


Abstract
Objectives: To assess the prevalence and associations of mesenteric panniculitis (MP) using multi-detector CT (MDCT).
Methods: This retrospective study included 4758 consecutive patients who underwent abdomino-pelvic MDCT between January 2012 and December 2014 at Jordan University Hospital, Amman, Jordan. Radiological database was searched for MP diagnosis and patients with suspected MP were re-evaluated by an experienced radiologist to confirm the diagnosis. Data on all patients with confirmed MP diagnosis were subsequently collected and analyzed.
Results: Computed tomography features of MP were identified in 90 patients (41 males, 49 females), a prevalence of 1.9%. Mesenteric panniculitis was identified in both asymptomatic and symptomatic patients. Malignancy was found in 28 MP patients (31%) and 44 of the MP patients (49%) had prior history of abdomino-pelvic surgery. Mesenteric panniculitis was significantly more frequently associated with prior abdomino-pelvic surgery (p=0.0001) and the likelihood of associated malignancy in patients with MP was 2.1-fold higher than in patients without MP (p=0.0013).
Conclusion: Mesenteric panniculitis can be reliably diagnosed by MDCT due to its typical CT appearance. Its identification is important because of its significant association with malignancy and because it represents one of the differential diagnoses in patients with nonspecific symptoms referred for abdomino-pelvic CT.
Mesenteric panniculitis (MP) is a term first used by Odgen et al1 in 1965 to describe a condition affecting the adipose tissue of the bowel mesentery. However, MP was actually described four decades earlier by Jura2 under the term sclerosing mesenteritis. Other names used to describe MP include mesenteric lipomatosis, mesenteric lipodystrophy and retractile mesenteritis, all of which are part of the spectrum of the same disorder.3 Proposed causes of MP include ischemia of the mesentery, infection, trauma and autoimmune response and associations with conditions such as malignancy, prior abdominal surgery, vasculitis and granulomatous disease have been reported.4,5 MP is usually asymptomatic and, when symptomatic presents with a benign course.3 Symptoms include abdominal pain, pyrexia, palpable abdominal mass and gastro-intestinal disturbances.6 Mesenteric panniculitis is best diagnosed by multi-detector CT (MDCT), which also differentiates it from other mesenteric conditions with similar CT features such as lymphoma, carcinoid tumors, desmoids tumors, metastases and infectious diseases like tuberculosis and histoplasmosis.7
The objectives of this study are to estimate the prevalence and determine the possible associations of MP diagnosed using a 128-slice MDCT in a large comprehensive study at a large university hospital in the University of Jordan. In addition, we establish the value of MDCT in the diagnosis of MP.
Methods
This retrospective study was conducted based on abdomino-pelvic CT scans performed between January 2012 and December 2014 at Jordan University Hospital, Amman, Jordan. The study was approved by the Institutional Review Board (IRB) at our hospital and adhered to the principles of the Helsinki Declaration. The IRB did not require an informed consent for this study because the research only required retrospective review of patient data and images obtained as part of clinical practice. Search for prior related research was performed in PubMed database using the keywords: mesenteric panniculitis, sclerosing mesenteritis, mesenteric lipomatosis, mesenteric lipodystrophy, retractile mesenteritis, MDCT, and CT.
Inclusion criteria were patients who underwent contrast-enhanced abdomino-pelvic CT examinations (including patients who underwent dynamic urinary tract examinations) between January 2012 and December 2014. Exclusion criteria were patients with marked ascites along with those with known mesenteric tumors potentially mimicking MP, such as carcinoid and desmoid tumors as well as mesenteric metastases. In addition, patients whose abdomino-pelvic CT reports suggested MP but, based on the opinion of the re-evaluating experienced radiologist did not present with the typical findings of MP were excluded from the analysis.
A total of 4758 consecutive adult patients who underwent contrast-enhanced (porto-venous phase) abdomino-pelvic CT examinations (including 560 patients who underwent dynamic urinary tract examinations) in the period between January 2012 and December 2014 were included in this study. There were 2077 males (mean age ± SD= 62.3 ± 13.9 years; range, 21-92) and 2681 females (mean age ± SD = 61.6 ± 15.3 years; range, 31-84). The departmental radiological database was searched for the diagnosis of MP in patients using the search term mesenteric panniculitis, a term used by all our radiologists to describe this entity. All patients whose abdominal CT scan reports contained mesenteric panniculitis were subsequently re-evaluated by an experienced radiologist to confirm the diagnosis. All CT examinations were performed on a dual-source 128-slice MDCT scanner (Somatom Definition, Siemens Medical Solution, Germany). The protocol routinely used at our department for contrast-enhanced abdomino-pelvic CT and dynamic urinary tract CT included: scanned area from dome of the liver to the symphysis pubis; tube voltage 120-140 KVP, effective tube current 210-300 mAs; collimation 0.6 mm, pitch 0.6 and gantry rotation time 0.5 seconds. All examinations were reviewed at a workstation (Work Station Syngo Multi Modalities MMWP, Siemens, Germany) on axial and coronal planes, and whenever needed in the sagittal plane with a slice thickness of 1 and 5 mms.
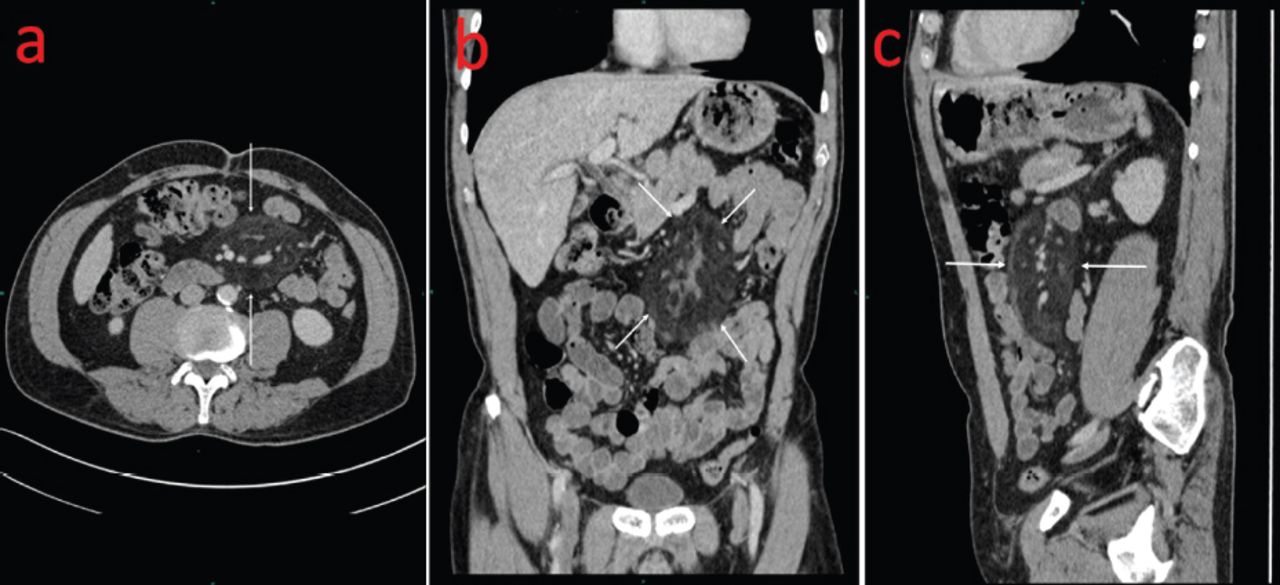
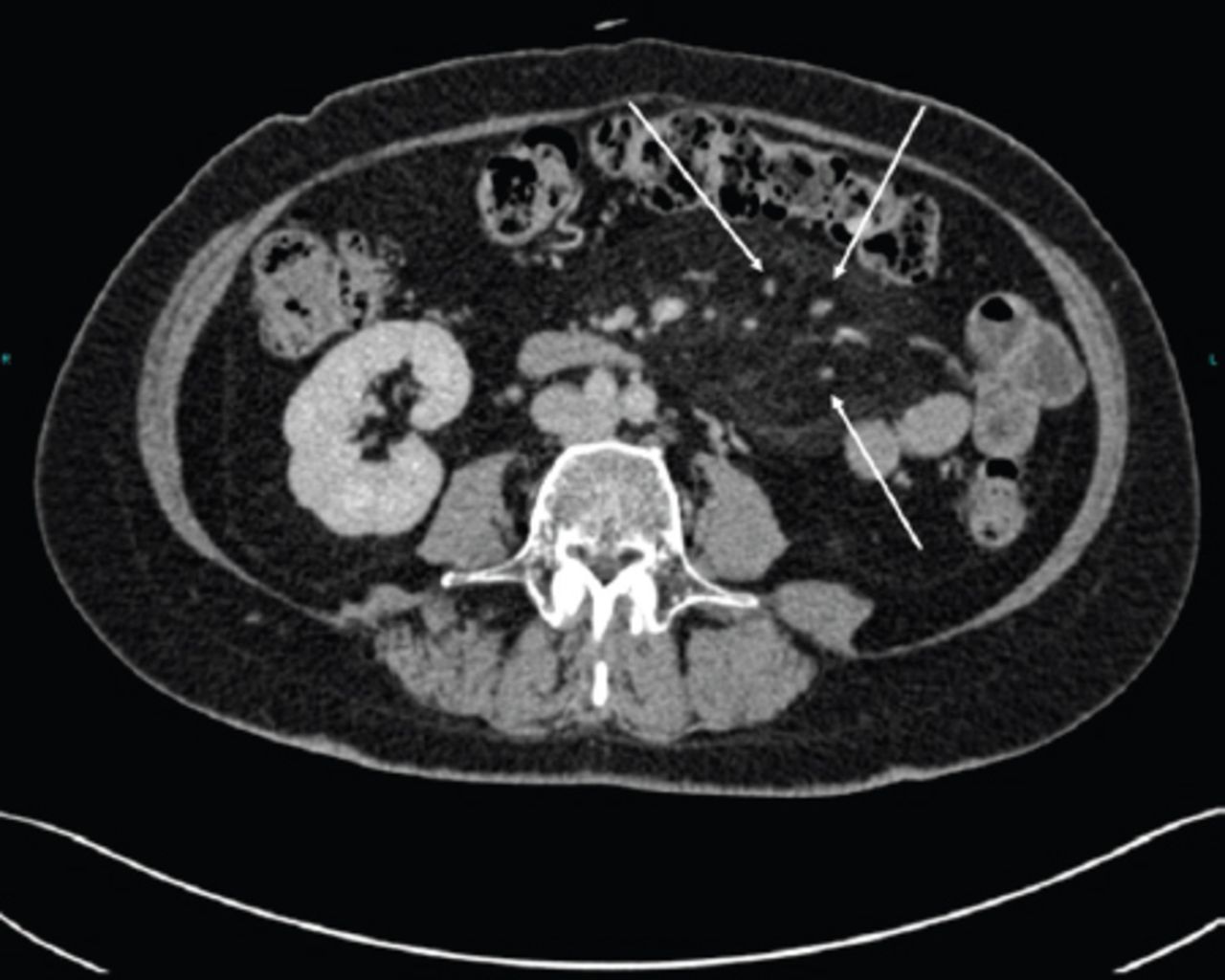
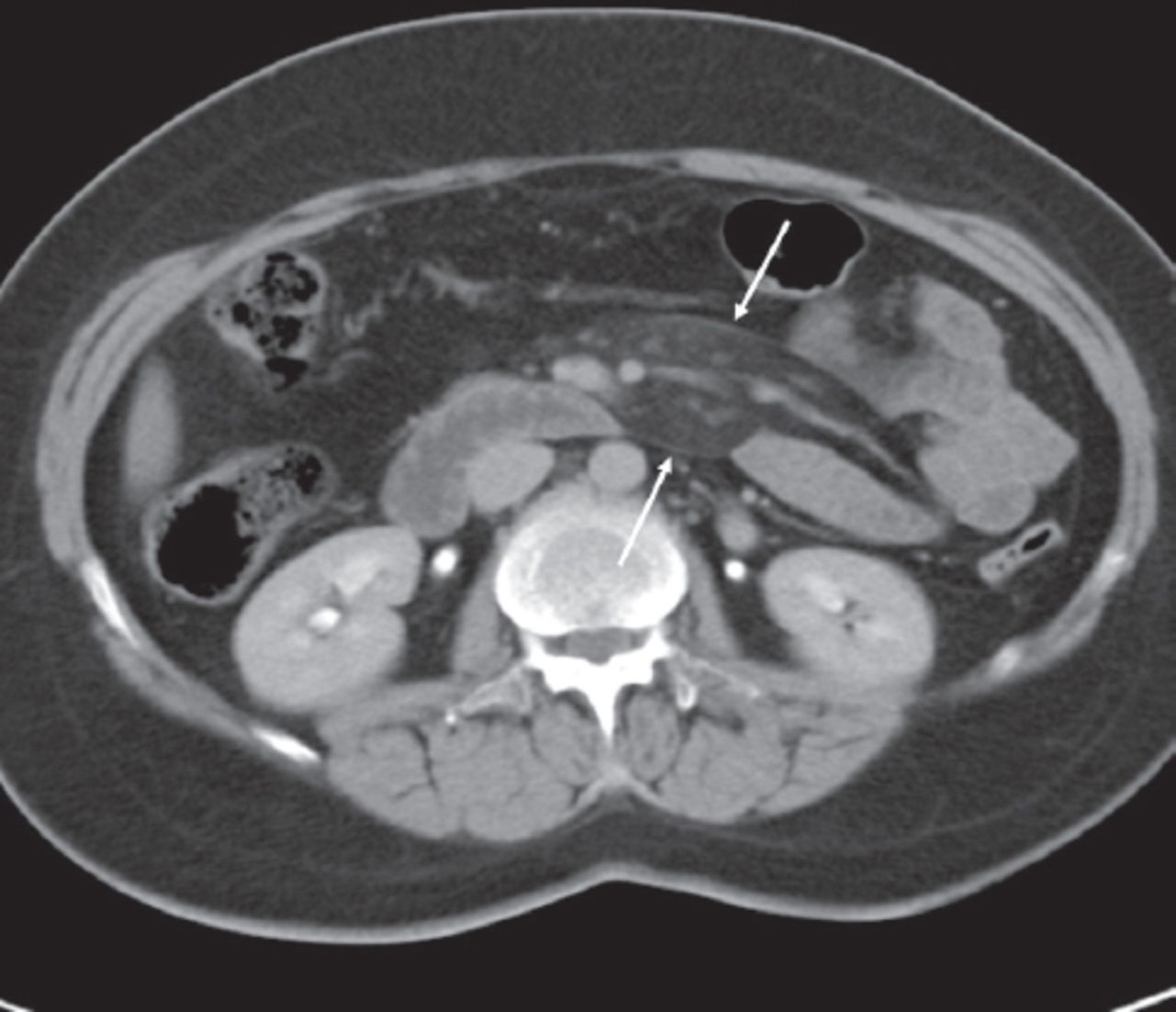
A positive CT diagnosis of MP was based on the observation of a well-defined inhomogeneous fatty tissue mass, with attenuation values higher than that of the retroperitoneal fat mostly at the root of the small bowel mesentery along with at least 2 of the typical signs of the disease according to the accepted criteria reported in the literature: mass effect on adjacent structures with no evidence of invasion (Figure 1), subcentimetric mesenteric lymphadenopathy or encasement of mesenteric vessels without vascular invasion, hypo-attenuating fatty halo around the mesenteric vessels or nodes, the so-called fatty ring sign or fatty halo sign (Figure 2) and hyper-attenuating stripe, the so-called tumoral pseudocapsule surrounding the mesenteric fatty mass (Figure 3).7 These diagnostic criteria apply to typical MP rather than the advanced condition of retractile mesenteritis where fibrosis and retraction predominate, which is a rarely found condition.

Multi-detector CT images of mesenteric panniculitis (MP) in A) axial, B) coronal, and C) sagittal reformations offer an overview of MP in a 72-year-old male patient with metastatic colon cancer and show the space occupying effect of MP on adjacent structures without evidence of infiltration (arrows).

Contrast-enhanced abdominal CT for a 64-year-old female with abdominal pain showing mesenteric vessels and nodes encased by mesenteric panniculitis and surrounded by a low attenuation fatty halo, the so called fatty ring sign (arrows).
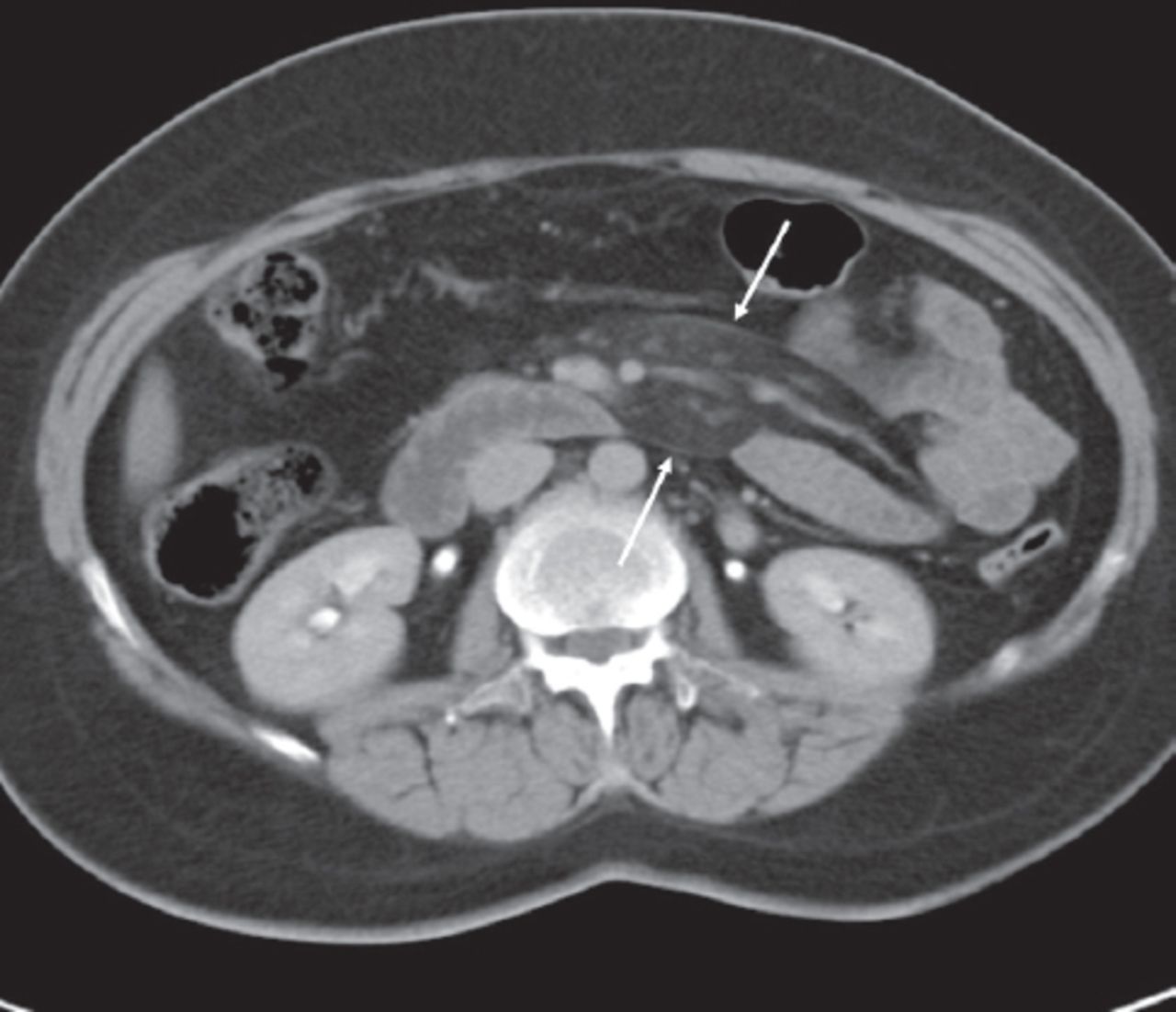
Contrast-enhanced abdominal CT for 58-year-old female with a history of breast cancer showing a hyperattenuating stripe (pseudo-capsule) delineating the outline of mesenteric panniculitis (arrows).
The medical records of all patients with the diagnosis of MP were reviewed to identify patients’ clinical history and indication for CT examination, physical examination findings, and laboratory data. The prevalence of the disease was estimated and associations with previous abdominal surgeries and coexisting pathologies, including malignancy were recorded.
Statistical analysis
Data is presented as mean ± standard deviation. Paired t-test was used to determine whether examined parameters were significantly different within the same patients. Comparison of proportions was performed using the “N-1” Chi-squared test as recommended by Campbell8 and Richardson.9 The odds ratio was calculated according to Altman.10 Data were analyzed using SPSS software for windows version 11.5. A p-value of <0.05 was considered statistically significant.
Results
Based on the CT reports of the 4758 patients included in this study, 93 patients were thought to have MP. However, the re-evaluating experienced radiologist confirmed the MP diagnosis in 90 of the 4758 patients, a prevalence of 1.9%. Three patients did not meet the criteria of MP. Of the 90 patients with documented MP, there were 41 (45.5%) males (mean age ± SD = 61.6 ± 15.3 years; range, 21-92) and 49 (54.5%) females (mean age ± SD = 62.8 ± 16.7 years; range, 38-84). The prevalence of MP in males was 2% (41/2077) compared with 1.8% (49/2764) in females, a statistically insignificant difference (p=0.61). Approximately 65% of patients with MP were ≥60 years old and only 6.6% were <40 years old.
The most common indication (46/90 [51%]) for obtaining the initial CT scan in patients with documented MP was symptoms caused by known benign or malignant disease or by illness first revealed by the initial CT scan documenting MP. Another indication in 28 patients (31%) was the performance of a follow-up CT scan in an asymptomatic patient with known illness. In 16 patients (18%), the CT scan was performed for nonspecific symptoms unrelated to any benign or malignant illness with MP being the only finding encountered on CT. These symptoms included intermittent diffuse or epigastric abdominal pain, constipation, diarrhea and vomiting, fever, weight loss and melena. The laboratory findings in these patients were unremarkable except for 2 patients who showed mild elevation of ESR levels at 55 and 65.
The fatty density mass lesion was located in the left side of the abdomen in relation to the small bowel mesentery in 85 patients (94.4%), in relation to large bowel mesentery in 2 patients (2.2%) and in the peripancreatic region in 3 patients (3.3%). The maximum transverse diameter of the fatty mass ranged from 3 to 16 cm with a mean ± SD of 10.1 ± 2.4 cm. Maximum anteroposterior diameter ranged from 1 to 9 cm with a mean ± SD of 4.8 ± 1.7 cm. The CT criteria of MP in 90 patients are summarized in Table 1.
Computed tomography characteristics of mesenteric panniculitis in 90 patients.
The CT attenuation values of the fatty mass ranged from -115 to -14 HU with a mean ± SD of -67.7 ± 23.3 HU and were significantly higher (p=0.0001) than the CT attenuation values of the adjacent normal retroperitoneal fat of the same patients ranging from -148 to -70 HU (mean ± SD of -103 ± 21.6 HU).
A prior history of abdomino-pelvic surgery was present in 44 (49%) of the 90 patients with MP of whom 9 (10%) had more than one abdomino-pelvic surgery (Table 2). The prevalence of MP in patients with prior abdomino-pelvic surgery was 9.2% (44/476) versus 1.1% (46/4282) in patients without prior abdomino-pelvic surgery, a statistically highly significant difference (p=0.0001).
Previous surgical procedures in patients with mesenteric panniculitis (n=44 patients, 53 procedures).*
Association with malignancy was found in 28 of the 90 patients (31%) with MP. Of those patients, 15 (16.7% of all MP patients) had intra-abdominal malignancy, 8 (8.9%) extra-abdominal malignancy, 3 (3.3%) lymphoma, and 2 (2.2%) leukemia (Table 3). Malignancy was concurrent with MP in the vast majority of patients (22/28 or 78.6%) who had MP associated with known malignancy. Concurrent cancers were those diagnosed within 3 months of the CT scan demonstrating MP. Five patients were considered to have past cancer since malignancy was diagnosed more than 3 months prior to MP and the patients were in remission at the time of MP diagnosis. In one patient, malignancy was diagnosed 20 months following the MP diagnosis. Overall, the prevalence of MP in patients with malignancy was 3.3% (28/855), significantly higher than the 1.6% (62/3903) prevalence in patients without malignancy (p=0.001). Moreover, the likelihood of associated malignancy in patients with MP was significantly higher than in patients without MP (odds ratio = 2.1; 95%CI=1.33-3.30, p=0.0013). Of the 90 MP patients, the disease was associated with smoking in 49 (54.4%), diabetes mellitus in 41 (45.5%), and hypertension in 51 patients (56.7%).
Malignancies identified in patients with mesenteric panniculitis.
One or more follow up abdomino-pelvic CT scans were available in 33 (36.7%) of the 90 patients with MP. The follow-up period ranged from 2.6 to 37 months with a mean ± SD of 18.6 ± 11.7 months. In 15 of the 33 patients (45.5%), the size and/or density of MP increased on the follow-up scan. The size and/or density of MP was stable in 10 patients (30.3%) while it decreased in 8 patients (24.2%).
Discussion
Our data based on over 4700 MDCT scans obtained at a large University Hospital demonstrate that the prevalence of MP of 1.9% is within the range of what has been reported in other countries after introduction of MDCT.7,11,12 In fact, more recent larger series performed using MDCT have shown that the disease is more frequently encountered than before with a prevalence of up to 7.8% suggesting that MP may not be such an uncommon finding in the MDCT era.7,11,12
In the present study, the characteristic CT features of MP were seen in most of our patients with suspected MP (Table 1) and there was an excellent agreement between the initial interpretation by board-certified radiologists with different experience levels and the experienced radiologist who reviewed all scans, suggesting that the interpretation criteria are easily implemented by the interpreting radiologists with little inter observer variability.
The association between MP and history of previous abdomino-pelvic surgery found in our study is similar to what has been reported in studies from outside the Arab region.4,5,13 In our study, prior history of one or more abdominal surgeries was documented in 49% of patients with MP and the prevalence of MP was significantly higher in patients with prior abdomino-pelvic surgery compared with those without such history (p=0.0001). Daskalogiannaki et al4 reported a history of abdominal surgery in 57%, Sabate et al5 in 52.9%, and Akram et al13 in 40% of their MP patients. The exact mechanism linking MP with surgery is not well established. It is believed that abdominal surgery among other causative factors, such as mesenteric ischemia and infections may trigger the development of nonspecific inflammatory reaction in the mesenteric fat with potential development of MP.
The association between MP and malignancy found in our study is also consistent to what has been reported in literature from outside the Arab region.4,7,12,14 Intra-abdominal malignancies, such as colorectal, urogenital, hepatobiliary and pancreatic are the most frequently encountered associations.14 Extra-abdominal malignancies, such as lung, breast and melanoma are less frequent, but well-recognized associations with MP.7,14 In our study, 28 (31%) of the 90 patients with MP had one or more malignancies distributed among various intra and extra- abdominal organs of origin (Table 3). Daskalogiannaki et al4 reported an even higher rate of malignancies in their patients with MP with extra-abdominal malignancies found in approximately half of them. Patients with known malignancy in our study had a 2-fold higher prevalence of MP compared with those without malignancy (3.3% versus 1.6%, p=0.001). Moreover, the likelihood of associated malignancy in patients with MP was 2.1-fold higher than in patients without MP. Our data is consistent with that of Sheer et al,11 who found an even higher prevalence of MP in patients with compared to those without malignancy (5.4% versus 1%, p<0.005). Using a matched pair analysis, Van Putte-Katier et al12 found a significantly higher rate of malignancy in MP patients than in age- and gender-matched controls and also found that patients with MP developed significantly more malignancies than controls during a 5-year follow-up. Taken together, the data suggests that when MP is incidentally found on abdomino-pelvic CT, the CT scan should be scrutinized to rule out any malignancy. However, the data on malignancy potentially developing subsequent to MP is inconclusive in the literature.12,15,16 Hence, it does not seem justified to subject patients with MP, especially those in whom other associations, such as abdomino-pelvic surgery may explain the MP finding, to multiple follow-up CT scans with the aim of detecting a future malignancy.12,15,16
In our study, MP was identified in both asymptomatic and symptomatic patients which is similar to what has been reported in prior studies.3,6 Interestingly, MP provided the only explanation for nonspecific symptoms in a fraction of patients referred for abdomino-pelvic CT, emphasizing the importance of identifying MP on the CT of these patients.
Follow up CT scans were available in approximately 37% of our MP patients with an average follow-up period of approximately 19 months. The size and/or density of MP remained stable or even increased in the majority of patients (76%) with regression noted in 24% of patients. This data is similar to that by Buchwald et al17 who showed that MP did not regress in 80.9% of patients. Daskalogiannaki et al4 also reported profound stability of the CT findings in 20 of 21 MP patients in whom follow up CT examinations were available within 5 months to 3 years.
Study limitations
The first limitation pertains to its retrospective nature. Secondly, we have not obtained a histopathologic diagnosis of MP in our patients since most reports have shown that MP can be reliably diagnosed using MDCT rather than open biopsy or surgery.18 Finally, it is possible that some of the associations with MP found in our study were merely due to the fact that most of our MP patients were 60 years or older and certain conditions, such as DM and hypertension are more common in this age group. It may be that such associations will not be found in a study of the prevalence of MP in younger patients in whom such conditions are much less common.
In conclusion, MP can be reliably diagnosed by MDCT due to its typical CT appearance. Its prevalence of 1.9% found in our study is well within the range of recently reported rates in the MDCT era. Mesenteric panniculitis is significantly associated with prior abdomino-pelvic surgery. Its identification is important due to its significant association with malignancy and because it might provide the only explanation for nonspecific symptoms in a fraction of patients referred for abdomino-pelvic CT. Future research should focus on determining whether MP in patients without risk factors, such as prior abdomino-pelvic surgery predisposes for development of malignancy even years after it has been observed on MDCT.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 21, 2017.
- Accepted July 25, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.