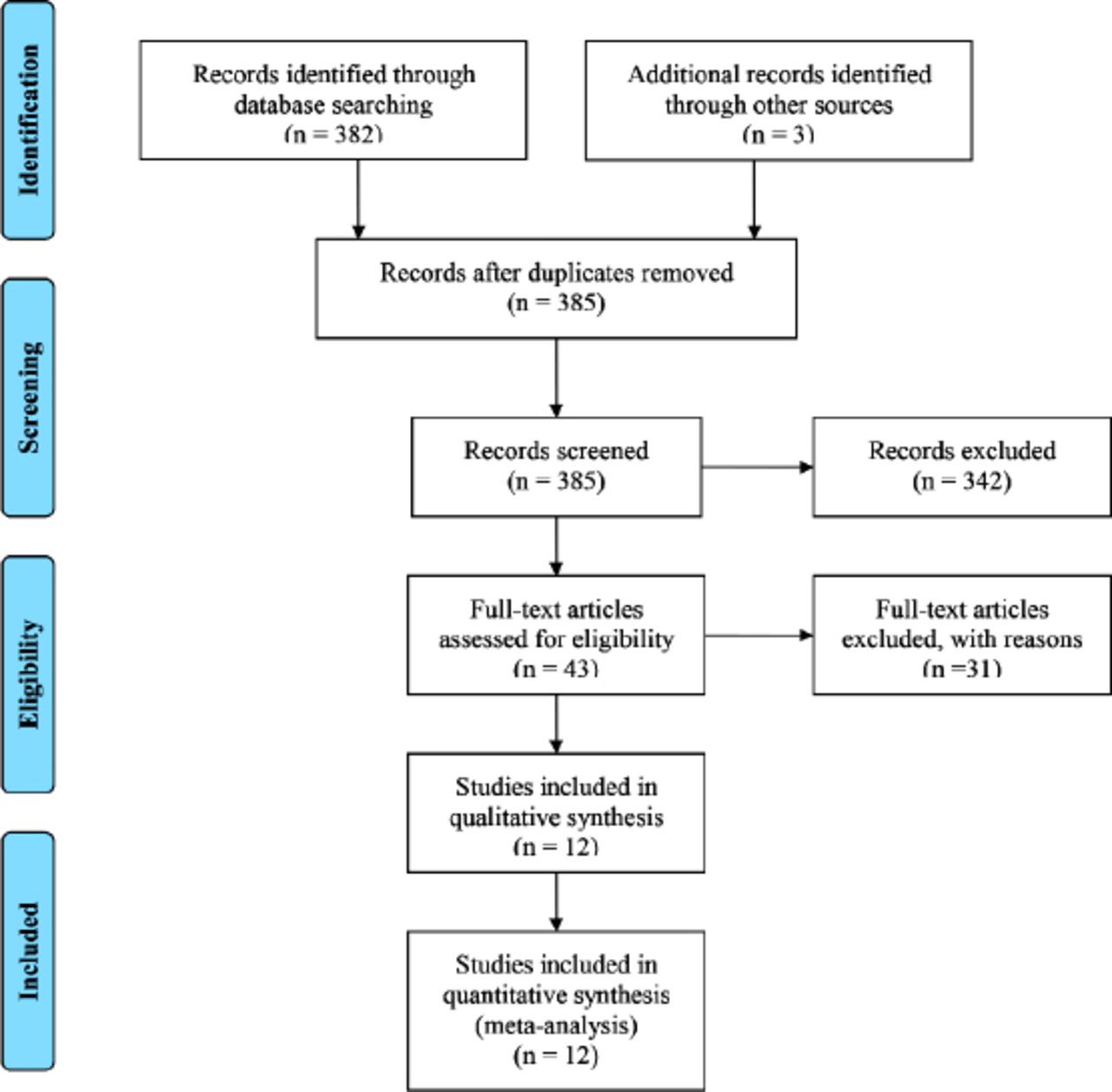
The primary literature search identified 385 potentially relevant titles. After discarding the duplicates and reviewing the titles and abstracts, 342 publications were excluded. The remaining literature was further assessed for eligibility based on the full-text articles. Twelve publications that were classified as observational studies were ultimately included for the data collection and critical assessment. Of the 12 studies, 7 were retrospective,6,7,13,24-27 4 were prospective,9,28-30 and one was not reported.8 Articles were primarily excluded due to lack of comparisons between the medial group and the lateral group, or a lack of available clinical results for extraction. The process of literature selection is presented in Figure 1.

Flow diagram of the literature search included in the study.
Study characteristics and quality
A total of 676 participants were included in the assessed studies, and 280 were sorted into the medial group and 396 were sorted into the lateral group. The mean age range of the subjects was between 31 and 40 years old. The mean follow-up time ranged from 24.9 to 165.6 months. The majority of meniscal allograft transplantation patients were male (66% male). The basic conditions of the included studies are shown in Table 1. The NOS for assessing the quality of each study is shown in Table 2. We classified 2 studies29,30 in the high methodological quality group, whereas the remaining ten studies6-9,13,24-28 were in the medium methodological quality group.
Characteristics of the studies.
Quality assessment of the 12 evaluated studies using the Newcastle-Ottawa Scale (NOS).
Effects of intervention. Lysholm score
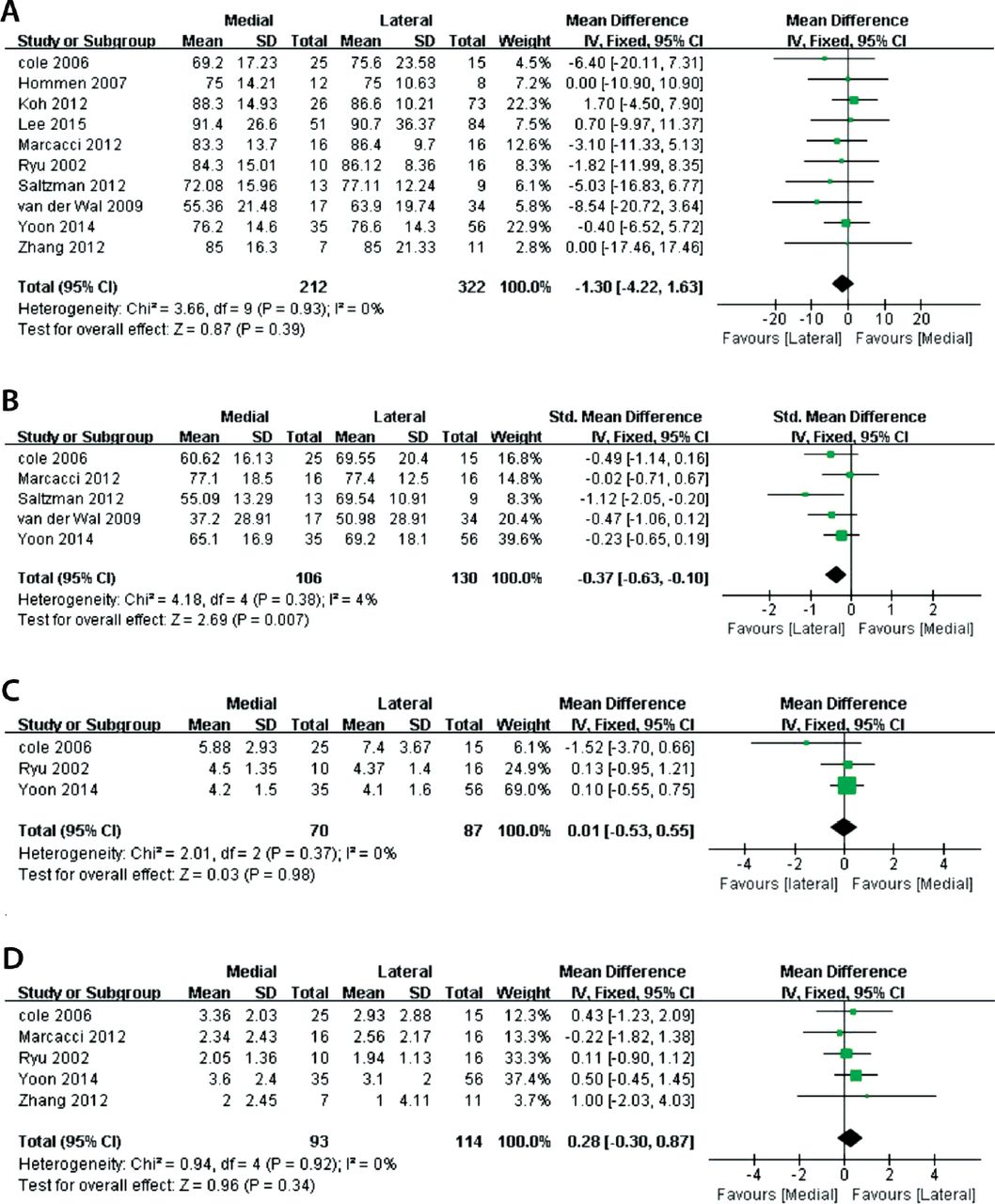
Ten studies provided adequate data from postoperative follow-up investigations using the Lysholm score for the medial group and the lateral group.7,8,13,24-30 These 10 studies included 534 patients, of which 212 patients were assigned to the medial group and 322 patients were assigned to the lateral group. Statistical heterogeneity was not observed among the studies (p=0.93 and I2 = 0%), and a fixed-effects model of the pooled data did not reveal significant differences in the Lysholm scores and function outcomes between the medial and lateral groups (MD: -0.13, 95% confidence intervals [CI]: -4.22 to 1.63; p=0.39; Figure 2A).

Meta-analysis of the lysholm score A) IKDC value, B) Tegner activity score, C) and VAS for pain D) between the medial and lateral MAT groups. CI - confidence interval, SD - standard deviation, MAT - meniscus allograft transplantation, IKDC - International knee documentation committee, VAS - visual analog scale.
International Knee Documentation Committee
Five studies provided IKDC clinical outcomes7,8,13,28,29 and included 106 patients in the medial group and 130 patients in the lateral group. However, 2 of these studies24,25 were excluded from the data pooling because the authors dichotomized the IKDC score. Moreover, one study26 was excluded because the IKDC score was dichotomized and the medial and lateral groups did not show contrasting values. For the IKDC analysis, the effect sizes were calculated by the standardized MDs because the MDs between the studies was too large. The meta-analysis indicated a significant difference in the IKDC scores between the medial and lateral groups, and the standardized mean difference of the IKDC scores was -0.37 (95% CI: -0.63 to -0.10, p=0.007, Figure 2B), with the lateral group showing the highest values. The heterogeneity test did not show significant values (p=0.38, I2 =4%).
Tegner activity score
Five studies provided data on the Tegner Activity Score. However, 2 studies25,29 included mean or median values without SDs, and the SDs could not be directly and indirectly derived through other methods. Three studies provided useful data with mean and SD values and included 70 medial and 87 lateral MAT patients.13,26,28 Heterogeneity was not observed between the groups (p=0.37, I2 = 0%), and the MD were approximately equivalent between the medial and lateral groups (MD: 0.01, 95% CI: -0.53 to 0.55; p=0.98; Figure 2C).
Visual analog scale for pain
Five studies provided VAS for pain values13,24,26,28,29 and included a total of 207 patients, with 93 patients in the medial MAT group and 114 patients in the lateral MAT group. The meta-analysis indicated that significant differences did not occur between the medial and lateral MAT groups (MD: 0.28; 95% CI: -0.30 to 0.87; p=0.34; Figure 2D), and significant heterogeneity was not observed (p=0.92, I2 = 0%).
Knee injury and osteoarthritis outcome score
In 7of the studies included in the analysis, 5 studies6-8,24,28 used the KOOS subscale to measure the postoperative MAT outcome and included 78 patients in the medial group and 84 patients in the lateral group. The KOOS subscales (KOOS pain: p=0.88, I2 = 0%, MD: -9.65, 95% CI: -15.91 to -3.38, p=0.003; Figure 3A, and KOOS activities of daily living (ADL): p=0.38, I2 =4%, MD: -8.04; 95% CI: -12.89 to -3.20, p=0.001; Figure 3C) indicated greater improvements in the lateral group than in the medial group. The MDs for the remaining KOOS subscales were not statistically significant for the lateral and medial MAT groups: KOOS Symptoms (p=0.3, I2 = 17%, MD: -4.85, 95% CI: -10.42 to 0.71, p=0.09; Figure 3B), KOOS sports and recreation (S&R) (p=0.16, I2 = 39%, MD: -7.09; 95% CI: -14.5 to 0.33, p=0.06; Figure 3D), KOOS quality of life (QOL) (p=0.57, I2 = 0%, MD: -5.03, 95% CI: -13.16 to 3.1, p=0.23; Figure 3E).

Meta-analysis of the KOOS Pain (A), KOOS Symptoms (B), KOOS ADL (C), KOOS S&R (D), and KOOS QOL (E) between the medial and lateral MAT groups. CI, confidence interval; SD, standard deviation; MAT, meniscus allograft transplantation; KOOS, Knee Injury and Osteoarthritis Outcome Score; ADL, Activities of Daily Living; S&R, Sports and Recreation; and QOL, Quality of Life.
Absolute and relative extrusion observed on MRI
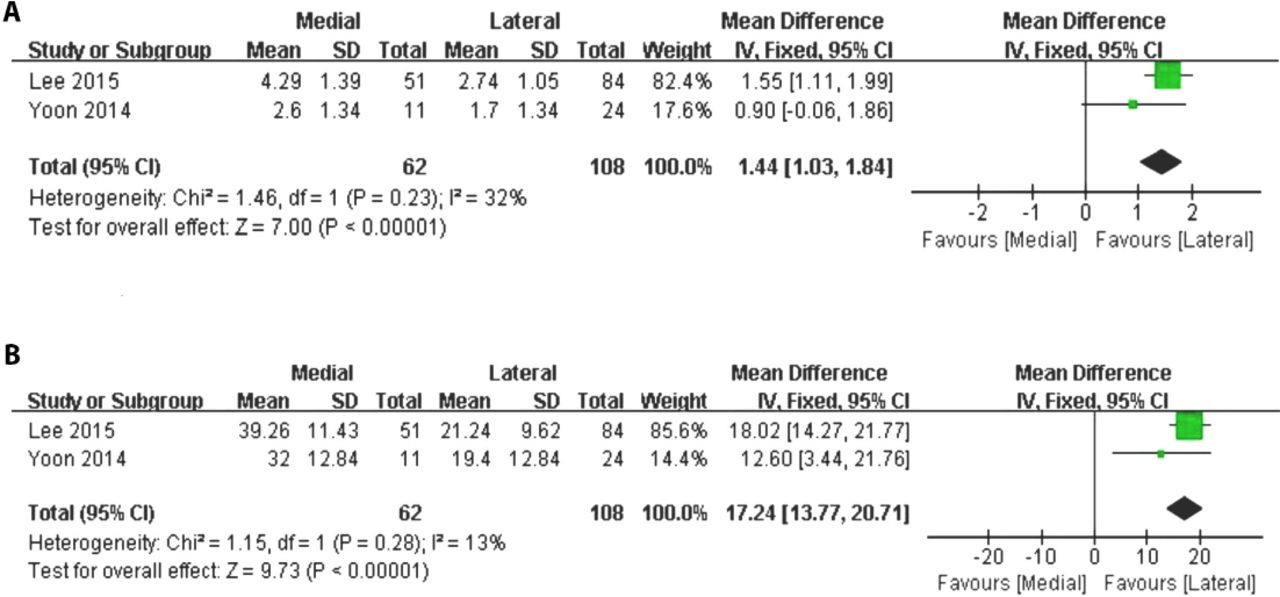
The absolute and relative extrusion observed on MRI was reported in 3 studies; however, due to the different measurement and calculation methods, one study27 was eliminated and 2 studies13,30 were included for data pooling. The 2 studies enrolled 170 patients, with 62 patients in the medial group and 108 patients in the lateral group. The MD in the absolute extrusion observed on MRI was 1.44 (95% CI: 1.03 to 1.84; p<0.00001; Figure 4A) in favor of the lateral group, and statistical heterogeneity was not observed (p=0.23, I2 = 32%; Figure 4A). For the relative extrusion observed on MRI, an evaluation of both groups indicated that the lateral group presented significantly higher values (MD: 17.24; 95% CI: 13.77 to 20.71; p<0.00001, Figure 4B). Statistical heterogeneity was not observed (p=0.28, I2 = 13%; Figure 4B).

Meta-analysis of the absolute extrusion observed on MRI and A) relative extrusion observed on MRI B) between the medial MAT and lateral MAT groups. CI - confidence interval, SD - standard deviation, and MAT - meniscus allograft transplantation.
Failure rates
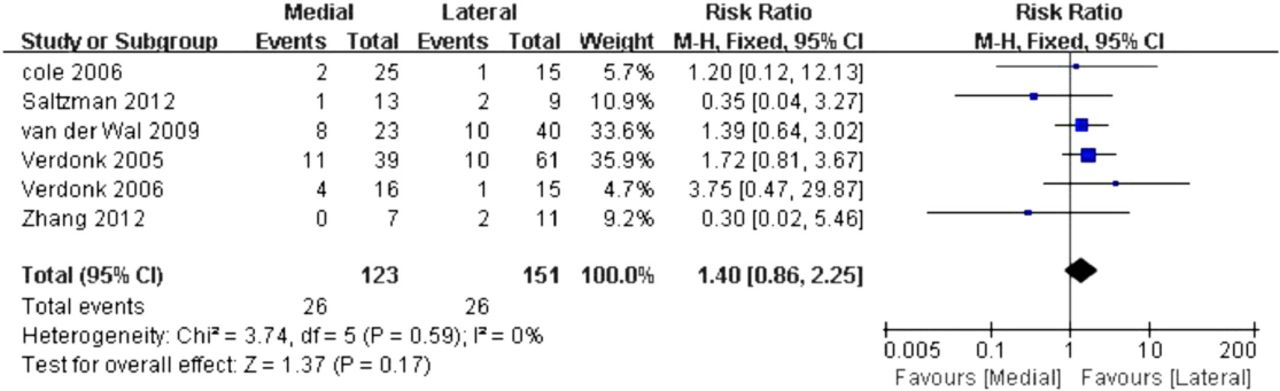
Of the total studies used in this meta-analysis, 5 studies6-9,24,28 reported failure rates, with allograft failure observed in 26 patients out of 123 medial MAT patients and 151 lateral MAT patients. The criteria for failure of an allograft were complete resection of the graft with or without the placement of unicompartmental knee arthroplasty or TKA. However, a poor Lysholm score (<65) and a lack of improvement in the pain score were considered the standards of failure by Hommen et al;25 therefore, this study was excluded. The meta-analyses demonstrated a trend towards lower failure risk in the lateral MAT patients, although the differences between the 2 groups were not statistically significant (RR: 1.4, 95% CI: 0.86 to 2.25, p=0.17, Figure 5). The heterogeneity test also showed statistically insignificant results (p=0.59, I2 = 0%; Figure 5)

Meta-analysis of the failure rates between the medial and lateral MAT groups. CI - confidence interval, SD - standard deviation, and MAT - meniscus allograft transplantation.
Publication bias and sensitivity analysis
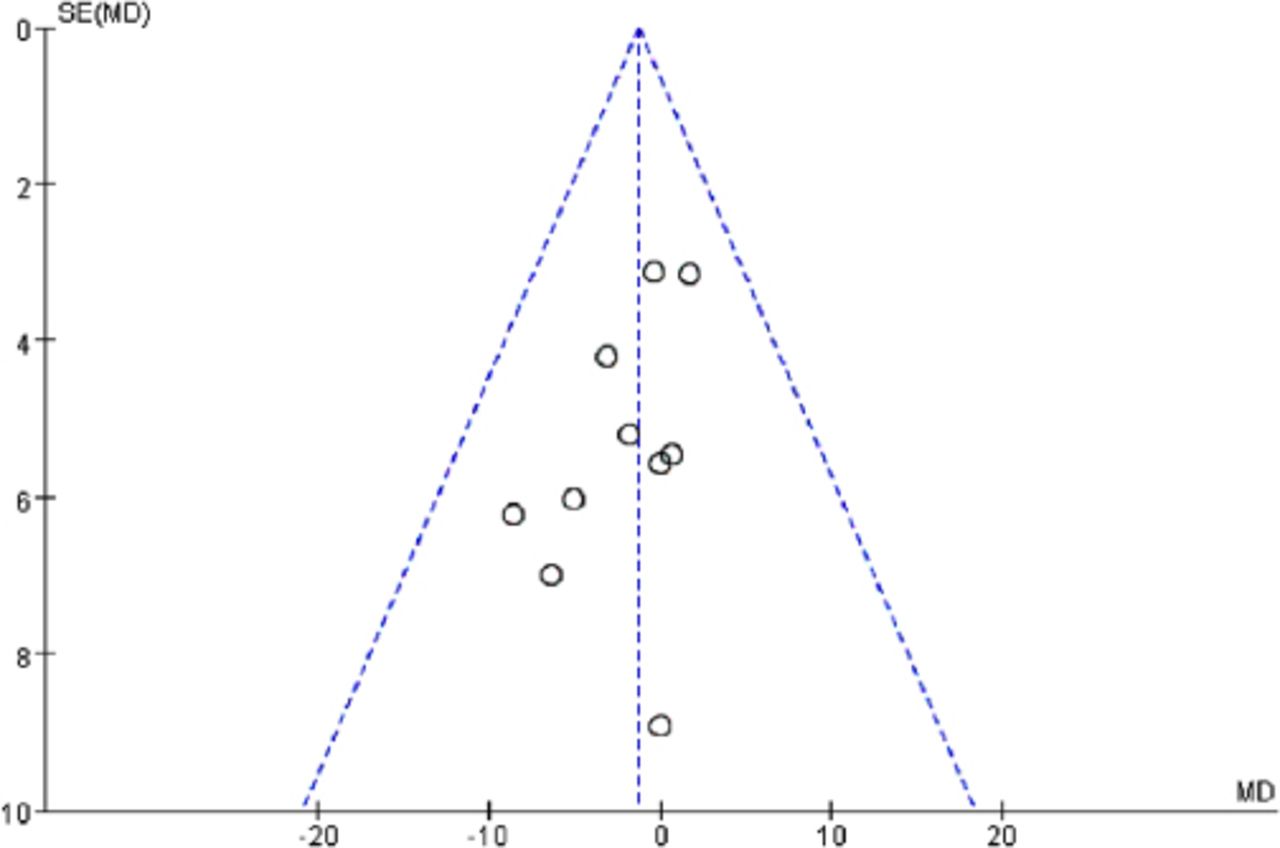
The funnel plots of the Lysholm Score showed a fairly symmetrical distribution of the pooled estimates from the meta-analysis. Ten studies were scattered and spread evenly on both sides of the average (Figure 6). To evaluate the robustness of our analysis, a series of sensitivity analyses were conducted by eliminating individual studies one at a time. According to the analysis results, none of the studies had a greater impact relative to the other selected studies except for Zhang’s study,24 which had an impact on the KOOS Symptom and S&R values. After eliminating Zhang’s study, the pooled KOOS symptom and S&R results changed significantly (p=0.51, I2 = 0%, MD: -6.44, 95% CI: -12.34 to -0.54, p=0.03; and p=0.51, I2 = 0%, MD: -11.11, 95% CI: -19.46 to -2.77, p=0.009).

Funnel plot of the lysholm score. MD - mean difference, SE - standard error
Discussion
In the pooled study of approximately 676 participants from 12 studies, we chose the Lysholm score, IKDC, Tegner activity score, VAS, KOOS, MRI and failure rate to evaluate improvements in knee function and pain relief in the postoperative patients. The primary findings from our study consistently showed that the clinical lateral MAT and medial MAT results were significantly different with regard to the IKDC, KOOS, and MRI values but relatively equivalent for the Lysholm Scores, Tegner Activity Scores, VAS values, and failure rates. The main purpose of performing MAT procedures is to re-create the load distributing properties of the native meniscus to prevent or slow the cartilage degeneration process, alleviate pain and improve quality of life. Validated outcome scores related to knee injuries and general health were used to assess the curative effect of the medial and lateral MAT procedures. This meta-analysis demonstrated that significant differences in the Lysholm Score did not occur between the 2 groups, which indicated that the medial MAT procedure could produce similar results with regard to improved functions compared with the lateral MAT procedure. In addition, the Tegner Activity Score was also compared between the medial MAT group and the lateral MAT group, and significant differences were not observed. The Lysholm Score and the Tegner activity score results were consistent with the result of studies conducted by Farr et al31 and Vundelinckx et al.12 However, in this meta-analysis, the lateral group acquired higher IKDC scores than the medial group, which suggests that patients undergoing lateral MAT would present improved activity levels relative to patients undergoing medial MAT. In addition, the KOOS subscale can provide an overall evaluation of postoperative MAT outcomes. This meta-analysis demonstrated that significant differences did not occur in the KOOS Symptom, KOOS S&R and KOOS QOL values between the medial and lateral MAT groups, which indicates that lateral MAT patients could achieve similar improvements in function as medial MAT patients. However, the clinical KOOS Pain and KOOS ADL results for the lateral group were better than those for the medial group, and the difference was significant, whereas, the pooled data on the VAS for pain values showed equivalent pain scores between the medial and lateral groups. The results showed that patients with lateral MAT tended to present greater improvements, although statistically significant differences were not detected for the majority of pooled Lysholm scores, VAS values and Tegner activity scores. Nevertheless, in the evaluated studies, the number of medial MAT and lateral MAT patients was insufficient to detect differences between the 2 groups. Thus, differences observed in the outcomes may have been caused by anatomy, biomechanical functions, meniscal lesion frequency, ACL ruptures and postmeniscectomy osteoarthritis incidence. In addition, the 5 score systems included here are subjective and considerable variability was observed among different patients; thus, the results of this study should be considered with caution.
Moreover, failure rates and MRI were used to evaluate the objective results of the medial and lateral MAT patients. In this study, the meta-analysis results for the failure rates showed that the medial MAT procedure was more prone to failure relative to the lateral MAT procedure, although the differences between the 2 groups were not significant. This finding might be explained by the limited number of patients and follow-up investigations included in the present literature review and meta-analysis and the high number of patients with associated ACL laxity.32 Research has suggested that medial MAT patients have a higher risk of failure than lateral MAT patients.9,32,33 The absolute and relative extrusions observed on MRI were also analyzed in our study, although only 2 of the included studies were used in this meta-analysis to assess the extent of graft extrusion in the medial and lateral groups. The pooled data indicated that transplanted medial menisci extruded more significantly than transplanted lateral menisci in terms of the absolute and relative extrusions on MRI, and this finding was consistent with the results of a study conducted by Wilmes et al.34
Study limitations
Our findings from this systematic review and meta-analysis must be interpreted cautiously because of the methodological limitations of this study. In addition to the lack of high-quality evidence, a number of potential limitations should be considered. First, the treatment methods could not be prospectively randomized; thus, a random clinical trial could not be performed. Various retrospective observational studies analyzed here were prone to publication, attrition and selection bias, which can affect the validity of the results. In addition, the impact of differences in the baseline characteristics, meniscal preservation techniques, surgical fixation types, concomitant procedures, and follow-up times on the outcomes could not be analyzed in this meta-analysis because of the limited data availability. Finally, the small sample size and subjective scoring system may introduce inconsistencies to the study results.
In conclusions, although limitations occurred in this work, this is a literature review and meta-analysis to provide a comparison between medial MAT and lateral MAT patients. According to our pooled data, improved clinical outcomes were observed for the lateral MAT patients compared with the medial MAT patients with regard to the KOOS and IKDC scores. The follow-up MRI results indicate that the extent of graft extrusion was greater in the lateral MAT patients than in the medial MAT patients. Although significant difference were not detected between the 2 groups, the medial MAT patients were more prone to failure than the lateral MAT patients. High-quality prospective comparative trials with larger sample sizes are required to further evaluate the differences between medial MAT and lateral MAT patients.
Withdrawal policy
By submission, the author grants the journal right of first publication. Therefore, the journal discourages unethical withdrawal of manuscript from the publication process after peer review. The corresponding author should send a formal request signed by all co-authors stating the reason for withdrawing the manuscript. Withdrawal of manuscript is only considered valid when the editor accepts, or approves the reason to withdraw the manuscript from publication. Subsequently, the author must receive a confirmation from the editorial office. Only at that stage, authors are free to submit the manuscript elsewhere.
No response from the authors to all journal communication after review and acceptance is also considered unethical withdrawal. Withdrawn manuscripts noted to have already been submitted or published in another journal will be subjected to sanctions in accordance with the journal policy. The journal will take disciplinary measures for unacceptable withdrawal of manuscripts. An embargo of 5 years will be enforced for the author and their co-authors, and their institute will be notified of this action.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 18, 2015.
- Accepted March 9, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.