


Clinical Presentation
A 53-year-old male who presented to the emergency department complaining of abdominal pain was examined by abdominal computed tomography (CT), with pre-diagnosis of acute abdomen after ultrasound (US) examination without any pathological findings. He did not have any of the possible causes of isolated mesenteric artery (SMA) dissection, which can be counted as diabetes mellitus, hypertension fibromuscular dysplasia, atherosclerosis, cystic medial necrosis, and elastic tissue abnormalities like Marfan and Ehlers-Danlos syndromes. There was no abdominal surgery or trauma in his medical history. He had 4 hours of acute abdominal pain, which was exacerbated with food intake. He received 2x 500 mg tablets of paracetamol before admitted to the emergency department without any change in his symptoms. Computed tomography revealed isolated superior SMA dissection extending to the segmental branches (Figure 1) without any additional vascular pathology such as aneurysm of the abdominal aorta. There were no accompanying CT findings, such as increased thickness of the bowel wall, ascites or heterogeneity of mesenteric fatty tissue supporting intestinal ischemia, and no indications of acute abdomen, such as obstruction, appendicitis, or mesenteric ischemia.

Sagittal CT image shows isolated superior mesenteric artery dissection extending to the segmental branches (arrow).
Questions
What is the likely diagnosis?
What is the etiology of this condition?
What is the management?
Answers
The final diagnosis is spontaneous isolated SMA dissection.
The etiology of spontaneous isolated SMA dissection has not yet been clarified, however, arteriosclerosis, medial degeneration of the arterial wall, cystic medial necrosis, fibromuscular dysplasia, trauma, and inflammation are blamed as the potential etiologic factors. Moreover, the coexistence of hypertension and isolated SMA dissection is reported as 30% in regard to the literature.1,2
Low molecular weight heparin was administered at a dosage of 0.6 mg. As there was no improvement in clinical status, the occluded distal vascular segments were treated with thrombolytics by the endovascular route initially to reduce the thrombus load. During the following runs it was noticed that the patent lumen was compressed more than 80% at mid-SMA and there was no change in the patients’ complaints. Hence emergent endovascular stenting (ES) was performed proximal to the dissection (Figure 2). The patency and the flow of the SMA returned to normal after ES and the patient had no symptoms during the 6-month follow up period.
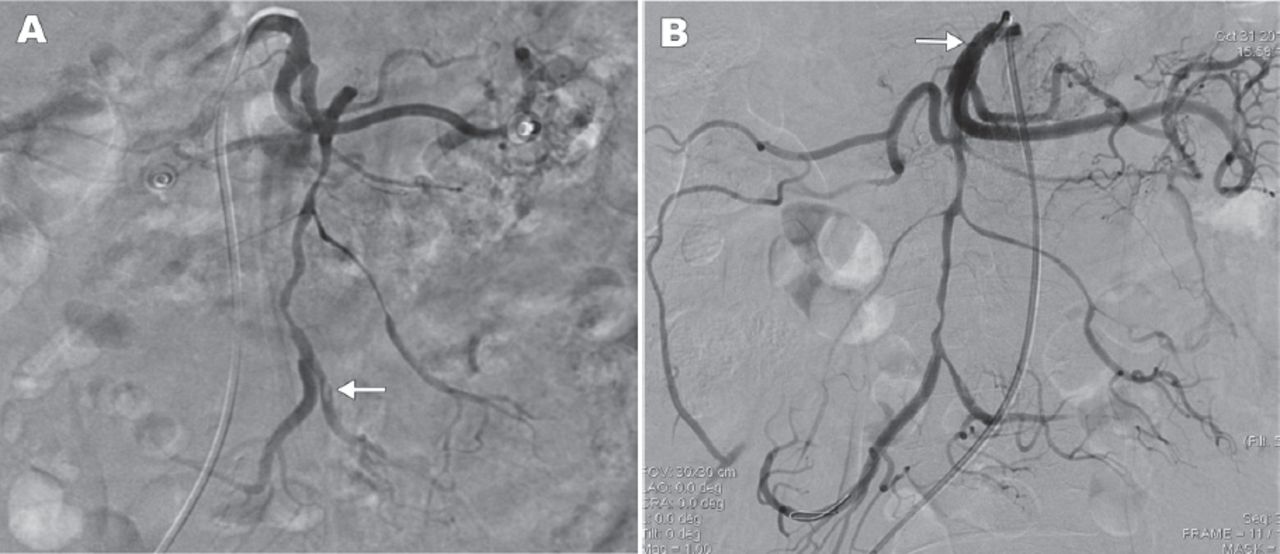
Digital subtraction angiography images showing: A) Segmental stenosis due to dissection at SMA and its distal braches. Focal thrombus at the distal branch of superior mesenteric artery (SMA) (arrow), and B) Restored patency at proximal SMA after endovascular stent placement (arrow).
Discussion
Isolated SMA dissection without associated aortic dissection is a rare disorder. The aim of the therapy is to increase the patency rate of the affected lumen and to prevent extension of the dissection. Treatment involves conservative management, anticoagulation, ES, or surgery. Medical treatment is initially used if bowel perfusion still continues. Endovascular stenting is performed if the patient has bowel ischemia or compression of the patent lumen by more than 80%. Emergent surgery is indicated when ES is unsuccessful, or when thrombosis of the SMA gives rise to bowel necrosis, hemorrhage, or peritonitis.1,3
Isolated SMA dissection should be included in the differential diagnosis of middle aged or older patients who present with acute abdomen, as it can be fatal if early diagnosis and treatment are not considered.
References
* References should be primary source and numbered in the order in which they appear in the text. At the end of the article the full list of references should follow the Vancouver style.
* Unpublished data and personal communications should be cited only in the text, not as a formal reference.
* The author is responsible for the accuracy and completeness of referencesand for their correct textual citation.
* When a citation is referred to in the text by name, the accompanying reference must be from the original source.
* Upon acceptance of a paper all authors must be able to provide the full paper for each reference cited upon request at any time up to publication.
* Only 1-2 up to date references should be used for each particular point in the text.
Sample references are available from:
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.