


Abstract
Objectives: To retrospectively analyzed the preoperative echocardiographic findings of 9 patients with doubly committed ventricular septal defect (VSD) associated with aortic valve prolapse and to summarize the reasons for misdiagnosis.
Methods: This retrospective study was conducted in Yijishan Hospital, Wannan, Anhui, China between June 2005 and May 2015. Using transthoracic echocardiography (TTE), 92 patients were diagnosed with doubly committed VSD associated with rupture of an aortic sinus aneurysm. The operative findings proved to be in accordance with the echocardiographic findings in 83 patients. Nine patients were confirmed as showing doubly committed VSD associated with perforation of a prolapsed aortic valve. We primarily discussed the 9 patients who were misdiagnosed by TTE.
Results: Aneurysm-like protrusions could be detected by 2-dimensional TTE in the right ventricular outflow tract (RVOT) in 9 patients. All of the aneurysm-like protrusions were confirmed by surgery as over-enlarged right coronary leaflets bulging into the RVOT.
Conclusion: Occasionally, in patients with doubly committed VSD, aortic valve prolapse can be misdiagnosed as an aortic sinus aneurysm. To reduce the misdiagnosis rate and to provide a more precise preoperative diagnosis, multi-section, and multi-angle observation of these diseases should be performed.
Doubly committed ventricular septal defect (VSD) is frequently associated with aortic valve prolapse. Aortic sinus aneurysm can also be associated with doubly committed VSD. Previous studies of these diseases have shown that echocardiography has become a useful noninvasive technique for diagnosing doubly committed VSD associated with aortic valve prolapse without the need for cardiac catheterization.1 However, transthoracic echocardiography (TTE) is associated with a certain misdiagnosis rate,2 and there is very little literature regarding the causes of echocardiographic misdiagnosis. Therefore, we collected 9 patients diagnosed by TTE as having doubly committed VSD associated with a ruptured aortic sinus aneurysm, but later confirmed by surgery as having doubly committed VSD associated with a perforated aortic valve bulging into the RVOT. We retrospectively analyzed the preoperative echocardiographic findings of these 9 patients in hopes of providing more accurate preoperative diagnoses for cardiac surgical operations in the future.
Methods
This retrospective study was conducted in Yijishan, Hospital, Wannan, Anhui, China between June 2005 and May 2015. The inclusion criteria were met by 92 patients (83 cases correct and 9 cases misdiagnosed), there were no special exclusion criteria. Using TTE, 92 patients were diagnosed as having doubly committed VSD associated with aortic sinus aneurysm. Of those patients, surgery confirmed 83 patients as having the same diagnosis as the echocardiographic findings, whereas 9 patients were confirmed as having doubly committed VSD associated with aortic valve prolapse. In this paper, we primarily discussed the 9 patients who were misdiagnosed by TTE. For all patients, TTE was performed using a Philips IE33 echocardiograph. (Philips American investment co., LTD) There were 6 female patients and 3 male patients aged between 3 and 45 years old (mean 16.5 years). Auscultation revealed a continuous murmur along the left sternal border in all patients.
For all patients, TTE was performed using an IE33 echocardiograph, a transducer of 3, 3.75, or 5 was used depending on the patient’s physique and the type of echocardiograph. All the patients were confirmed with operative findings. For the 9 misdiagnosed patients, the TTE images and the operative findings were compared.
Results
In the study period, All 9 patients were diagnosed by TTE with doubly committed VSD, and the intro-operative findings confirmed the diagnoses. Both color and continuous Doppler showed continuous turbulence in the ventricular outflow tract (RVOT) in all the patients, aneurysm-like protrusions were detected by 2-dimensional TTE in the RVOT in all the patients. The operative findings confirmed that there aneurysm-like protrusions were over enlarged right coronary leaflets bulging into the RVOT. Due to infective endocarditis, perforation of the right coronary leaflets was found in 9 patients. Other associated congenital heart diseases included double-chambered right ventricle, secondary atrial septal defect, and patent ductus arteriosus. In all patients, TTE indicated aortic regurgitation to various degrees. Comparison between TTE diagnoses and the operative findings as shown in Table 1.
Comparison between transthoracic echocardiography diagnosis and operative findings
Discussion
Ventricular septal defect is one of the most common congenital heart diseases. There are many subtypes of VSD,3 among which is the doubly committed VSD, is a relatively more common subtype that is seen in Asians than in caucasians.4,5 Unlike other types of VSD, doubly committed VSD is known for a small tendency for spontaneous closure as well as progressive aortic valve prolapse and aortic regurgitation due to the “Venturi pressure effect” of the left-to-right shunt and a lack of anatomical support for the aortic valve.6,7 Open-heart surgery has been advocated as the best treatment for doubly committed VSD. The introduction of echocardiography has made it possible to noninvasively diagnose the location and presence of the VSD and aortic valve deformity.8 Aortic sinus aneurysm is often associated with doubly committed VSD,9 although we observed that the echocardiographic criteria for diagnosis of aortic sinus aneurysm include the following a) the root of the aneurysm is above the aortic annulus, b) the aneurysm is saccular, c) continuous turbulence and high velocities can be detected by continuous-wave Doppler distal to the area of rupture, and d) color flow shows mosaic turbulence across the ruptured aneurysm in real time.10 Using TTE, we occasionally misdiagnose aortic valve prolapse as aortic sinus aneurysm in patients with doubly committed VSD.
In all 9 patients, the size of doubly committed VSD appeared smaller when measured by TTE than in the surgical findings due to the prolapsed coronary leaflets were tethered to the VSD margin, overlying part of the VSD and thus reducing its apparent size.10 In addition, the jet of the VSD was not parallel to the ultrasound beam.11 Ultrasonic physicians should be aware of this phenomenon as it is very common. In all 9 patients, the pronounced distortion and translocation of the aortic annulus resulting from the lack of anatomical support due to the large doubly committed VSD made it difficult to judge the exact location of the root of the aneurysm-like protrusions using the 2–dimensional TTE. Valve excrescences can always form on the surface of the aortic valves as a result of infective endocarditis; they can appear not only as nodular masses (Figure 1), but also as long strips (Figure 2).9,10 These excrescences float around the VSD, covering the aortic annulus, making it more difficult to demarcate the roots of aneurysm-like protrusions. We suggest that the continuity of the coronary leaflet and the root of the aneurysm -like protrusions should be carefully observed when the aneurysm like protrusions are suspected of originating from the prolapsed coronary leaflet. In addition, the coronary leaflet that prolapses into the RVOT through the VSD is always enlarged; thus, its movement is not as stable as that of a normal coronary leaflet in cardiac cycles. Perforation of the aneurysm-like protrusions triggered by extremely thin coronary leaflets and infective endocarditis could be displayed by TTE in all 9 patients, therefore a continuous turbulent flow, which is also a typical feature of ruptured aortic sinus aneurysm could be detected in the RVOT by continuous-wave Doppler.11 In addition, auscultation revealed a continuous harsh murmur along the left sternal border, so ultrasonic physicians tended to diagnose ruptured aortic sinus aneurysm. We should bear in mind that the continuous turbulent flow detected in the RVOT is not unique to ruptured aortic sinus aneurysms.

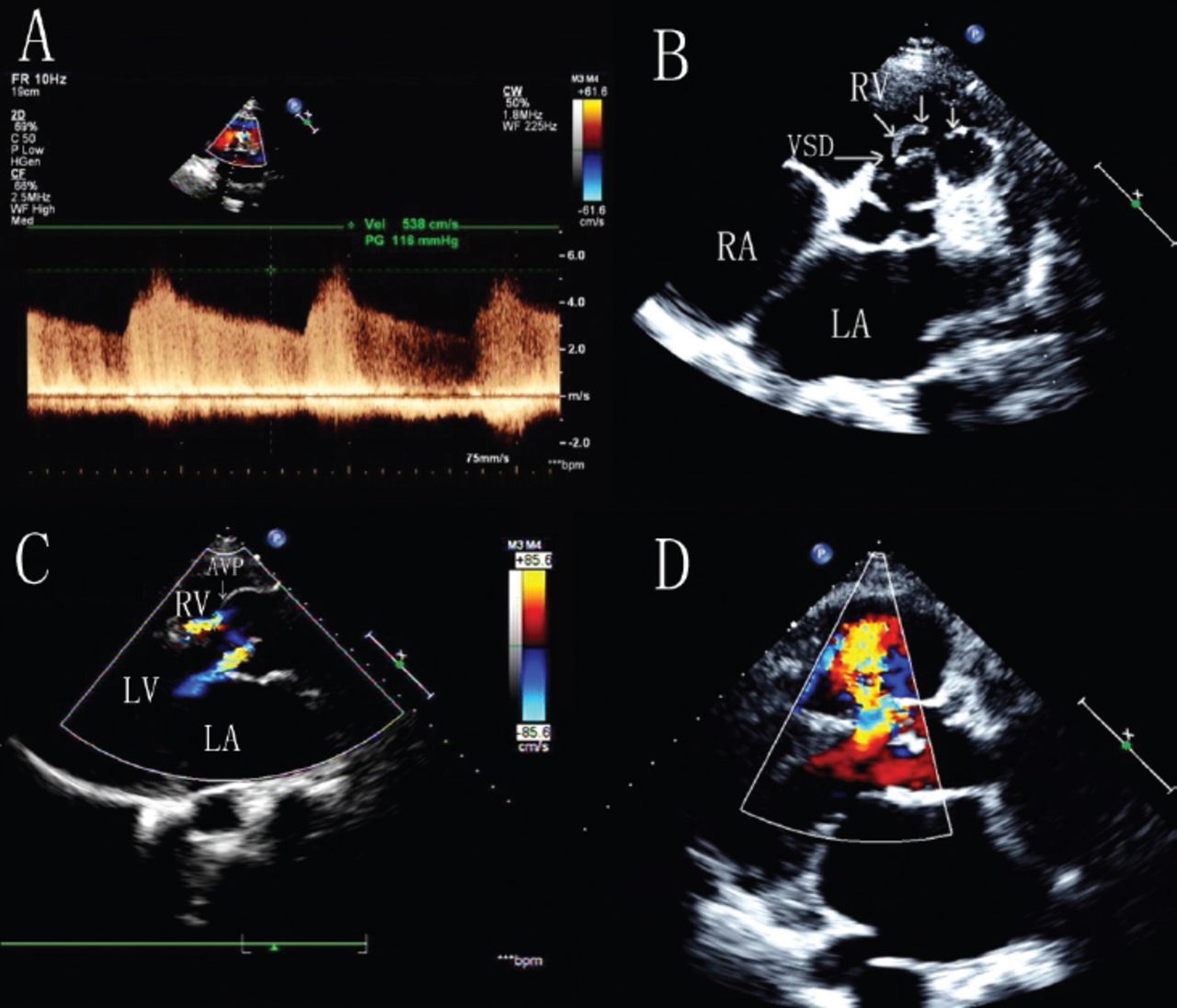
Continuous-wave Doppler showed A) a continuous turbulent flow during both systole and diastole. B) The over enlarged right coronary leaflet appeared to be bulbous and bulging into the right ventricular outflow tract (RVOT), valve excrescence appeared as small masses. C) Color Doppler showed blood flow across large ventricular septal defect during systole. D) RVOT view displayed perforation of the right coronary leaflet

Continuous-wave Doppler showed A) continuous turbulent flow during both systole and diastole. B) The excrescence appeared in the shape of long strips in the right ventricular outflow tract (RVOT). C) The over-enlarged right coronary leaflet appeared to be bulbous and bulging into the RVOT; perforation of right coronary leaflet could also be seen. D) Color Doppler showed blood flow across a large ventricular septal defect during systole.
Apart from the main causes of misdiagnosis mentioned above, other causes of misdiagnosis include the following: a) the irregular shape of VSD, complex structures around VSD and associated abnormalities such as double-chambered right ventricle,12,13 b) Inappropriate gain adjustment of the ultrasound machine, poor imaging on 2-dimensional TTE, and anamorphosis of the color flow signal,14,15 and c) limited experience or lack of skill or understanding of the disease, or limited experience, leading ultrasonic physicians observing a large VSD to fail to scan the exact position of the aneurysm-like protrusion.
The limitation of this study, we haven’t accumulated enough cases, so we need more practice and further research for this kind of disease.
In conclusion, Using TTE, it is sometimes very difficult to obtain an accurate diagnosis of doubly committed VSD associated with aortic valve prolapse. To reduce the misdiagnosis rate and to provide a precise preoperative diagnosis, multi-section, multi-angle observations of the aneurysm-like protrusions should be performed, and the ultrasonic physicians should have thorough knowledge of hemodynamics.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. This article was funded by the First Affiliated Hospital of Wannan Medical College Program, Wuhu, Anhui, China. (Grant No.WK2015ZF and 2016QK019).
- Received October 13, 2016.
- Accepted November 16, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.