


Abstract
Objectives: To determine the associations between serum cancer antigen 15-3 levels and prognostic factors in patients with endometrial carcinomas. Additionally, we investigated the clinical utility of serum cancer antigen 15-3 levels in the selection of low-risk patients with endometrioid type, tumor size <2 cm, myometrial invasion ≤50%, and histological grade 1-2.
Methods: Ninety-six patients, who were surgically staged at Ankara Yildirim Beyazit University, Ankara, Turkey, between 2007 and 2016, were retrospectively analyzed. Demographic, clinical, and surgical characteristics were retrieved from the patients’ hospital records. A p<0.05 was considered significant.
Results: Fifteen patients had advanced (≥Stage II) disease, 14 patients had Type 2 histology, 20 patients had Grade 3 tumors, 23 patients had lymphovascular space invasion, and 10 patients had positive lymph node involvement. Serum cancer antigen 15-3 levels were significantly higher in patients with advanced (≥Stage II) disease, Type 2 histology, Grade 3 tumors, lymp°hovascular space invasion, and positive lymph node involvement (p<0.05). Serum cancer antigen 15-3 levels were also significantly correlated with tumor size (p=0.006). Serum cancer antigen 15-3 levels were significantly lower (95% confidence interval: 0.57−0.79; p=0.03) in low-risk patients compared to other endometrial carcinoma patients. A cutoff of 25.0 IU/mL was used to identify high-risk patients with a specificity of 100%.
Conclusion: Serum cancer antigen 15-3 levels significantly correlated with prognostic factors and were a useful diagnostic tool for endometrial carcinomas.
I Cancer antigen 15-3 (CA15-3) is a tumor marker of several types of cancer (for example, breast, colon, and liver) that is derived from the MUC1 gene.1 Previous studies2-5 of endometrial carcinoma (EC) patients have shown that high serum CA15-3 levels are associated with a greater disease stage and a poorer prognosis. An additional study by Hebbar et al6 demonstrated that MUC1, MUC5B, and MUC8 expression was significantly increased in EC tissues compared to normal endometrial tissues. Endometrial carcinoma represents the second most frequent gynecological cancer worldwide.7 Seventy-five percent of EC patients who are diagnosed at an early stage have a relatively favorable prognosis compared to other types of gynecological cancer. However, its prevalence is increasing, especially due to obesity in developed countries.7,8 Currently, there is no reliable screening test for EC and screening is not recommended for women without certain conditions (for example, Lynch syndrome).9 However, in order to identify tumors at an early stage and to determine their prognosis, imaging methods, tumor markers, or both have been investigated.5,10,11 The role of serum CA15-3 in ECs has been studied for >20 years and some encouraging reports have been published.2-5,12 However, the clinical utility of serum CA15-3 has yet to be fully elucidated. The aim of this study was to determine the associations between serum CA15-3 levels and prognostic factors (age, disease stage, histological type and grade, tumor size, lymphovascular space invasion [LVSI], and lymph node involvement [LNI]) in patients with ECs. Additionally, we investigated the clinical utility of serum CA15-3 levels in the selection of low-risk patients with endometrioid type, tumor size <2 cm, myometrial invasion ≤50%, and histological grade 1-2.13
Methods
The medical records of 136 EC patients who underwent staging surgery according to the recommendations of the International Federation of Gynecology and Obstetrics (FIGO) at the Ankara Atatürk Education and Research Hospital, Ankara Yildirim Beyazit University, Ankara, Turkey, between 2007 and 2016 were retrospectively analyzed.14 Forty patients whose preoperative serum CA15-3 levels were not examined were excluded. In total, 96 patients were enrolled in the study. All participants provided informed written consent. The study was approved by the Ethical Review Board Committee (Approval No=26379996/73) of Ankara Yildirim Beyazit University Faculty of Medicine, Ankara, Turkey. Research was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments.
Demographic (age, gravidity, and parity), clinical (preoperative serum CA15-3 level and endometrial dual-layer thickness on transvaginal ultrasound examination), and pathological (histological tumor type and grade, extent of myometrial invasion, tumor size, FIGO surgical stage, and LVSI and LNI statuses) data were retrieved from the patients’ charts and hospital records. Blood samples of patients were obtained prior to the surgery and the serum CA 15-3 values were determined by electrochemoluminescence immunoassay (Roche Elecsys Kits, Roche Diagnostic, Mannheim, Germany).
After associations between preoperative serum CA15-3 levels and prognostic factors of EC were examined (age, type 1 vs type 2 tumors, deep vs superficial invasion, early [Stage I] vs late [Stage II−IV] FIGO surgical stage, tumor size, histological grade, and LVSI and LNI statuses), we investigated the clinical utility of serum CA15-3 levels in the selection of low-risk patients with endometrioid type, tumor size <2 cm, myometrial invasion ≤50%, and histological grade 1-2.
The Kolmogorov-Smirnov test was used to assess the normality of the data. Normally, distributed data were expressed as the means±standard deviations (ranges). Non-parametric data were expressed as the medians (interquartile ranges) (ranges). Independent samples t-tests, one-way analysis of variance tests, and post-hoc Tukey tests (when one-way analysis of variance tests were significant) were used to compare the groups. The relationships between serum CA15-3 levels and age, tumor size, and endometrial thickness were determined using the Spearman’s and Pearson’s correlation coefficients. Receiver operating characteristic curves were used to determine cutoff serum CA15-3 levels for selecting low-risk patients. All statistical analyses were conducted using Statistical Package for the Social Sciences for Windows, software version 21.0 (IBM Corp., Armonk, NY, USA). A p<0.05 was considered statistically significant and odds ratios and 95% confidence intervals were determined.
Results
The demographic, clinical, and pathological characteristics of all 96 patients with EC are summarized in Table 1. The mean serum CA15-3 levels were significantly higher in advanced (≥Stage II) tumors compared to early (Stage I) tumors (34.2±35.3 [7.0-153.0] IU/mL vs 19.3±9.8 [4.0-44.0] IU/mL; p=0.001). Moreover, there was a weak linear correlation between serum CA15-3 levels and tumor size (Spearman’s correlation coefficient, p=0.006) (Figure 1). In contrast, there were no associations between serum CA15-3 levels and age (Spearman’s correlation coefficient, p=0.78) or endometrial dual-layer thickness (Pearson’s correlation coefficient, p=0.60).
Demographic, clinical, and surgical characteristics of 96 endometrial carcinoma patients who underwent staging surgery.

Spearman’s correlation between serum cancer antigen (CA15-3) levels and tumor size (p=0.006). Serum CA15-3 levels of >55.0 IU/mL were fixed to 55.0 IU/mL.
The mean serum CA15-3 levels were significantly higher in histological Type 2 tumors compared to histological Type 1 tumors (31.8±37.2 [6.7-153.0] IU/mL vs 19.9±8.6 [4.0–41.0] IU/mL; p=0.01). Thereafter, mean serum CA15-3 levels differed significantly according to histological grade (p=0.007). Post-hoc Tukey analyses revealed that the mean serum CA15-3 levels were significantly higher in Grade 3 tumors (31.7±30.7 [4.0−153.0] IU/mL) compared to Grade 1 (17.9±7.8 [8.0–38.0] IU/mL; p=0.009) or Grade 2 tumors (19.4±8.5 [4.0–41.0] IU/mL; p=0.02). In contrast, no significant differences were observed between Grade 1 and Grade 2 tumors (p=0.90).
The mean serum CA15-3 levels were significantly higher in patients with LVSI or LNI compared to patients without LVSI or LNI (29.0±29.4 [4.0-153.0] IU/mL vs 19.3±8.3 [4.0–41.0] IU/mL [p=0.01] and 36.5±42.9 [10.7-153.0] IU/mL vs 19.9±8.8 [4.0-44.0] IU/mL [p=0.002]).
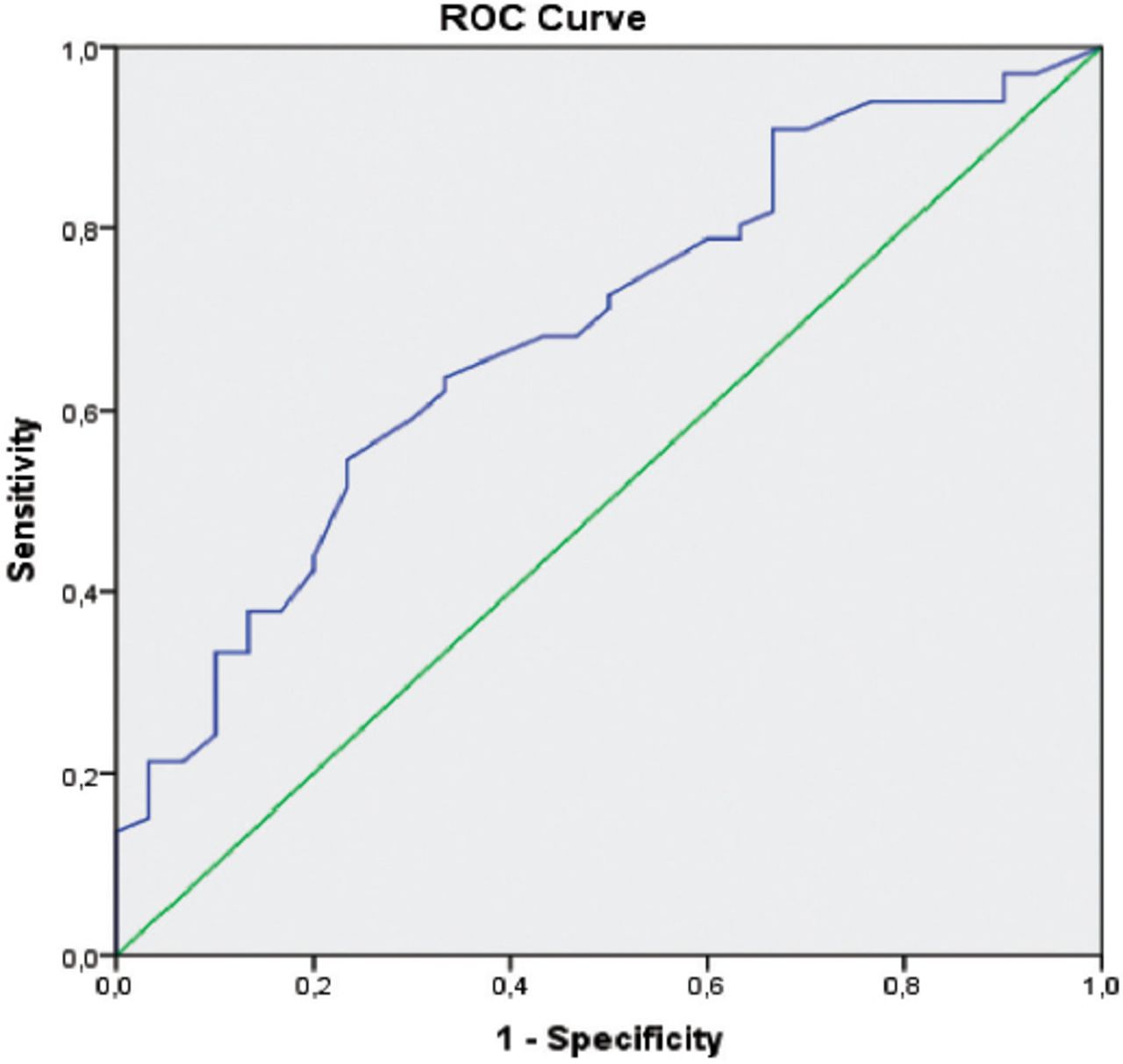
Finally, the mean serum CA15-3 levels were lower in low-risk patients compared to other patients with ECs (16.2±7.1 [4.0-32.0] IU/mL vs 24.4±18.2 [4.0-153.0] IU/mL). This difference was statistically significant (95% confidence interval: 0.57−0.79; p=0.03). Receiver operating characteristic curve analysis revealed that the most suitable cutoff serum CA15-3 level for discriminating between low-risk patients and other patients with ECs was 18.5 IU/mL. The sensitivity was 64% and the specificity was 67% (Figure 2). When the groups (low-risk patients vs other patients with ECs) were assessed in the receiver operating characteristic curve analysis in terms of the 25.0 IU/mL cutoff value, the sensitivity was 33.3% and the specificity was 100%.

Receiver operating characteristic curve of serum cancer antigen 15-3 levels for discriminating low-risk patients (endometrioid type, tumor size <2 cm, myometrial invasion ≤50%, and histological grade 1-2) from other patients with endometrial cancer (area under curve: 0.68; standard error: 0.06).
Discussion
The usefulness of different serum tumor markers has been investigated in EC patients for >20 years. It has been suggested that the application of serum tumor markers with or without the use of different techniques (namely, imaging or pathological procedures) may reflect tumor stage and prognosis in a number of studies.2−5,10,11 However, inconsistent results have been published and there is no consensus on whether serum tumor markers are of diagnostic or prognostic importance in EC. Studies examining serum CA15-3 levels in EC patients2-5,12,15 were also found to be inconsistent.
In several preliminary reports, Soper et al2 and Scambia et al3 had demonstrated that advanced tumor stage and extra-uterine disease risks were increased with elevated serum CA15-3 levels. Moreover, high serum CA15-3 levels were associated with a number of poor prognostic factors (for example, histological grade) and a shorter survival.3,5,12,16,17 However, no consensus has been reached on whether these differences are significant or not.
In contrast to previous reports, we determined preoperative serum CA15-3 levels to be significantly higher in advanced (≥Stage II) EC patients compared to early (Stage I) EC patients (p<0.05).4 However, due to insufficient patient numbers, we were unable to determine whether serum CA15-3 levels differed between advanced FIGO stages. It has been well established that certain factors (for example, older age, advanced tumor grade, type 2 histology, tumor size, and positive LVSI and LNI statuses) are independent prognostic factors for EC.18 However, the relationships between serum CA15-3 levels and these prognostic factors have yet to be fully elucidated. In the present study, we failed to demonstrate an association between serum CA15-3 levels and age. However, we did find that serum CA15-3 levels differed significantly according to tumor size, histological type (Type 2 > Type 1), histological grade (Grade 3 > Grade 1-2), and positive LVSI and LNI statuses. In previous studies, Scambia et al,3 Li et al,5 and Yildiz et al19 reported significant associations between serum CA15-3 levels and FIGO stage, histological grade, and a positive LNI status. However, we demonstrate significant associations between serum CA15-3 levels and tumor size, histological type, and a positive LVSI status.
Low-risk patients (endometrioid type, tumor size <2 cm, myometrial invasion ≤50%, and histological grade 1-2) have a favorable prognosis and it is still debated whether comprehensive surgery is necessary in these patients.20,21 However, the successfulness of investigations that have been performed using different techniques (for example, preoperative imaging studies with or without serum tumor markers and intraoperative frozen section analysis) to discriminate between low- and high-risk patients has varied considerably.10,11,22 Moreover, serum CA15-3 levels have not been evaluated in terms of selecting these patients. In the present study, we demonstrate that serum CA15-3 levels differ significantly between low- and high-risk patients and that 18.5 IU/mL is the most suitable cutoff value for patient selection (sensitivity, 64%; specificity, 67%). Furthermore, a cutoff value of 25.0 IU/mL was able to identify patients in need of comprehensive staging surgery with a specificity of 100%.
In conclusion, although this study has several limitations (for example, its retrospective single-center design and relatively small sample size), we propose that serum CA15-3 levels are a useful diagnostic tumor marker for EC. Comprehensive studies on different histological subtypes are necessary to determine the utility of this tumor marker for patients with ECs.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 31, 2017.
- Accepted August 16, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.