


Abstract
Objectives: To assist the endoscopic localization of the lacrimal sac (LS) relative to nearby landmarks.
Methods: This is a descriptive prospective anatomical study. Sixteen lateral nasal walls were dissected endoscopically to identify and localize the LS between October and November 2015. Multiple measurements were obtained from the NS to the anterior and posterior walls of the LS, as well as to the middle turbinate axilla (MTA) and from the MTA to the LS borders.
Results: The average distance from the NS to the anterior border of the LS was 42.0 mm and the posterior border was 48.5 mm. The average widths of the LS were 7.55 mm superiorly, and 6.6 mm inferiorly representing a mathematical proof that the LS is a trapezoid shape. The mean distance from the NS to the MTA was 47.3 mm. Nine of the 16 lacrimal sacs (56.3%) were found to be partially overlapped by the MTA. The LS was only totally overlapped and lying posterior to the MTA in one side (6.3%), while in 6 sides (37.5%) the LS lay anterior to the MTA.
Conclusion: Endoscopic surgeons should be aware of the location of the LS relative to nearby landmarks, particularly the MTA. Representing a mathematical proof that the LS is wider at it upper part than lower part best presented as a trapezoid shape. We have provided additional measurements that may prove useful in cases of difficult exposure.
Dacryocystorhinostomy (DCR) is the standard treatment for nasolacrimal duct obstruction, and can be performed externally or endoscopically. The endoscopic approach is currently the technique of choice, as it allows improved visualization, avoids an external incision, and does not pose a risk of injury to the medial palpebral ligament or orbicularis oculi, thus, preserving the pumping mechanism of the lacrimal apparatus.1 The most critical step of endoscopic DCR is determination of the location for the mucosal incision and lacrimal osteotomy.2 The size and location of the required bony lacrimal window, as well as the extent of associated soft tissue surgical resections, vary considerably among reports.3,4 In previous reports,5-9 the anterior part of the middle turbinate was resected in 0% to 30% of cases.
Improved endoscopic DCR results can certainly be achieved via a good understanding of the anatomy and topography of the lacrimal sac (LS). One of the main landmarks in the endoscopic approach to the LS is the middle turbinate axilla (MTA). Current anatomical knowledge of this region is, however, inadequate in terms of preparing surgeons for accurate endoscopic localization of the LS in some cases. In fact, only a few cadaveric studies investigating the LS location from an endoscopic perspective have been performed.2,10,11 Notably, the distance from the LS to nearby landmarks may prove useful for the correct localization of the osteotomy site in this context. We have therefore undertaken this descriptive anatomical study, to characterize the anatomy of the LS relative to nearby landmarks. We have also performed several measurements that may be of supplementary assistance for determining an optimal endoscopic approach to the LS.
Methods
Study design
We conducted a descriptive anatomical study of the LS region as a collaborative project between the Otolaryngology-Head & Neck Surgery and Human Anatomy & Histology Departments at Umm Al-Qura University, Makkah. We dissected 16 lateral nasal walls in 8 adult (>18 years old) cadaveric heads between October and November 2015. No heads with evidence of injury to the lateral nasal wall, nasal cavity, or orbit were included. The University Institutional Review Board approved the study protocol prior to commencement of the work.
Dissections and measurements
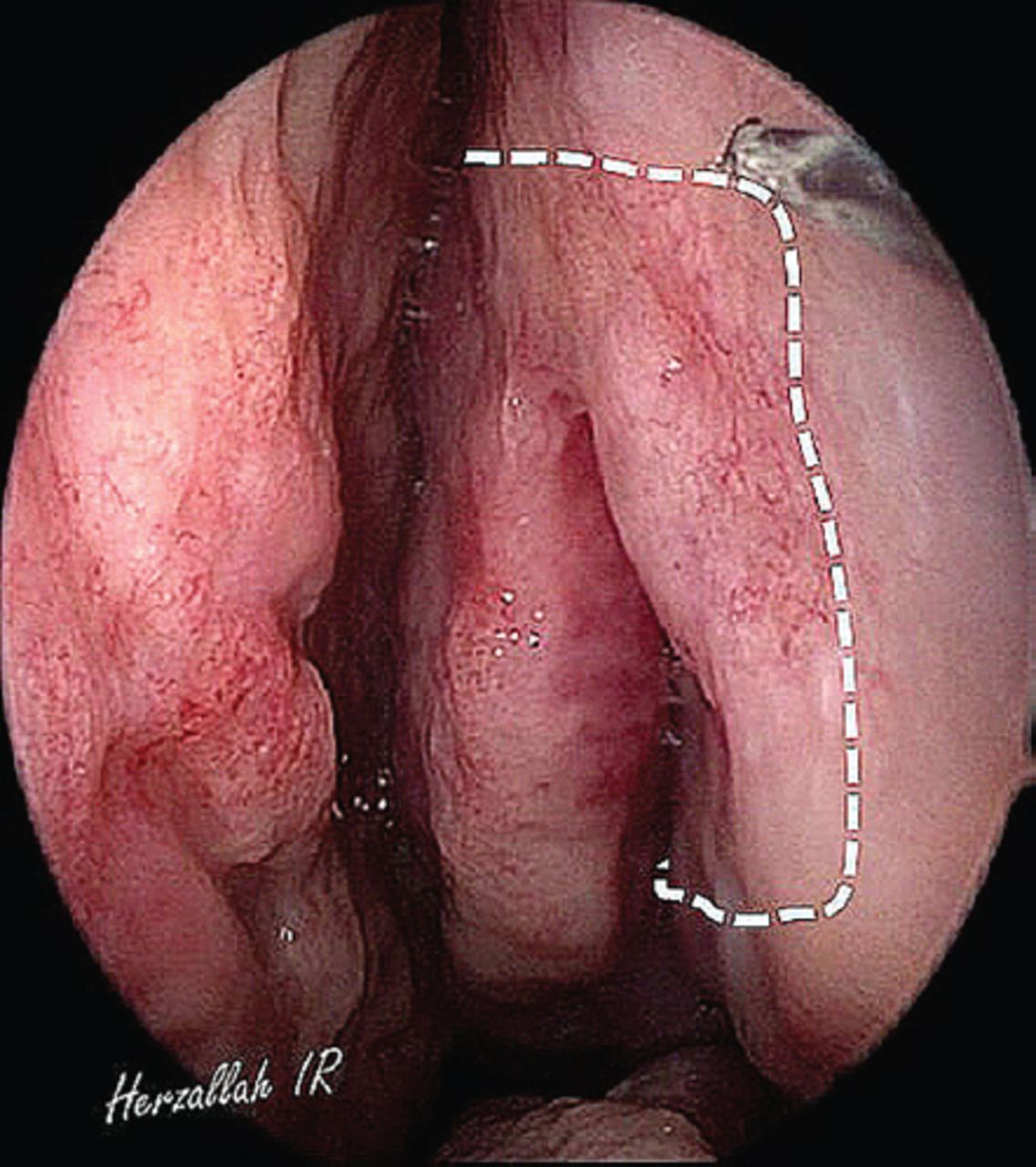
Dissections were performed bilaterally, in accordance with endoscopic surgical steps. A horizontal mucosal incision was made approximately 8 mm above the MTA, and was then continued vertically approximately 10 mm anterior to the MTA. A muco-periosteal flap was then elevated posteriorly, to expose the frontal process of the maxilla and the lacrimal bone (Figure 1). An osteotomy to create a lacrimal bony window was then performed, using a drill and/or Kerrison forceps to expose the LS. The medial wall of the LS was then removed, to ensure proper identification. We described the location of the LS in relation to nearby landmarks by recording the following study variables: 1) distance from the nasal sill (NS) to the anterior and posterior borders of the LS. 2) Width of the LS at the inferior axis, as determined by subtracting the distance between the NS and anterior border of the LS from the distance between the NS and the posterior border of the LS. 3) distance from the NS to the MTA, 4) distances from the MTA to the anterior border of the LS, and to the posterior border of the LS, and 5) width of the LS at the superior axis, as determined by subtracting the distance between the MTA and the anterior border of the LS from the distance between the MTA and the posterior border of the LS (Figure 2).

Lateral nasal wall showing the placement of the muco-periosteal flap to expose the frontal process of the maxilla and the lacrimal bone.

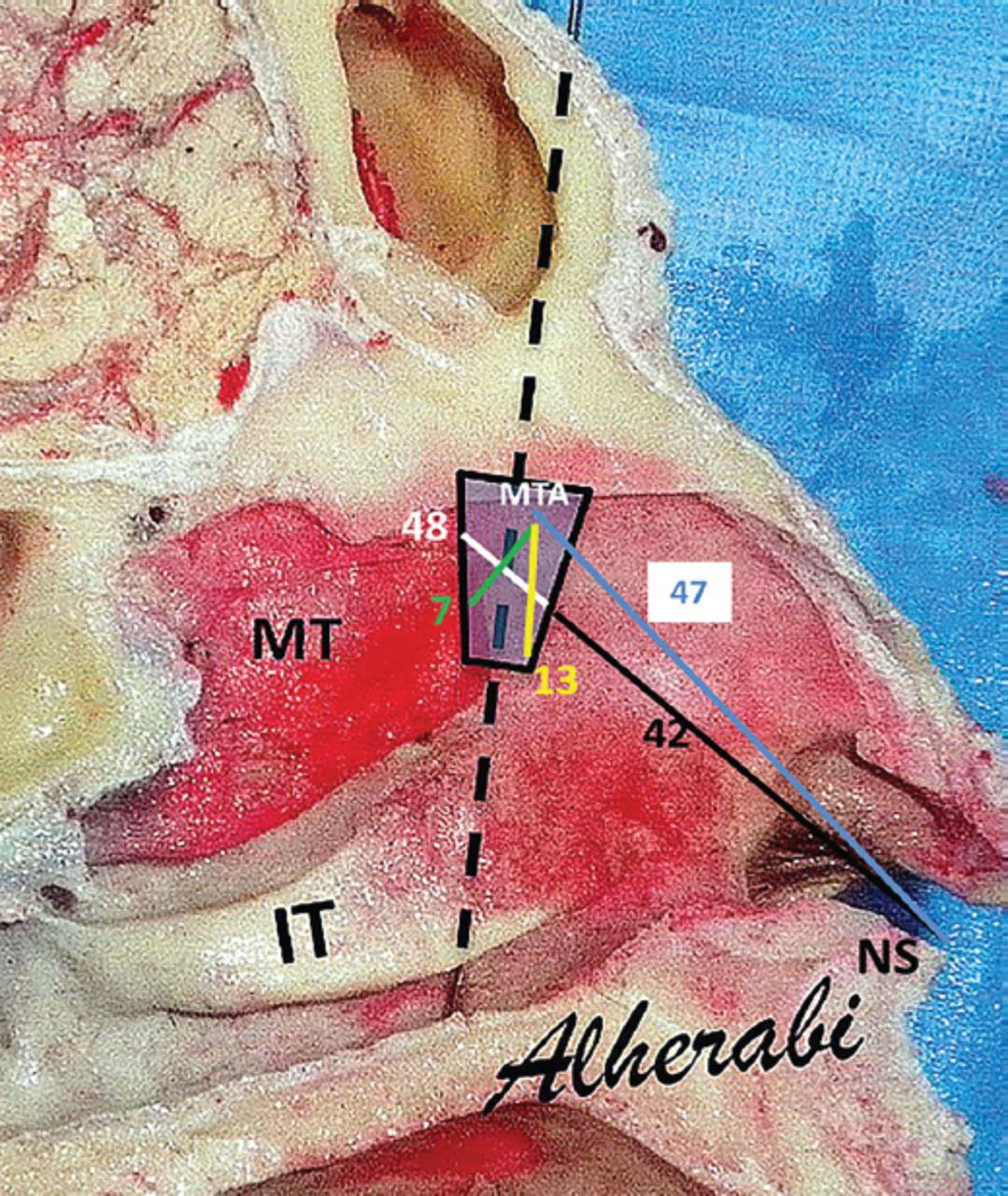
Graphic presentation of all measurements taken of the lateral nasal wall with their averages. Distance from the nasal sill (NS) to the anterior (black) and posterior (white) borders of the LS. Distance from the NS to the MTA (blue). Distances from the MTA to the anterior (yellow) border of the LS, and to the posterior (green) border of the LS. MTA - middle turbinate axilla, IT - inferior turbinate, MT - middle turbinate, NS - nasal sill.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences Version 16 (SPSS Inc., Chicago, IL, USA). Descriptive analyses for all continuous variables were based on mean ± standard deviation (SD), and range. The measurements of the left and right sides were compared using the paired t-test. A p value of <0.05 was considered statistically significant.
Results
All dissected 16 lateral nasal walls in 8 adult (>18 years old) cadaveric heads, 6 males and 2 female’s heads. Both sides were dissected. The mean distance from the NS to the anterior border of the LS was 42.0 mm (± 1.8), and that from the NS to the posterior border was 48.5 mm (± 1.9). The mean width of the LS was 6.6 mm (± 2.2, range 4.0-10.0). The mean distance from the NS to the MTA was 47.3 mm (± 3.1). All measurements are summarized in Tables 1 & 2. Based on the differential distance from the NS to the borders of the LS compared with that from NS to the MTA, 9 of the 16 lacrimal sacs analyzed (56.3%) were found to be partially overlapped by the MTA. The mean width of the LS was 7.55 mm (± 2.4) at the superior axis, and the average width of the LS at the inferior axis was 6.6 mm (± 2.2). Thus, the LS was wider in the upper part than in the lower part mathematically proven to be trapezoid shape (Figure 3). The mean width of the LS that was overlapped by the MTA was 3.0 mm (± 1.6, range 1.0-6.0). The corresponding percentage data were a mean of 42% of the width of the LS overlapped by the MTA, with a range of 20-85%. In 3 of the 16 sides investigated (18.75%), the anterior and posterior borders of the LS lay anterior to the MTA. In another 3 sides (18.75%), the LS lay anterior to the MTA, but the posterior border of the LS lay at the coronal level of the MTA. Only in 1 side (6.3%) was the LS totally overlapped by, and lying posterior to the MTA (posteriorly displaced LS), which is the most difficult type, surgically. The types and corresponding percentages observed are summarized in Table 3, and graphic representations of the different types are shown in Figure 4. No statistically significant differences in any of the measurements (NS to the anterior and posterior borders of the LS, width of the LS, NS to the MTA, or MTA to the anterior and posterior borders of the LS) were evident between the right and left sides (p>0.05 for all comparisons).
Measured distances (mm) to lacrimal sac (LS) borders form nearby landmarks including nasal sill (NS) and middle turbinate axilla (MTA).
Right and left measurements (mm) to lacrimal sac (LS) from nearby landmarks.

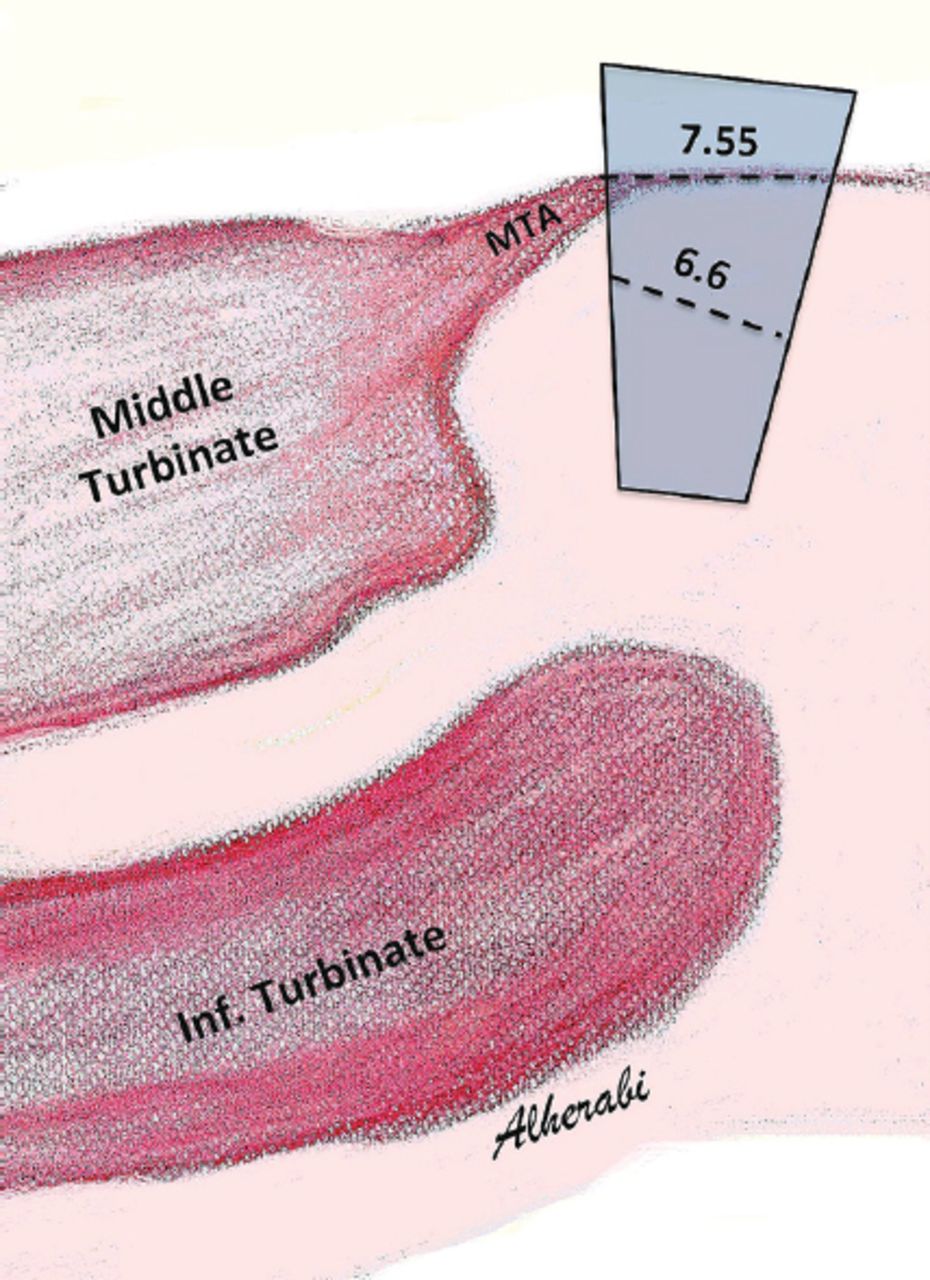
Graphic presentation of the lacrimal sac (LS) model shape. Representing a mathematical proof that the LS is wider at it upper part than lower part mathematically proven to be trapezoid shape. The average width of the LS was 7.55 mm at the superior axis and 6.6 mm at the inferior axis. MTA - middle turbinate axilla.
Summary of Lacrimal sac position types and their related percentage.

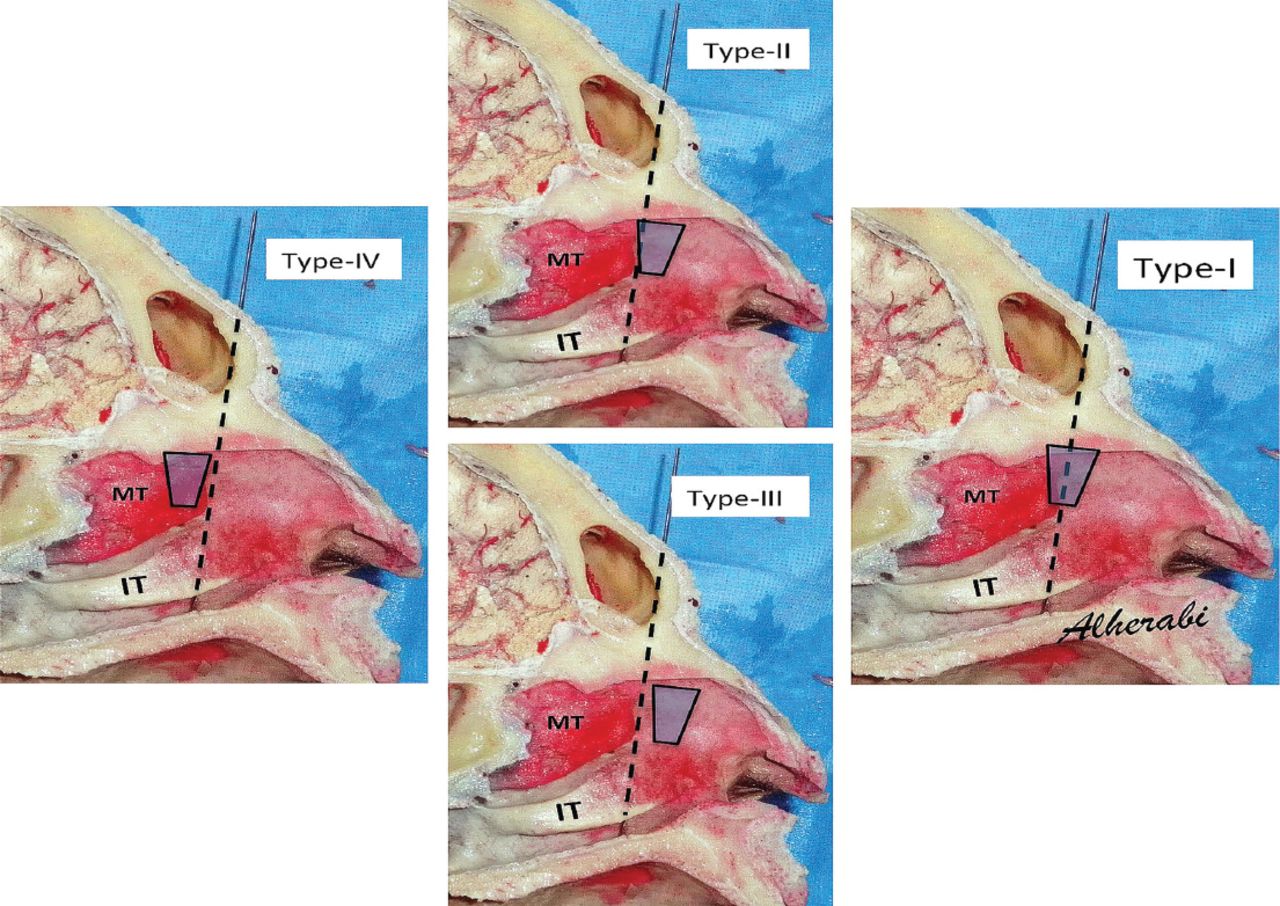
Graphic presentation of the lacrimal sac (LS) types according to position in relation to an axis passes from the eye lower canaliculus and MTA. MTA - middle turbinate axilla, IT - inferior turbinate, MT - middle turbinate.
Discussion
Endoscopic DCR surgery involves removal of the medial wall of the lacrimal fossa after elevation of the muco-periosteum, to create a bony window. It is generally accepted that the anterior half of the LS is covered with the frontal part of the maxilla, and the posterior half is associated with the lacrimal bone.2,12 The success-rate of DCR performed externally or endoscopically is reported to be approximately 80-95%.13-17
Several factors are responsible for the failure of endoscopic DCR. Important factors include the location of the bony ostium and its size, as well as adequate exposure and opening of the LS.18,19 In one study, the size of the ostium and its localization were responsible for 111 of 208 DCR failures.20 To achieve the best result, recent studies suggest the importance of opening the LS ostium as wide as possible. Current literature describes the location of most lacrimal sacs as being anterior to the MTA; it suggests that unless the middle turbinate is hypertrophic or polypoid, the LS commonly lies anterior to the MTA.21,22 However, a CT study by Fayet et al,23 59 patients with complete nasolacrimal stenosis underwent a high resolution (CT) scan before endonasal DCR, that in axial sections the MTA always lies anterior to the lacrimo-maxillary suture, and is never attached to the lacrimal bone. This observation contradicts the traditional premise that the MTA is located posterior to the fossa of the LS. Furthermore, 2 recent cadaver studies have reported that the LS frequently lies partially overlapped by, or posterior to the MTA.2,11
In our dissections, 9 of 16 LSs (56.3%) were found to be partially overlapped by the MTA. Only in 1 of the 16 sides (6.3%) was the LS totally overlapped by, and lying posterior to the MTA. In 6 sides (37.5%), the LS lay anterior to the MTA. Our results are comparable to those reported by Orhan et al,2 who found that the LS is most commonly partially overlapped by the MTA (15 of 20 sides; 75%). However, they reported that 10% of the lacrimal sacs lay totally anterior to, and posterior to the MTA (15%). Both our results and those of Orhan et al2 differ substantially from those reported by Kim et al,11 who found that the most frequent location of the LS in Korean cadavers is lying posterior to, and totally overlapped by the MTA (23 of 36 sides; 63.9%), and in only 27.8% of sides was the LS partially overlapped by the MTA. The reason for these differences is not clear. It may be related to race or gender differences, or it may simply be an artifact arising from the small sample sizes in all these cadaveric studies, including the present study. Another possible factor is the difficulty of accurately delineating the anterior border of the LS. In fact, a difference of just 1 mm can cause the LS to be interpreted as being totally rather than partially overlapped, and vice versa. Characterization of the distances between the LS and nearby landmarks has been proposed as a means to improve the accuracy of localization of the LS. Orhan et al2 reported a mean distance from the anterior nasal spine to the fornix of the LS of 41.20 mm (± 3.96), and a mean distance from the anterior nasal spine to the lower border of the LS of 31.36 mm (± 3.20). These numbers cannot be meaningfully compared to our results, because we measured distances from the NS rather than the anterior spine, the former being easier to identify. Furthermore, we measured distances to the midpoint of the anterior and posterior borders of the LS, because we focused on the anteroposterior extension rather than the vertical extension of the LS, which is now known to be mostly situated above the MTA.2,12 We appreciate that such measurements are not commonly favored by most endoscopic surgeons, and thus they may ultimately serve as secondary guidelines, to be utilized in cases of difficult exposure. In our dissections, the average distance from the NS to the anterior border of the LS was 42.0 mm (± 1.8) while that to the posterior border was 48.5 mm (± 1.9). Lacrimal sac was wider in the upper part than in the lower part mathematically proven to be trapezoid shape rather than oval or rectangular as been represented in the literature.
Study limitations
As our focus was on the localization of the LS, we did not report the relationships between the LS and the uncinate process or the frontal recess in our dissections. A number of previous studies have described the role of uncinectomy in appropriate endoscopic exposure of the LS.5,24,25 We believe that such relationships are important in endoscopic DCR, and should be explored in future studies. Also, a small sample size will necessitate a larger scale study in the future.
In conclusion, the current study provides an update on the endoscopic anatomy of the LS. Endoscopic surgeons should be aware of the location of the LS relative to nearby structures, particularly the MTA. We also advocate the use of the trapezoid shape representation of the LS in the future lacrimal literature. Although many surgeons prefer not to rely on distances during their endoscopic work, we have provided some measurements that may be of assistance in cases of difficult exposure.
Acknowledgment
The authors gratefully acknowledge Mrs. Nesreen Alrehyani for her artistic work of Figure 3.
Footnotes
Disclosure. This study was funded by a Research Grant from the Institute of Scientific Research and Revival of Islamic Heritage, Umm Al-Qura University, Makkah, Saudi Arabia (Grant # 42909012).
- Received August 1, 2016.
- Accepted November 28, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.