


Abstract
Objectives: To assess primary care physicians’ (PCPs) knowledge and attitudes toward sleep disorders.
Methods: In this cross-sectional quantitative study, we surveyed 88 primary care centers under the Ministry of Health during 2015 in Riyadh, Saudi Arabia, using a combination of pre-designed validated questionnaires. Knowledge was assessed using the Assessment of Sleep Knowledge in Medical Education (ASKME) questionnaire, and attitude was assessed using a pre-designed survey. For numerical variables, t-test was used, and for categorical variables, Chi-square test was used.
Results: Data from 223 PCPs (males 50.2%) were analyzed. Among the participants, 44 (19.9%) did not know that sleep medicine is a distinct medical specialty, and 24 (10.9%) felt that sleep disorders are uncommon medical problems based on their daily practice. Only 87 (39%) of physicians stated that they referred patients with sleep disorders to specialized medical centers for further management. The mean score of the ASKME questionnaire was 14.4 ± 4 out of 30 (48%). The majority of physicians (78.5%) obtained a score between 11 and 20. Score results were not related to gender or years of practice.
Conclusion: Primary care physicians’ have a low level of awareness and poor knowledge of sleep medicine and sleep disorders.
Sleep medicine is a relatively new medical field; it was not recognized as an independent specialty in the United States and in Germany until 2006.1 In Saudi Arabia, the first certification exam for sleep medicine as an independent specialty was approved in 2009,1 and sleep medicine was recognized as an independent specialty in 2012.2 Several studies1,2 have documented that sleep disorders are prevalent among all age groups. In Saudi Arabia, an estimated 33% of middle-aged men and 39% of middle-aged women who visited primary care clinics were at risk of developing obstructive sleep apnea (OSA).1 Research has established that sleep disorders, particularly OSA, are associated with different systemic diseases. Moreover, the prevalence of restless legs syndrome (RLS) among patients attending primary care clinics in Saudi Arabia was estimated to be 5.2%.1 Interestingly, in that study, none of the interviewed participants with RLS had been diagnosed or treated for RLS. This result suggests that sleep disorders are under recognized and under treated in the primary care setting. Sleep medicine continues to be insufficiently covered in undergraduate medical school curricula and postgraduate residency training programs.1 In Saudi Arabia, a recent survey of medical schools revealed that the mean time spent teaching sleep medicine was 2.6 ± 2.6 hours.3 Moreover, >95% of the participating medical students scored <60% on the Assessment of Sleep Knowledge in Medical Education (ASKME) questionnaire.3
Primary care physicians (PCPs) are the front-line practitioners in the health care system. The health system in Saudi Arabia relies on the referral system. In this system, the patient’s first contact is typically with a PCP, who assesses the patient and creates the patient’s management plan. The early detection of patients with sleep disorders largely depends on PCPs’ knowledge of sleep medicine. A limited number of studies have assessed PCPs’ knowledge of sleep and sleep disorders in different countries and have generally demonstrated that PCPs have poor knowledge.4-6 Most of those studies were conducted several years ago. For example, an earlier study conducted in Saudi Arabia (1999)6 revealed that only 40% of physicians identified the link between OSA and ischemic heart disease, 43% did not realize that sleep medicine was a distinct specialty and 85% had never attended a lecture on sleep medicine.Since then, the awareness of sleep medicine and sleep disorders has increased, the service has expanded, new sleep disorder centers have been opened, many specialists have joined the field, the Saudi Commission for Health Specialties has recognized sleep medicine as an independent specialty and subspecialty training programs have been established in the country.1,2 Therefore, we designed this study to assess PCPs’ attitudes and knowledge toward sleep and sleep disorders in Saudi Arabia using standardized validated questionnaires and to compare the new findings with the 1999 survey.6
Methods
Health care services in Saudi Arabia are provided by the Ministry of Health (MOH) and other governmental or private health care services. In this study, we targeted PCPs from the MOH, the main health care provider in the country. This cross-sectional study was conducted in all primary care centers under the MOH, Riyadh (the capital), Saudi Arabia, between January and December 2015. According to the database of the General Directorate of Health Affairs in Riyadh, approximately 300 physicians work in 88 primary care centers of the MOH in Riyadh. Inclusion criteria included all PCPs in the MOH. Exclusion criteria included refusal to participate. Primary care centers are distributed across Riyadh and are easily accessible to all residents. Doctors working in primary care centers have different levels of postgraduate education, but all work as PCPs. In general, patients cannot gain access to specialized medical care in the MOH secondary and tertiary care centers unless they are referred by PCPs.
Data collection and questionnaire
In Saudi Arabia, medicine is taught in the English language. Thus, we distributed a self-administered questionnaire written in English to all PCPs. The questionnaire used in this study was composed of 3 sections: 1) Demographics and other variables (age, gender and years of practice). 2) Attitude toward sleep medicine. This section was derived from our previous study and aimed to assess the participant’s education in sleep medicine, attitude toward sleep medicine, and sleep disorders, ability to evaluate possible complications of OSA, and referral of patients with sleep disorders to higher medical centers.6 3) Knowledge assessment. Knowledge of sleep medicine was assessed using the ASKME survey, which is a standardized measure for assessing medical education in sleep.7 The ASKME questionnaire demonstrated a high degree of internal consistency and reliability among the survey items. The score was calculated by adding the correct answers. Participants were divided into 2 groups: those who scored ≥60% (high score group) and those who scored <60% (low score group). We defined a high score as ≥60% because 60% is the pass score in Saudi Arabia.
The study protocol was approved by the Institutional Review Board of King Saud University and the Ethics Committee of the Ministry of Health. The study was conducted in accordance with the Helsinki Declaration. Informed consent was collected from all physicians prior to the inclusion critera. The adaptation of similar studies from the literature was completed using the PubMed.
Data analysis
Data are expressed as the mean ± standard deviation for continuous data. Categorical data are expressed as number and percentage. T-test was used to compare the sleep knowledge scores between groups. If normality test failed, Mann-Whitney U test was used. For categorical data, Chi-square tests were used to compare the sleep knowledge scores between groups. The results were considered statistically significant if p≤0.05. Statistical Package for the Social Sciences, IBM version 22 (SPSS Inc., Chicago, IL, USA), software was used for data analysis and management.
Results
Two hundred and twenty-three PCPs (males: 50.2%) completed the questionnaires, resulting in a response rate of 74.3%. The participants’ mean age was 39.9 ± 9.6 years, and their average “years of practice” was 13.7 ± 9.4 years.
Attitude assessment
One hundred and seventy-seven physicians (80.1%) agreed that sleep medicine is a distinct specialty in the medical field, and 197 (89.1%) agreed that sleep disorders are important medical problems. However, 25.7% did not consider taking a sleep medicine history from patients as an important component of collecting the medical history, and 39.2% considered sleep disturbances to be lifestyle problems rather than medical problems. By contrast, 24 physicians (10.9%) felt that sleep disorders are uncommon medical problems based on their daily practice. Only 75 physicians (33.6%) attended lectures on sleep disorders or received some education about sleep in their postgraduate training and practice. Table 1 presents a comparison of PCPs’ attitude toward sleep medicine between 1999 and 2015 surveys. Most of the assessed parameters showed an improvement in the 2015 surrey compared to the 1999 survey. Eighty-seven (39%) physicians stated that they referred patients with sleep disorders to higher medical centers for further management; however, only 65 (29.7%) realized that sleep disorder centers are located in Riyadh. This discrepancy was due to lack of knowledge of PCPs that there are special units in the hospitals assigned for sleep disorders. The remaining physicians referred their patients to other specialties, including psychiatry and neurology. Physicians who never referred their patients with sleep disorders reported the following reasons: “I do not see patients with sleep disorders” (39.1%); “I can manage patients with sleep disorders” (10.9%); “The head of my center or the referral system does not allow such referrals” (6.5%); “I do not know to whom I should refer my patients” (25.4%); “There are no sleep disorder specialists in the city” (12.3%); and other reasons (5.8%). Table 1 presents a comparison between the current survey and the 1999 survey with regards to the reasons why PCPs did not refer patients with sleep disorders. The percentage of PCPs who did not know to whom they should refer their patients and the percentage of PCPs who thought that no sleep medicine specialists were located in the city significantly decreased.
A comparison of primary care physicians’ attitude toward sleep medicine, reasons why physicians did not refer patients with sleep disorders, and their recognition of the complications of obstructive sleep apnea (OSA) between 2015 and 1999 surveys.
Knowledge assessment
The mean score of the ASKME questionnaire was 14.4 ± 4.0 out of 30 (48%). Further analysis showed that 33 participants (14.8%) received a score of ≤10, 167 (74.9%) a score between 11 and 19 and 23 (10.3%) a score ≥20. Table 2 presents the percentage of correct answers for each question.
The percentage and number of correct answers for each question of the ASKME questionnaire given to primary care physicians.
Subsequently, the respondents were divided into 2 groups: those with high scores (≥60%) and those with low scores (<60%). Forty-five physicians (20.2%) achieved high scores, whereas approximately 79.8% (n=178) were categorized into the low score group. No differences were found between PCPs who had high score in the ASKME and those with low score with regard to the number of years spent on clinical practice (15±7.6 versus 13.3±9.8, p=0.13), and gender (p=0.59). Nevertheless, a significantly higher percentage PCPs who had high score in the ASKME questionnaire received education or attended lectures on sleep disorders during postgraduate training or practice (46.7% versus 30.3%, p=0.04). Additionally, PCPs with high score referred more patients with sleep disorders to the sleep disorder centers (51.1% versus 36%, p=0.06). Only 128 (57.7%) physicians recognized that patients with OSA are at increased risk of hypertension. The percentage of physicians that recognized the other complications and consequences of OSA were as follows: 129 (58.1%) recognized ischemic heart disease, 139 (62.6%) depression, 149 (67.1%) motor vehicle accidents, 63 (28.4%) diabetes mellitus and 111 (50%) pulmonary hypertension. Table 1 presents a comparison of the OSA complications recognized by PCPs in the current survey and those in the 1999 survey.
Discussion
Compared with the results of the 1999 survey with our results show some improvement in PCPs’ awareness of and attitude toward sleep medicine and sleep disorders. Nevertheless, the current survey demonstrates that PCPs still under recognize the importance of sleep disorders and sleep medicine and fail to identify the comorbidities of OSA. Moreover, this study documents that the knowledge of sleep medicine among PCPs in Saudi Arabia is generally low.
Attitude assessment
There was an improvement in PCPs’ attitude toward sleep medicine in this study compared with the 1999 survey. However, PCPs’ level of awareness remained low. Approximately one-quarter of PCPs did not consider taking a sleep history from patients as an important component of the medical history and felt that sleep disorders are uncommon medical problems. Additionally, only 29.7% realized that sleep disorder centers exist in Riyadh. This result mirrors the finding that only 39% of PCPs had referred patients with sleep disorders to higher medical centers for further management.
Older data that assessed PCPs’ attitude toward sleep disorders demonstrated that PCPs did not routinely obtain sleep history during patient interviews.8 One might assume that with an increased number of publications addressing the prevalence and the serious consequences of sleep disorders, PCPs’ awareness of the importance of screening for sleep disorders would improve. Nevertheless, the PCPs’ awareness of sleep disorders remained low. A recent paper evaluated the medical history collected by PCPs in accordance with validated, standardized, patient-report questionnaires on sleep disorders. The study revealed that sleep disorders symptoms are common among patients attending primary care clinics, but are not routinely screened for in the primary care setting.9 Despite the development of sleep medicine service and training in Saudi Arabia, the increased number of sleep medicine specialists and the accreditation of the sleep medicine specialty by the Saudi Commission for Health Specialties, sleep disorders remain under recognized among PCPs.1,2,6 This result is reflected by the finding that approximately one-quarter of the surveyed PCPs did not gather sleep history information and approximately two-thirds did not refer any patients with a sleep disorder diagnosis to higher care medical centers. Two previous studies reported that the interval between symptom onset and referral to a sleep specialist for patients with narcolepsy in Saudi Arabia was 8 years and for OSA was 10 years.1
Knowledge assessment
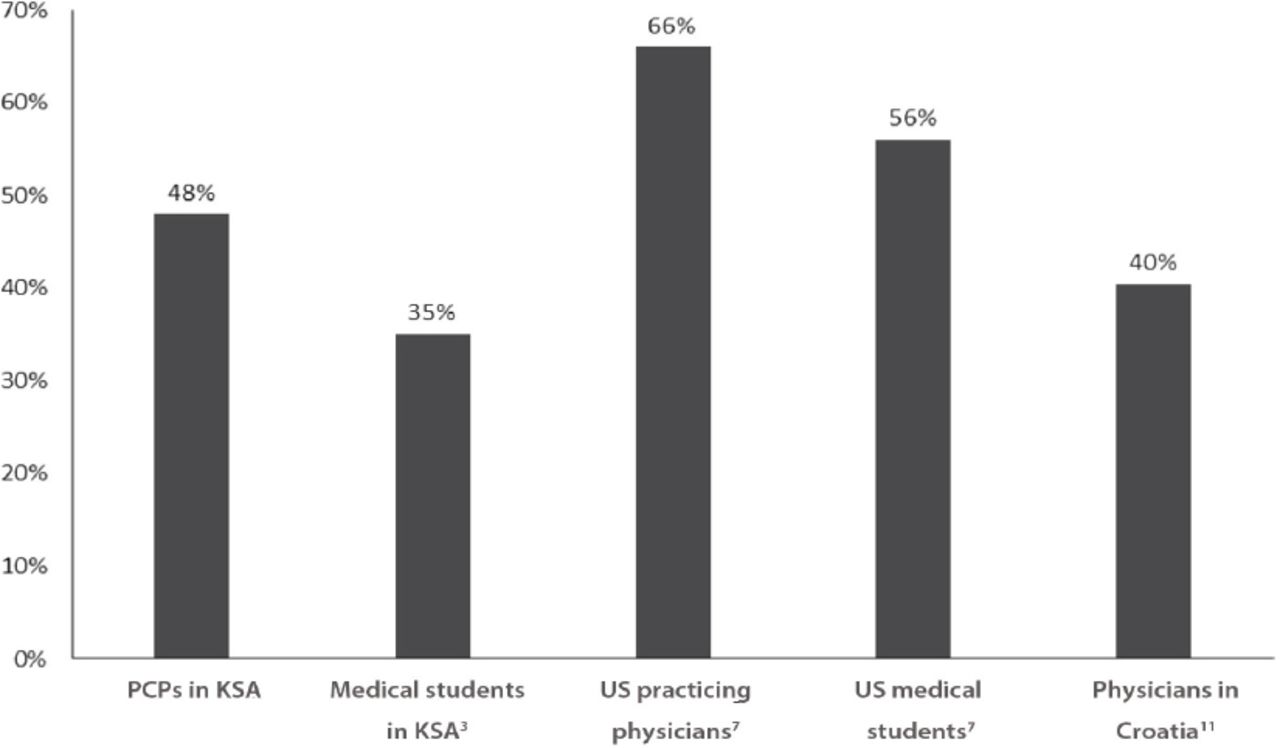
In the present study, only 20.2% of the respondents correctly answered ≥60% of the questions. Figure 1 shows a comparison of the mean ASKME score of PCPs in our study and studies conducted in other countries using the same assessment tool. The mean score of PCPs in our study was lower than the mean score of the United States (US) practicing physicians, nurses and medical students; however, it was higher than the score of practicing physicians in Croatia.7,10 In a US study, the investigators reviewed symptom checklists from patient charts. If the database search revealed a positive sleep diagnosis, the patient’s chart was further queried to determine the clinical assessment and outcome in a primary care community-based setting. The study showed a low rate of recognition of the health impact and diagnosis of sleep disorders in primary care settings.11 Another study revealed that PCPs rated their knowledge of sleep medicine as fair or poor.12
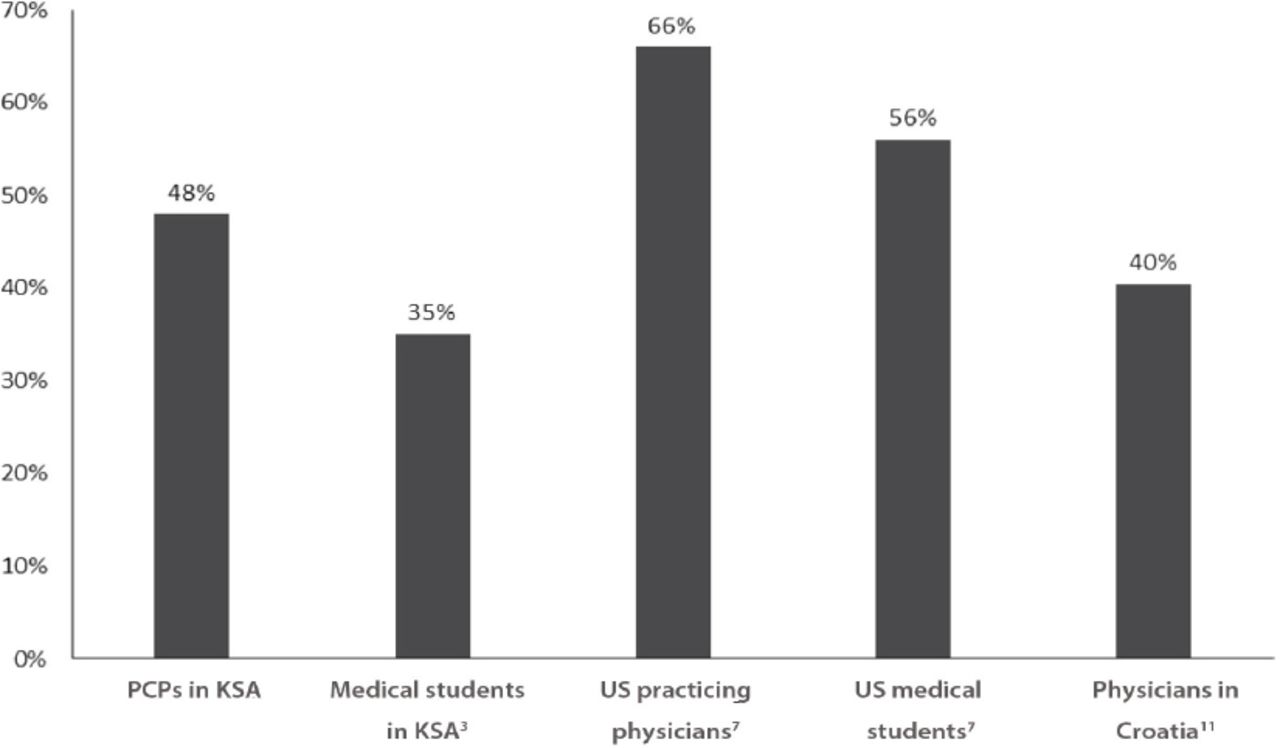
A comparison of the mean Assessment of Sleep Knowledge in Medical Education (ASKME) score of primary care physicians’ (PCPs) in our study and that of PCPs in studies in other countries using the same assessment tool.
In this study, when participants were divided into high score and low score groups, the years of practice did not significantly differ between the 2 groups. In a recent study conducted with PCPs in a few South American countries, the investigators assessed total OSA knowledge using the OSA Knowledge and Attitude (OSAKA) questionnaire and reported no differences among PCPs with varying years of practice.4 However, another study reported a negative correlation between years of practice and OSA knowledge using the OSAKA questionnaire.13 This discrepancy may reflect the lack of sleep medicine education in medical schools in Saudi Arabia. Hence, even younger physicians have limited knowledge on sleep medicine. This assumption was supported by the results of a new study that assessed medical students’ knowledge of sleep medicine and the time that major medical schools spent teaching sleep medicine.3 The mean number of hours spent teaching sleep medicine was 2.6, and there was no difference in the ASKME score of students with a high GPA and those with an average GPA, indicating that sleep medicine was not taught in medical schools.3 Moreover, sleep medicine education is not a part of the family medicine residency training curricula.1 There was a trend toward more referrals among PCPs who were in the high score group, reflecting the importance of good knowledge in detecting and referring cases of sleep disorders.
A study conducted by Reuveni et al14 demonstrated the lack of PCPs’ awareness of the importance of screening for OSA. However, most previous study9 have not explored the obstacles related to not referring patients with sleep disorders in primary care settings. In our study, when PCPs were asked regarding these obstacles, 39.1% stated that they did not see patients with sleep disorders, although previous study1 in Saudi Arabia have revealed that sleep disorders are common among patients attending primary care clinics; and 25% stated that they did not know to whom they should refer patients with sleep disorders. This result reflects the lack of PCPs’ awareness of the importance of recognizing and referring patients with sleep disorders.
Moreover, the findings indicated PCPs’ poor knowledge of sleep disorders, as one-quarter of PCPs included in this study did not consider taking a sleep medicine history from patients as an important component of the medical history. Nonetheless, PCPs might not screen for sleep disorders because they have limited time allocated to assess patients in the busy outpatient setting.15 In the current study, 25.4% of PCPs did not know to whom they should refer patients with sleep disorders. This issue can be improved by publicizing sleep medicine as a specialty and designing educational programs on sleep medicine for PCPs that include information on when and where to refer patients with sleep disorders.16 Moreover, PCPs should realize the importance of ensuring that patients with sleep disorders receive early referrals to sleep medicine specialists for proper diagnosis and treatment and improved outcome. The Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine17 recommended a multidisciplinary approach to the management of OSA that includes primary care. Nevertheless, with the limited number of sleep medicine specialists in Saudi Arabia, as well as in other countries, it is impractical to expect that the currently available sleep medicine service will be able to be the primary caregivers to care for all patients with sleep disorders. Therefore, sleep medicine specialists, PCPs and other related specialists must cooperate.1 Sleep medicine specialists need to inform primary care and family medicine residency programs of the importance of both theoretical and practical training in sleep medicine such that trainees can diagnose, treat and refer patients to sleep specialists, if needed. Sleep education for PCPs can make a difference.18 An intensive educational weekend course on sleep disorders developed by 2 physicians resulted in an 8-fold increase in referral rate from 0.27% before education to 2.1% after education.18 Moreover, rates of compliance with continuous positive airway pressure (CPAP) therapy among patients managed by their PCPs were comparable to those of patients managed by sleep medicine specialists.18 The detection and referral of patients with sleep disorders could also be improved by using a reliable and sensitive screening questionnaire for sleep disorders prior to the physician’s assessment; such a questionnaire would also reduce the time needed to assess symptoms.19
Study limitation
Bias may result from the fact that survey respondents may attempt to overstate their performance; thus, their lack of knowledge could be under reported in this study. Nevertheless, this study provides important information on PCPs’ knowledge of and attitude toward sleep disorders and stresses the need to improve PCPs’ awareness and knowledge of sleep medicine.
In conclusion, PCPs in Saudi Arabia have poor knowledge of sleep medicine and under recognize the importance and impact of sleep disorders, which may reflect the weak level of education and training in this field of medicine. Educating PCPs on sleep disorders will allow the early detection of sleep disorders; thus, the provision of proper treatment and the prevention of complications.
Acknowledgment
We would like to thank Mr. Abdullah Al-Sulimani and Ms. Sultanah Borai for their participation in data collection.
- Received November 20, 2016.
- Accepted January 25, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}