


Abstract
Objectives: To compares the effectiveness and impact of high inferior mesenteric artery (IMA) versus low IMA ligation on 5-year survival, lymph node yield rates, and peri-operative morbidity and mortality.
Methods: The databases of Educational Resources Information Centre (ERIC), the Web of Science, EBSCO and MEDLINE were searched using MeSH terms ‘colorectal cancer’, ‘inferior mesenteric artery’, ‘high ligation’, ‘low ligation’, ‘mesenteric lymph nodes’, ‘prognosis’, and ‘survival’. Only clinical studies were selected and review articles and meta-analysis were excluded. In cases of duplicate cohorts, only the latest article was included. Irrelevant articles and the articles on both right and left sided CRC were excluded. The finally selected studies were analysed for the defined end-point outcomes.
Results: The published data has shown that high IMA ligation improves the yield of harvested lymph node that allows accurate tumor staging and a more reliable estimation of prognosis. High ligation was not found to be positively correlated with increased anastomotic leakage or impaired genito-urinary function. However, high ligation demands advanced surgical expertise and longer operating time. There was no significant difference in 5-year survival rates for both techniques. Some studies have reported fatal complications of high ligation such as proximal bowel necrosis.
Conclusion: Although there is no consensus, this research signals the routine use of high ligation for left-sided CRC. However, the published fatal complications following high ligation and no significant difference in 5-year survival rates demand more studies to establishing a unified protocol.
Colorectal cancer (CRC) is the 3rd leading cause of cancer-related death,1 with age-adjusted rates of 26.6/100,000/year in women and 40.0/100,000/year in men.2 An escalating incidence of CRC is partly due to the association of some of the recently reported risk factors such as diabetes mellitus3 and smoking,4 and partly due to the rigorous cancer screening protocols for early detection.5 The invasiveness of gastrointestinal cancers including small bowel and CRC are primarily reflected by local and distant metastases.6,7 Left-sided CRC is estimated to account for just under two thirds of all colorectal cancers.8-10 The standard surgical technique for curative resection of left-sided colon cancers includes the division of inferior mesenteric vessels and resection of tumour with wide excision of the colonic mesentery.11 A substantial number of the lymph nodes draining distal colon are situated along inferior mesenteric vessels and ultimately drain into mesenteric and aortic lymph nodes. The level of arterial ligation can influence the extent of sympathetic nerve injures, impair genito-urinary function due to injury to superior hypogastric plexus, the extent and yield of lymphadenectomy, and can affect distal colonic anastomosis.12,13 The extent to which the mesenteric lymph nodes should be removed is debatable and there is no agreement on the level of arterial ligation during surgery for left-sided CRC.14-16 Historically, inferior mesenteric artery (IMA) is either ligated at its origin from aorta (high ligation) or below the origin of left colic artery (low ligation). Proponents of high ligation maintain that this approach guarantees a sufficient oncological resection by increasing the number of harvested lymph nodes.17 The histological analysis of greater number of lymph nodes might improve the staging accuracy of cancer that can reflect more reliable prediction of prognosis. Furthermore, some clinical studies have advocated that high ligation of IMA may provide a secure and tension-free anastomosis due to complete mobilization of the proximal colonic limb.18 However, this hypothesis has been challenged by other studies which showed that high ligation of IMA may compromise blood flow to the anastomosis.19,20 At the same time, high ligation also requires advanced surgical skills and a longer operating time. Several studies has purported that high IMA ligation did not improve the 5-year survival rates of patients with rectosigmoid or rectal cancers as compared to low IMA ligation.21-23 Existing body of literature has not shown consensus about a unified surgical approach for either high or low IMA ligation for left-sided CRC.24 There is a paucity of published clinical trials that have scientifically rationalized the significance of either surgical approach. This systematic review objectively explored and compared the existing data about the effectiveness and safety of high with low ligation of IMA by evaluating 3 outcome measures: 1) The 5-year survival rates, 2) Lymph node retrieval rates, and 3) peri-operative morbidity and mortality including anastomotic leakage and nerve injury.
Methods
Study design including eligibility criteria and information sources for systematic review
During October 2015, the databases of Educational Resources Information Center (ERIC), the Web of Science, EBSCO and MEDLINE were searched using MeSH terms ‘colorectal cancer’, ‘inferior mesenteric artery’, ‘high ligation’, ‘low ligation’, ‘mesenteric lymph nodes’, ‘prognosis’, and ‘survival’ for English language articles published during 1990-2015. The reference lists of all these potentially eligible studies were further reviewed. Only clinical studies were included and review and meta-analysis were excluded from this search. Both qualitative and quantitative investigations were selected for inclusion. In cases of duplicate cohorts, only the latest article was included. Irrelevant articles and the articles about both right and left sides of CRC were excluded from this search.
Synthesis of results
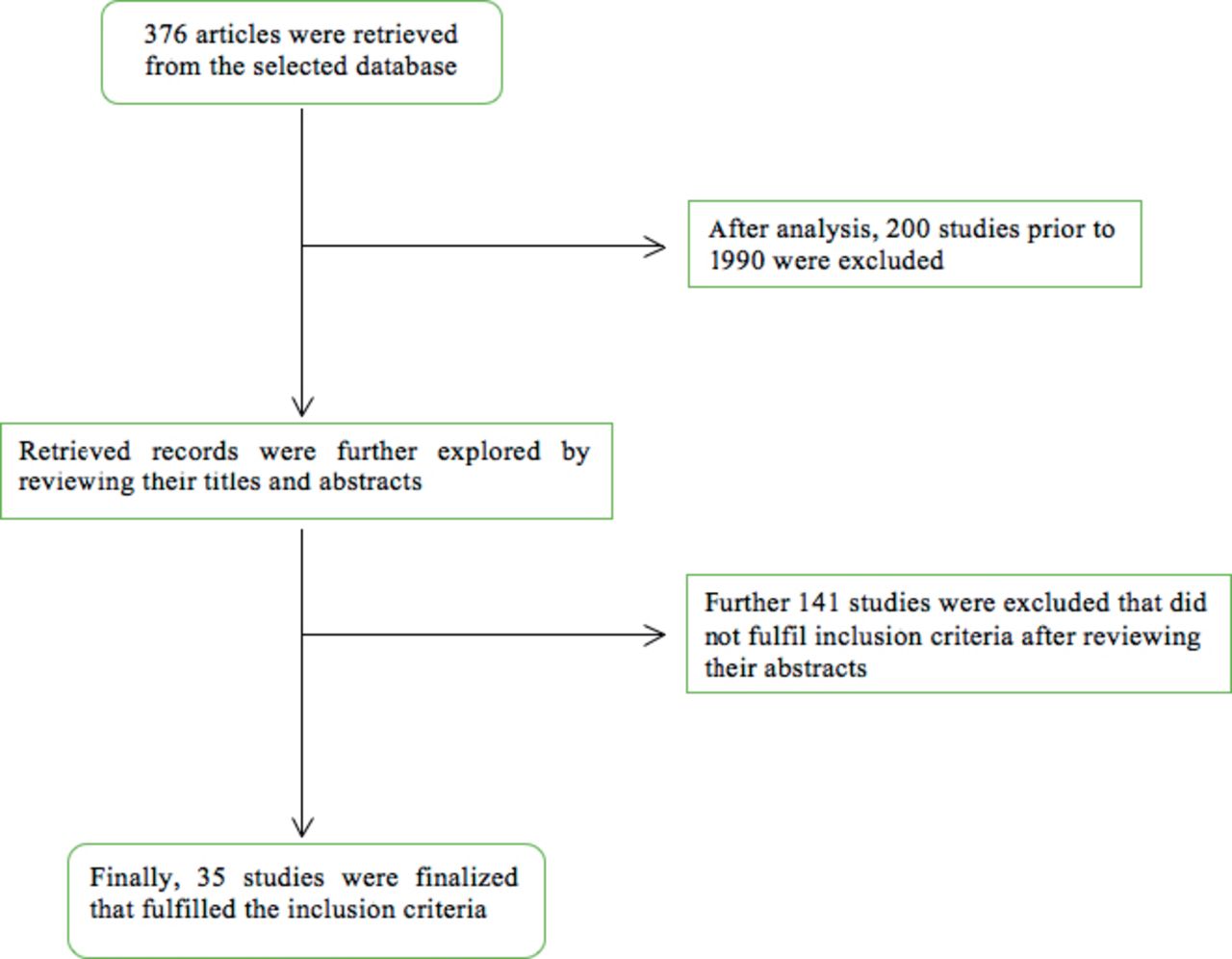
A schematic flowchart illustrating the selection process and final outcome is shown in Figure 1. There was no selection bias as this search did not involve any selective reporting during the systematic review of literature. The quantitative data from the main clinical studies selected in this systematic review are summarised in Table 1.

Schematic presentation of selection of studies about high and low ligation of inferior mesenteric artery for left-sided colorectal cancer
Summary of the quantitative data from main clinical studies on high and low ligation of inferior mesenteric artery for left-sided colorectal cancer.
Results
Initial search yielded 376 results. The data were finally selected from 35 articles about the left-sided CRC. The details of this search in terms of 5-year survival rates, lymph node retrieval rates, and the peri-operative morbidity and mortality including anastomotic leakage and nerve injury are elaborated in the following sections.
Literature review for high and low IMA ligation paradigm. a) The 5-year survival rates
A number of clinical trials in Japan have signalled an improved cancer-related survival with high IMA ligation.25-27 However, this improved survival might have been influenced by lateral pelvic lymphadenectomy, an additional surgical step that was performed in all these studies. A study by Read et al28 performed 1107 high IMA ligation and 1154 low IMA ligation operations for primary CRC at the Columbia-Presbyterian Hospital, New York, USA. They found comparable mortality rates of 4.2% for high and 5% for low IMA ligation and deduced that the level of IMA ligation had no impact on the 5-year survival rates for Duke’s A left-sided colon cancers. For Duke’s B cancers, authors reported 5-year survival rates of 83.9% and 73.9% for high and low ligation, respectively (p<0.01). For Duke’s C colon cancers, high IMA ligation improved 5-year survival rates up to 52.9%, in contrast to 45.2% for low IMA ligation (p<0.05). Finally, no significant difference in 5-year survival rates could be identified for Duke’s C2 stage cancers. Exploring from another perspective, the level of arterial ligation did not affect survival rates in cases where 5 or more lymph nodes were involved. This finding resonates well with the previous studies which showed that the curative advantage of high ligation was lost in cases of Duke’s C2 cancers with metastases to apical lymph nodes.29,30
A study by Adachi et al26 found 1% incidence of apical lymph node metastases from distal CRC and concluded that the level of arterial ligation could not affect the 5-year survival rate (83.2 % for high ligation and 91.5 % for low ligation). This study recommended to remove only peri-colic and intermediate lymph node groups in patients with no serosal or macroscopic lymph node invasion. Nevertheless, intra-operative judgement of lymph node involvement is not perceived to be reliable.29 In another study, Surtees at al22 from St. Mark’s Hospital compared the survival rates of 2 groups of patients with Duke’s C stage of rectal cancer who were treated by high and low IMA ligation. The mean of harvested lymph nodes was greater in patients with high IMA ligation; 14.1 for high and 11.9 for low ligation. The 5-year survival rates of 64 % for high and 54 % for low ligation did not demonstrate significant differences between the high and low ligation groups. Authors could not find improved survival rates in patients with Dukes’ C2 tumours treated by low IMA ligation.
b) Lymph node yield
Lymph node invasion is a key determinant of prognosis for survival following surgery for CRC. A study by Kanemitsu et al27 showed that “high ligation of the IMA allows curative resection and long-term survival in patients with cancer of the sigmoid colon or rectum and nodal metastases at the origin of the IMA”. Alici et al17 performed high ligation on 103 patients with CRC and prospectively assessed the number and status of apical lymph nodes in order to determine the risk of tumour involvement and the impact on anastomotic integrity. A mean of 14.5 ± 7.1 of non-apical and 4.4 ± 3.2 of apical lymph nodes were harvested; whereas tumor invasion was observed in 6 (5.8%) cases. Seven (8.3%) patients had anastomotic leak and there was no mortality in this study. Due to high rate of apical lymph node invasion and a low anastomotic leak, authors of this study recommended routine high IMA ligation for distal CRC. In another observational study by Charan at el,31 conducted on 60 patients with left-sided colon and rectal cancers, a median nodal yield of 33 high and 25 low ligation was observed (p=0.048). This study showed a better overall median survival by high IMA ligation (62 months) than low ligation (42 months).
The compelling reason for conducting high IMA ligation surgery is considered to be the expected increased lymph node yield and thus the improved accuracy of tumor staging. The knowledge regarding the cancerous invasion of central lymph nodes at the origin of IMA is the most significant predictor of disease-free survival.19 A study by O’Connell et al32 showed the 5-year survival rates of 27.9% of patients with IMA nodal metastases. In this study, 43 of 1,389 (3.1%) patients undergoing high ligation showed IMA nodal metastases. Although patients with IMA node metastasis were found to have increased tumor recurrence and metastasis, 25.6% of these patients remained disease free after high IMA ligation and apical nodal dissection during a minimum follow-up of 5 years. Authors maintained that if low IMA ligation was performed for these patients with proven IMA node metastases, some of the metastasized lymph nodes would have been left in situ, with no perceived benefits of curative surgery. Another study by Bonnet et al33 has concluded that low IMA ligation could leave behind as much as 9% (8/90) of metastasized apical lymph nodes in patients with left-sided colorectal cancers.
Literature has shown low survival rates of patients demonstrating IMA nodal metastases from left-sided colorectal cancers; the 5-year survival rates ranging from 18.7% to 38.5%, as opposed to 63.6% to 73.4% for patients who did not have IMA nodal metastases.23,32 Similarly, another clinical trial reported that the 5-year survival rates of patients with Dukes stage C were directly correlated with the level of lymph node invasion; 68.2% with marginal node, 25% with intermediate node, and 30% with central node metastases.34 These findings from literature have echoed the value of knowledge about the status of apical lymph nodes in determining accurate cancer staging and prognosis.
c) Anastomotic integrity and damage to superior hypogastric plexus following high and low ligation of IMA
The incidence of anastomotic leak after anterior resection has been estimated to range from 2.2% to 12%.32,35 Several clinical studies have shown that the surgical technique of high IMA ligation did not lead to increased anastomotic leakage rates and provided adequate length of bowel for performing a tension-free anastomosis low in the pelvis.36,37 From this perspective, Rutegård et al38 reviewed data from the Swedish Colorectal Cancer Registry of all patients with rectal cancers treated with anterior resection 2007 to 2009. The correlation between high IMA ligation and anastomotic leakage was explored by using a logistic regression model. This study reported symptomatic anastomotic leakage in 81 (9·9%) of 818 patients with high ligation and 108 (9·8%) of 1101 with low ligation. “Overall, the use of a high ligation was not associated with a higher risk of anastomotic leakage (odds ratio [OR] 1·00, 95% confidence interval 0·72 to 1·39)”. Another study has also endorsed the safety and effectiveness of high IMA ligation, with no increased mortality and morbidity.19
In sharp contrast to the aforementioned findings, Tsujinaka and co-workers have warned regarding the potentially fatal outcome of proximal bowel necrosis following high IMA ligation.39 In their retrospective study, they found proximal bowel necrosis in 6/302 patients following high ligation (2.0%). On the other hand, they did not report a single case of proximal bowel necrosis in other group of 107 patients with low IMA ligation. Univariate analysis showed that advanced age, cerebrovascular disease, and hypertension were significantly and positively correlated with proximal bowel necrosis; whereas multivariate analysis identified cerebrovascular disease as an independent predictor of proximal bowel necrosis. This underscores the importance of individualizing patients with left-sided colorectal cancers while deciding on the level of arterial ligation as comorbidity play a significant role in the final outcome.
Mari et al40 have registered a multi-center HIGHLOW randomised controlled trial where patients will be randomly recruited to high or low IMA ligation during laparoscopic anterior rectal resection with total mesorectal excision for rectal cancer. The primary end-point measure would be to estimate the incidence of post-operative genito-urinary dysfunction, and secondary end-point measure would be the assessment of the incidence of anastomotic leakage in both high and low ligation groups. This randomized controlled trial will provide objective evidence of the merits and demerits of both levels of arterial ligation and will determine the modality with better-preserved post-operative genito-urinary functions.
Controversies
A study by Yasuda et al41 has shown that low tie with lymph node dissection is anatomically less invasive and is not inferior to high IMA tie in terms of long-term prognosis. The researchers preferred low IMA ligation due to its less invasive degree of surgical dissection. Furthermore, they pointed out that high ligation may lead to compromised perfusion of colonic anastomosis and the potential impairment of anorectal function. Another study by Uehara et al42 could not record significant differences in survival rates between the 2 groups for lower rectal cancers. At the same time, investigators could not demonstrate any beneficial effect of prophylactic lymphadenectomy at the root of IMA.
In conclusion, High ligation of IMA for rectal and left-sided colonic cancers provides a higher number of harvested apical and non-apical lymph nodes that permits accurate staging of left-sided colorectal cancer. This in turn leads to more reliable estimation of prognosis. High ligation allows for en-bloc dissection of apical nodal metastases at and around the origin of IMA, while enabling a tension-free anastomosis. However, high ligation demands advanced surgical expertise and longer operating time. Routine use of high ligation is not associated with an increased rate of anastomotic leak. Overall, there is no significant difference in the 5-year survival rates between high and low ligation for left-sided colorectal cancers. There is some evidence of fatal proximal bowel necrosis following high IMA ligation. This emphasises the need to carefully select patients tailored to address every individual’s co-morbidity such as age, cerebrovascular disease, and diffuse atherosclerosis. Nevertheless, more rigorous randomized clinical trials and observational studies are needed to validate these findings.
Footnotes
Disclosure. Author has no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.