


Clinical Presentation
A 69-year-old man was referred to our hospital due to the identification a mass in the right upper quadrant by physical examination at a local infirmary. The patient had no clinical symptoms, but a subtle, smooth mass of approximately 10 cm with medium hardness in the right upper quadrant was found upon medical examination. All of the adrenal-related hormones, laboratory tests, and serum tumor markers in the patient were within normal limits. Ultrasonography (US) (Figure 1A), dynamic contrast-enhanced computed tomography (DCE-CT) (Figures 1B-1D), and magnetic resonance imaging (MRI) (Figures 1E-1G) of the upper abdomen were advised. In addition, pathological examination was performed to determine the nature of the mass at the boundary (Figures 2A-2B).
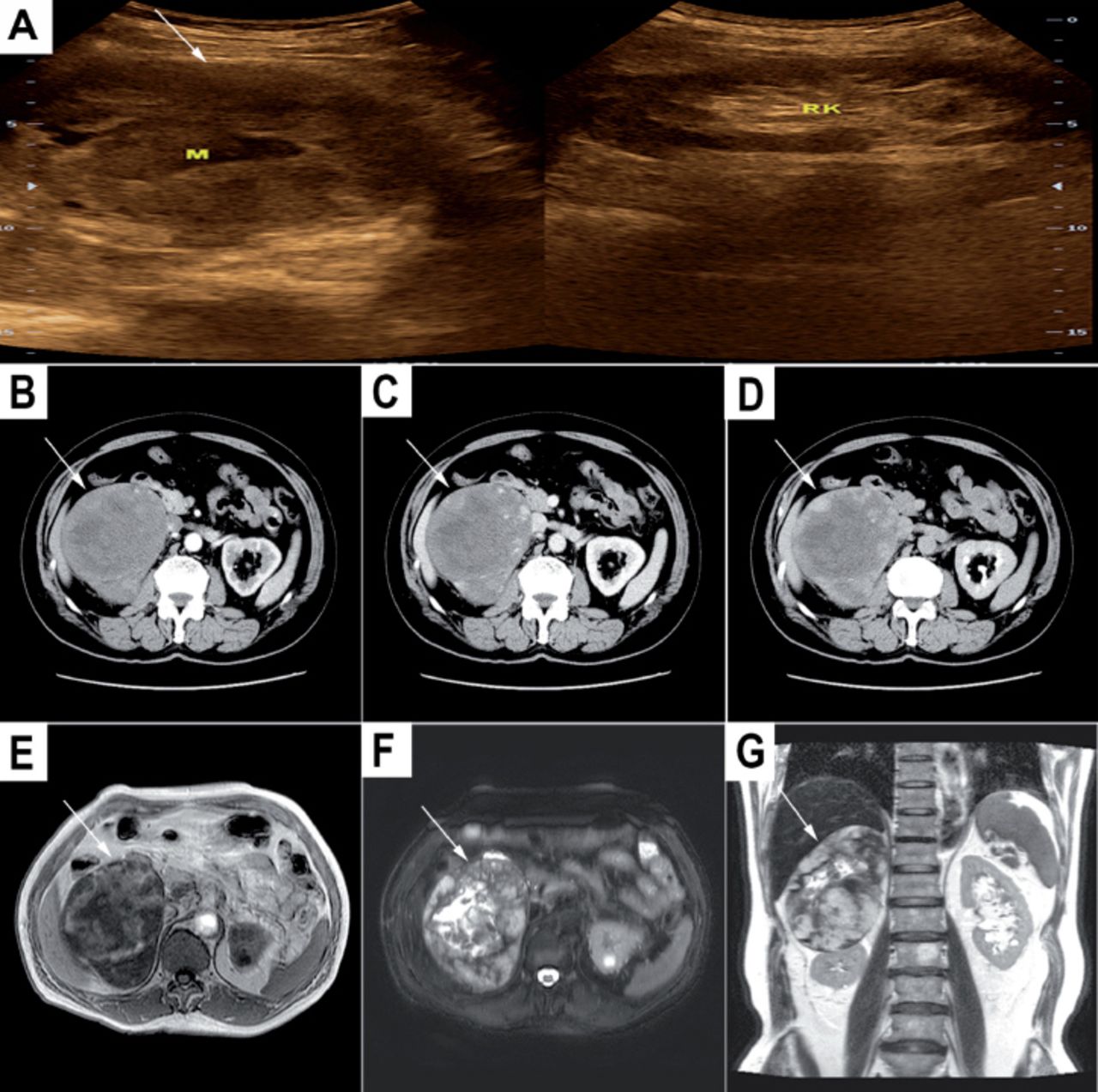
Ultrasonography showing: A) Right suprarenal region, a definite border, cystic-solid mass (arrow) with homogeneous echogenicity. (M - mass, RK - right kidney). Dynamic contrast-enhanced computed tomography showing: B) Mass (arrow) in the arterial phase, peripheral and nodular clumps of contrast. C) and D) Mass (arrows) in the portal venous phase and delayed phase, centripetal enhancement. Magnetic resonance imaging showing: E) T1-weighted imaging transversal sections, a well-defined contour, large in size, mainly low signal intensity mass (arrow). F) T2-weighted imaging transversal sections, mainly a high signal intensity mass (arrow) with a node or strip of low signal intensity inside. G) T2-weighted imaging coronal sections, the right lobe of the liver and the right kidney were partly displaced by the lesion (arrow).
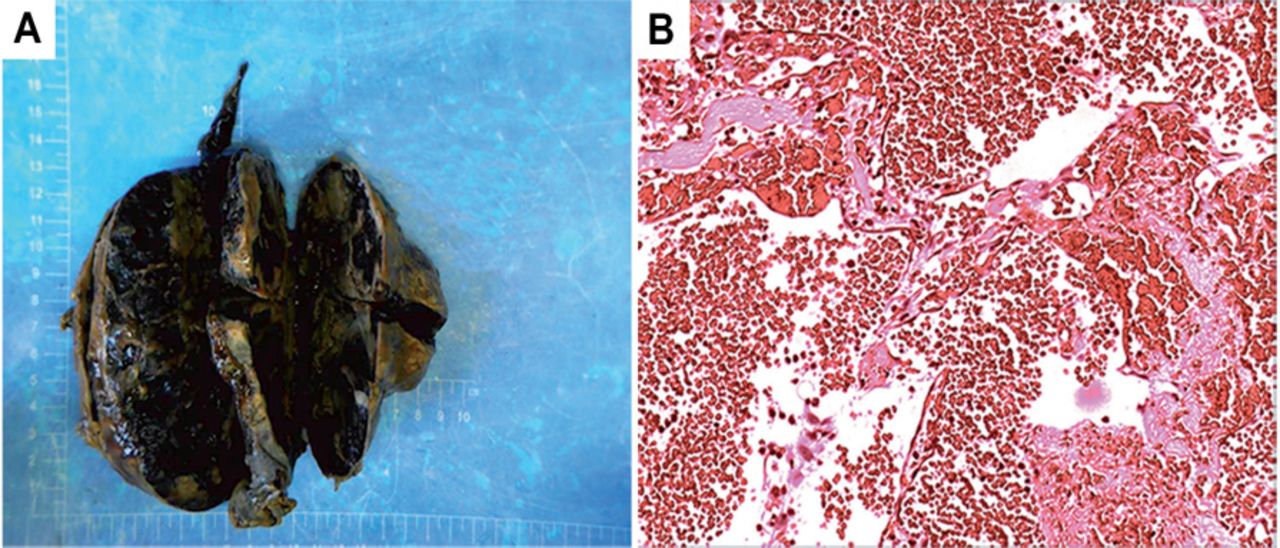
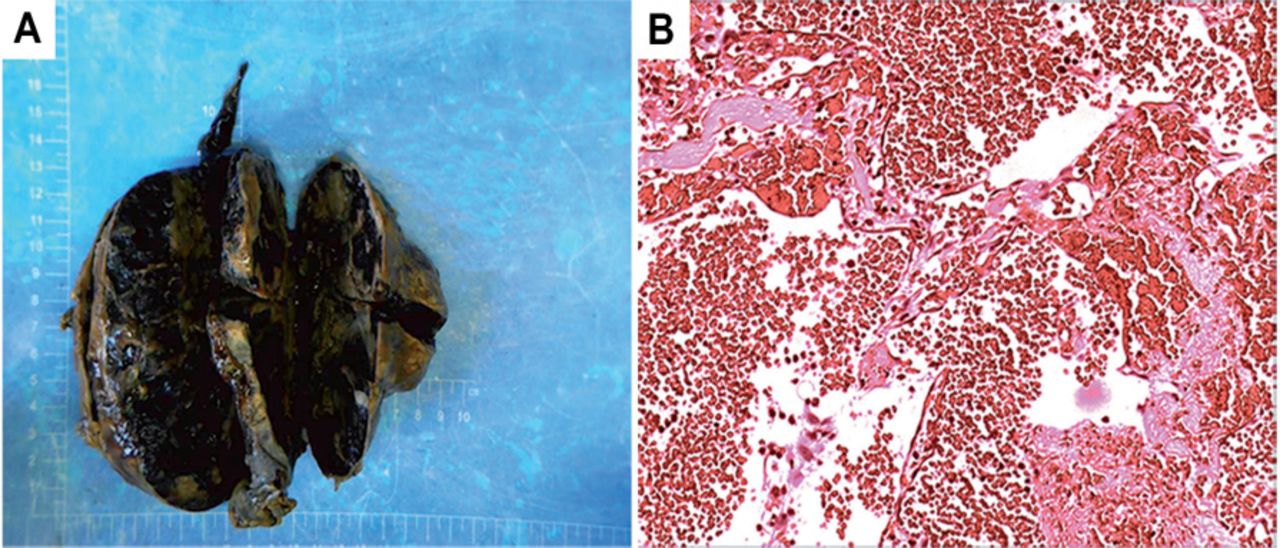
Pathology image showing: A) The gross section of the specimen was grayish yellow and had a dull red interphase, which showed focal red-purple hemorrhagic and cystic areas. B) Microscopically (hematoxylin and eosin staining, ×400), dilated, blood-filled vascular spaces were observed.
Questions
What were the abdominal US, DCE-CT, and MRI scan findings?
What is the likely diagnosis?
What is the management in this case?
Answers
The US (Figure 1A), DCE-CT (Figures 1B-1D), and MRI (Figures 1E-1G) showed a definite border of a heterogeneous mass in the right suprarenal region, that was 13.8 × 10.0 cm. On DCE-CT (Figures 1B-1D), peripheral and nodular clumps of contrast appeared in the arterial phase (Figure 1B), followed by centripetal diffusion of contrast on the next portal venous phase (Figure 1C) and delayed phase (Figure 1D). However, a strip of regions without enhancement was found in the center of this giant lesion during the dynamic scanning. Based on the MRI (Figures 1E-1G), some regions of necrosis and cystic changes were found in the center of the mass.
According to the medical history and preoperative imaging findings, a clinicoradiological diagnosis of adrenal gland hemangioma was considered, which was further confirmed after surgical removal of the tumor mass (Figure 2A) and histopathological examination (Figure 2B).
On account of the large size, possibility of malignancy, and risk of rupture, surgical resection was recommended. An open surgical excision was chosen, given the condition of the patient. The patient recovered well postoperatively and was discharged 7 days later.
Discussion
A hemangioma originating from the adrenal gland is an uncommon benign tumor. Since it was first described in the mid-1950s, only a few cases have been reported to date.1 The pathogenic factors of adrenal hemangioma are still not clear. On histopathological examination, adrenal hemangiomas are generally cavernous and rarely capillary in nature. Cavernous hemangiomas are expanding massive blood-filled sinusoidal channels that make inroads on and replace normal tissues. In addition, the presence of multiple vascular cavities in the periphery is specific, which accounts for the feature nodular contrast enhancement pattern of the periphery observed on imaging.2 Immunohistochemical inspection has shown that vessels are arranged with vascular endothelial cells, which are positive for CD31, CD34, and blood coagulation factor VIII, further indicating their endothelial nature.1 Adrenal hemangiomas are mostly unilateral lesions that are mainly found in women aged 50-70 years old. Their diameter ranges from 2 to 25 cm, the majority of which are more than 10 cm. Our patient was a 69-year-old man with a unilateral lesion of approximately 14 cm in diameter; thus, the patient age and lesion size were within the usual range. Typically, nonspecific clinical symptoms are present, unless the hemorrhage causes pain or the space-occupying effect influences the adjacent structures. Our patient had no clinical symptoms, possibly because the majority of the adrenal cavernous hemangioma was nonfunctional.
The sonographic characteristics of a hemangioma are usually nonspecific. Contrast-enhanced CT and MRI show features of peripheral spotty contrast enhancement with centripetal enhancement. This enhancement feature plays a crucial role in diagnosing an adrenal hemangioma,3 which is similar to those of hemangiomas in other anatomic locations, such as the liver. The enhancement pattern of this case was consistent with the typical enhancement pattern. On the contrary, some cases show no obvious enhancement in any phases or other patterns of enhancement, as reported by Peng et al,3 making the diagnosis more difficult.
Clinical guidelines have been formulated to provide a reference for clinicians to determine which types of adrenal hemangiomas should receive surgical resection at present. Tumor size, functional status, and imaging characteristics are major factors to be considered in these guidelines. Resection is usually recommended for all functioning lesions, together with those indicating a potential malignancy. The features for recommending a surgical resection are as follows: 1) a median lesion size greater than 4 cm (with the threshold ranging from 2.5 to 6 cm); 2) heterogeneity; 3) density >20 HU (Hounsfield Unit); 4) delayed flushing on enhanced CT scans; and 5) growth during the follow-up.4 Laparoscopic adrenalectomy or open surgery are the options for an adrenal mass. An open surgical excision was chosen in the present case, considering the large size, possibility of malignancy, and risk of rupture.
In conclusion, we report a rare case of a nonfunctioning adrenal hemangioma. This case reminds us that an adrenal hemangioma should be part of the differential diagnosis for adrenal neoplasms in clinical work. Contrast-enhanced CT and MRI showing features of peripheral spotty contrast enhancement with centripetal enhancement play an important role in diagnosis. We recommend individualizing the treatment based on tumor factors, patient factors, as well as the experience of the operator for adrenal cavernous hemangioma.
Acknowledgment
The authors are grateful to Dr. Ding Zhang from the Department of Pathology for preparing and reviewing the pathological images. In addition, the authors acknowledge Dr. Hong-Gang Yuan for his participation in the surgical part of the treatment.
Footnotes
Notice: Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42846.
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.