


Abstract
Objectives: To determine the validity of uric acid as a potential prognostic marker for long-term outcomes of patients with acute myocardial infarction (AMI) and those with AMI undergoing percutaneous coronary intervention (PCI).
Methods: Systematic review and meta-analysis were performed. We retrieved data from retrospective and prospective cohort studies that investigated whether serum uric acid (SUA) level affects the prognosis of patients with AMI.
Results: Thirteen studies involving 9371 patients were included. High serum uric acid (HSUA) level increased mid/long-term mortality (risk ratio (RR)=2.32, 95% confidence intervals (CI): 2.00–2.70) and had higher short-term mortality (RR=3.09, 95% CI: 2.58–3.71), higher mid/long-term major adverse cardiovascular events (MACE) risk (RR=1.70, 95% CI: 1.54–1.88), and higher short-term MACE risk (RR=2.47, 95% CI: 2.08–2.92) for patients with AMI. In the PCI subgroup, the HSUA level also increased mid/long-term mortality (RR=2.33, 95% CI: 1.89 to 2.87) and had higher mid/long-term MACE risk (RR=1.64, 95% CI: 1.48–1.82), and higher short-term MACE risk (RR 2.43, 95% CI: 2.02–2.93) for patients who were treated with PCI after AMI. Particularly in the PCI subgroup, a higher short-term mortality (RR=6.70, 95% CI: 3.14–14.31) was presented in the group with lower HSUA cut-off level, and the mortality was higher than the group with higher HSUA cut-off level (RR=2.69, 95% CI: 2.09–3.46).
Conclusion: The HSUA level significantly increased the mortality and MACE risk of patients with AMI. Mild elevation of SUA levels (normal range) have started to have a significant impact on the short-term mortality of patients who underwent PCI, and has not received the attention of previous studies. However, this condition should be further investigated.
With the developments in antithrombotic and reperfusion therapies over the past several years, the mortality of acute myocardial infarction (AMI) has been steadily decreasing. However, coronary artery disease (CAD) is still the leading cause of death worldwide.1 Uric acid is an end metabolite of purine.2 Hyperuricemia is often accompanied by metabolic syndrome, such as hypertension, diabetes, dyslipidemia, and obesity, which are all known risk factors of coronary heart disease (CHD).3 Cardiovascular health may suffer from the adverse effects caused by elevated serum uric acid (SUA) levels. The odds ratio (OR) for CHD was 2.59 for patients with UA levels >9 mg/dL.4 The risk for many diseases was increased with an increased SUA level although the SUA level <7.0 mg/dL.5 Many studies and two meta-analyses indicated an independent association between hyperuricemia and major adverse cardiovascular events (MACE) and mortality.6,7 Although many researches were conducted on the link between hyperuricemia and cardiovascular disease, their causal relationship remains controversial;8 Two meta-analyses have found that high serum uric acid (HSUA) level could significantly increase the mortality and risk of MACE in patients with AMI.9,10 One of these 2 meta-analyses only analyzed in-hospital mortality. Hence, the effect of HSUA on the long-term prognosis of patients with AMI and those undergoing percutaneous coronary intervention (PCI) subsequently is not well known. To determine the validity of uric acid as a potential prognostic marker for long-term outcomes of patients with AMI and those undergoing PCI, we systematically reviewed published reports on uric acid and AMI to assess the prognostic value of SUA as a risk factor for increased mortality and MACE.
Methods
Literature search
We retrieved cohort studies (prospective and retrospective) regarding whether SUA level affected the prognosis of patients with AMI from the following databases: Embase, PubMed, Cochrane Library (up to May 17, 2016). Our search strategies included the following search terms, (“uric acid” OR “uricemia” OR hyperuricemia) AND (“myocardial infarction” OR “acute coronary syndrome” OR “MI” OR “ACS”) AND (“mortality” OR “major adverse cardiovascular events” OR “MACE”) (Just search human studies. Language was restrained as English). We referred to the Meta-analysis of Observational Studies in Epidemiology11 as a reference when making the search strategy. In addition, we manually retrieved literatures to ensure identification of all published trials.
Study eligibility
Studies will be adopted if they fulfilled the criteria for inclusion as follows: (1) original, cohort studies of adult patients; (2) exposure factor, including hyperuricemia or HSUA level; (3) outcomes, including in-hospital mortality or short-term mortality (<30 days) or mid/long-term mortality (>6 months) or MACE; (4) sample size at least 100 cases; (5) score/star of study based on the Newcastle–Ottawa Scale (NOS)12 more than 7. Three major elements in NOS were used to evaluate the cohort study: selection (0–4 stars), comparability (0–2 stars), and outcome (0–3 stars). The full star was nine. In addition, we excluded studies without specific detailed data. We selected the study with the longest follow-up time (FUT) if data were reported repeatedly over time.
Study selection
Two authors based on the study eligibility independently selected the studies. The first author performed the primary screening through the titles and abstracts. We obtained the full text if we cannot rule out this research through its title and abstracts. After the primary screening, the texts were independently screened by 2 reviewers. Any disparities were resolved through discussion and arbitration by a third reviewer.
Data extraction
Two researchers independently extracted data from each study. A third reviewer was included for arbitration purposes. We contacted the authors of the study that had incomplete or unclear data. The data extracted included the sample size, number of exposure or non-exposure group, gender, age, HSUA cut-off level, and whether a successful treatment option was provided, such as PCI, outcome, FUT, variable controlled, number of mortality or MACE, and the data needed in NOS.
Statistical analysis
The data accumulated were used to calculate the risk ratio (RR) and 95% confidence intervals (CI) of HSUA as a risk to affect the incidence rate of MACE and mortality (significance level, p<0.05). The random effects model (D+L) was used while considering the differences in the evaluated settings. We illustrated relevant baseline characteristics in the studies and used the chi-square test based on Cochran’s Q test and I2 statistics (significance level, p<0.1) to assess the heterogeneity of the studies.13 The heterogeneity level was quantified by using the I2.14 Based on the severity of the heterogeneity, I2<25%, 25≤I2<50%, and I2≥50% are generally considered as no heterogeneity, mild heterogeneity, and indicative of large heterogeneity, respectively.14,15 The publication bias (significance level p<0.1) was assessed by using the Begg funnel plots.16,17 We performed a subgroup analysis on whether all the patients in the study cohort were treated with PCI. All the data were analyzed by using Stata 12.0 (Stata Corp, College Station, TX, USA).
Results
Literature search
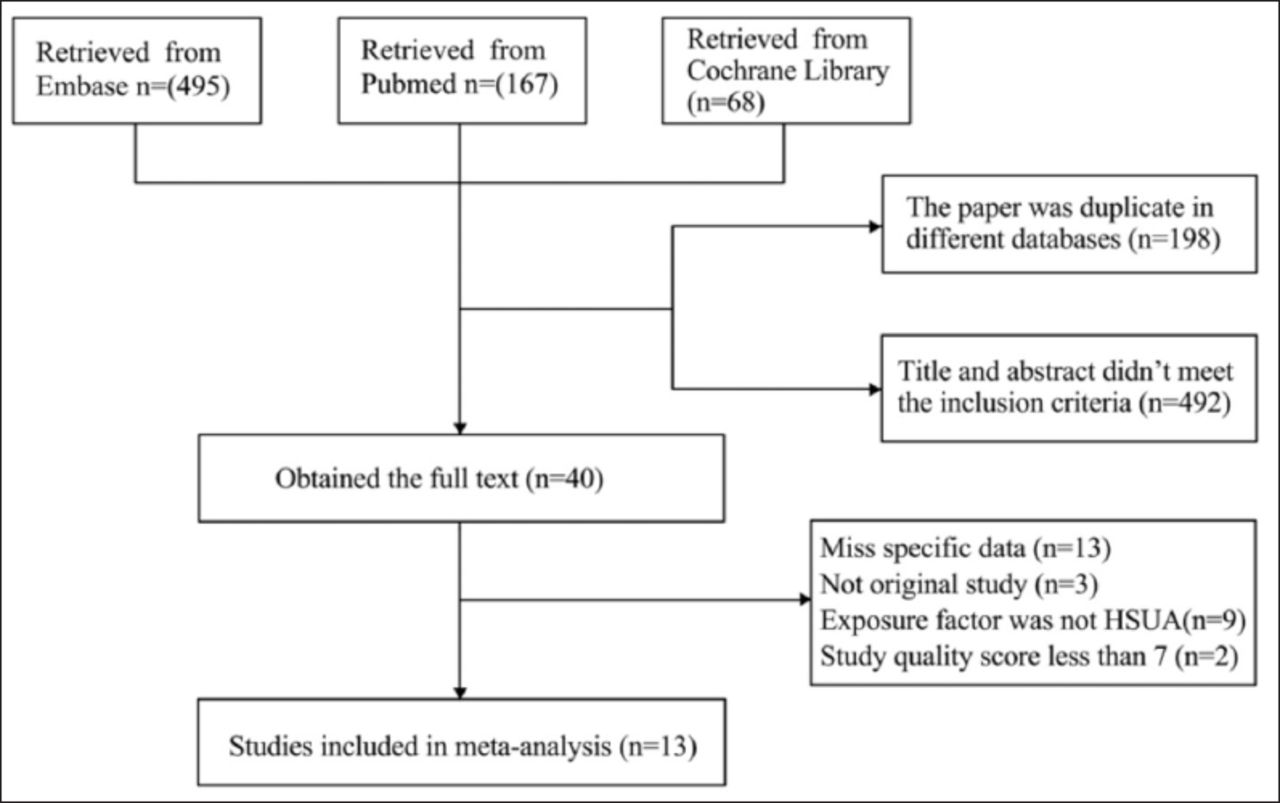
The electronic searches identified 730 records, wherein 13 studies18-30 met the inclusion criteria. Figure 1 describes the specific selection process of literature. If the same paper exists in multiple databases, we retained the paper of one database; thus, 198 papers were excluded. We excluded 492 papers because the title and abstract did not meet the inclusion criteria. We obtained the full text of 40 studies, wherein 13 were excluded because specific data were not included (for example, HSUA cut-off level, FUT, number of deaths). Three papers were not an original study. Nine studies were excluded because the exposure factor was not SUA or hyperuricemia. Two studies were excluded because NOS score was <7.

Flow chart summarizing the procedure of studies selection for the meta-analysis. HSUA - high serum uric acid
Description of studies
This analysis included 13 studies with 9371 patients. The inclusion criteria of 8 studies18-20,23,24,26-28 were patients who were diagnosed with acute ST-elevation myocardial infarction (STEMI) and underwent PCI subsequently. The inclusion criteria of 2 studies21,22 were patients with STEMI, but did not control their treatment plan. Another three studies25,29,30 did not control whether these patients underwent PCI and included patients with STEMI and non-STEMI (NSTEMI) in the cohort. The FUT of seven studies,19,23,25,26,28-30 was >6 months and <30 days for the others.18,20-22,24,27 All these studies had clear HSUA cut-off level. Two studies’19,24 particularly had a cut-off lower (5.4 mg/dL and 5.7 mg/dL) than other studies. Six studies19,23,26,28-30 reported mid/long-term mortality, and 5 studies19,23,25,26,28 reported mid/long-term MACE. Twelve studies18-24,26-30 reported short-term mortality, and 6 studies19,23,24,26,28,30 reported short-term MACE. The characteristics of these studies are shown in Table 1.
Characteristics of included studies in the meta-analysis that investigated whether serum uric acid (SUA) level affects the prognosis of patients with AMI.
Mid/long-term (≥6 months) mortality
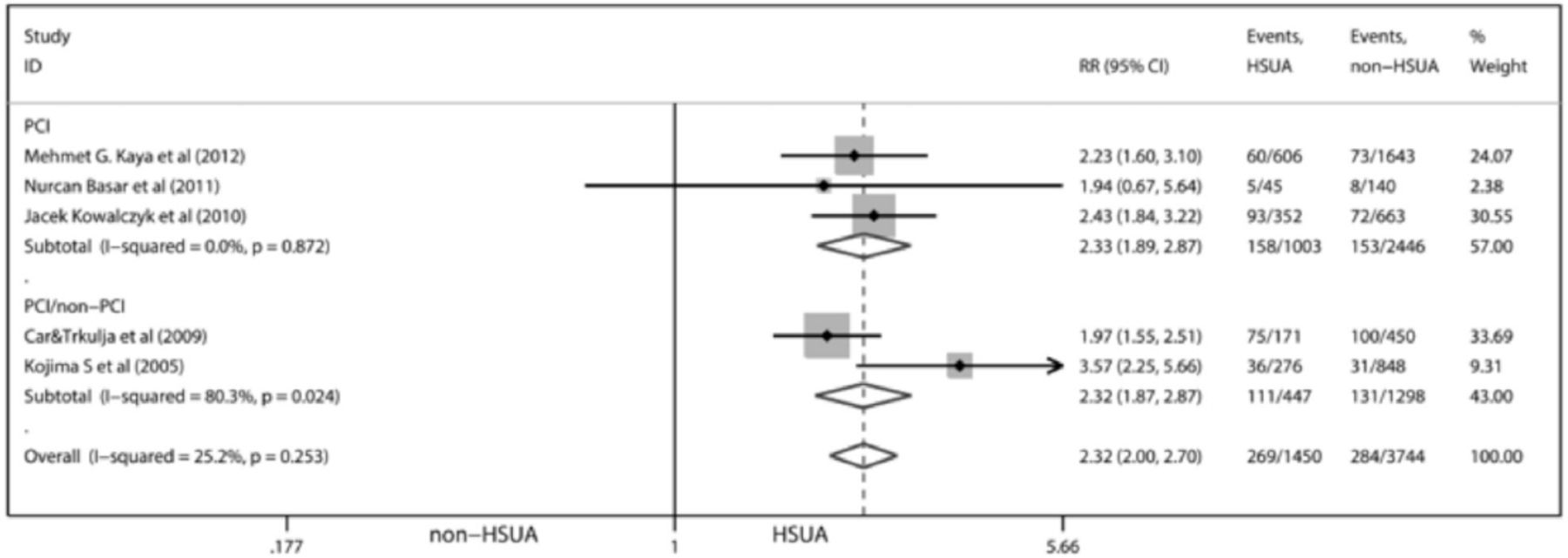
Six studies (5628 participants) reported mid/long-term mortality, wherein 2 studies29,30 included patients with STEMI and NSTEMI in the cohort, and did not control whether these patients underwent PCI; 4 studies19,23,26,28 included only patients with STEMI who underwent PCI. HSUA was associated with higher mid/long-term mortality (RR=2.43, 95% CI: 2.10–2.82). A study heterogeneity was observed (I2=50.4%, p=0.073). After excluding the study19 with significantly lower HSUA cut-off level than other studies, the effect was not much changed (RR=2.32, 95% CI: 2.00–2.70). Nonetheless, the heterogeneity was found to be significantly decreased (I2=25.2%, p=0.253) (Figure 2), and no publication bias was observed by the Begg test (z=0.24, p=0.806). In the subgroup analysis on whether patients underwent PCI, the effect (RR=2.33, 95% CI: 1.89–2.87) had almost no difference in the group that mixed patients who underwent PCI and those who did not (RR=2.32, 95% CI: 1.87–2.87), and no heterogeneity (I2=0.0%, p=0.872) was found among these studies that only included patients who underwent PCI (Figure 2). Therefore, the heterogeneity among studies may be due to the fact that some studies have not controlled whether patients underwent PCI or not, as well as differences in the critical value of HSUA in various studies.

Forest plot for random effects analysis of risks of AMI mid/long-term morbidity associated with HSUA. AMI - acute myocardial infarction, PCI - percutaneous coronary intervention, HSUA - high werum acid, RR - relative risk, CI - confidence interval
Short-term (≤30 days) mortality
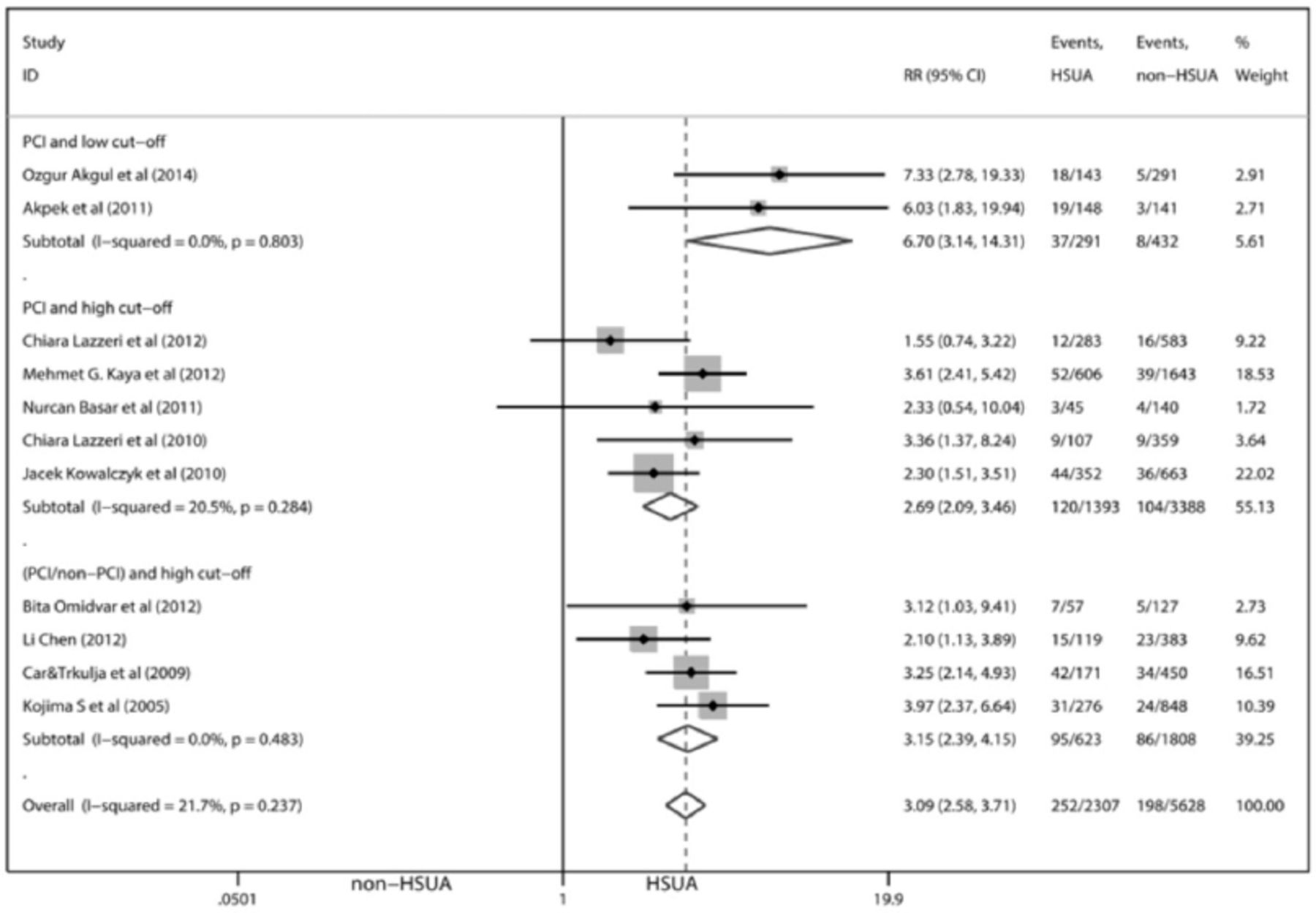
Twelve studies (8521 participants) reported short-term mortality, wherein 2 studies29,30 included patients with STEMI and NSTEMI in the cohort and did not control whether these patients underwent PCI; eight studies18-20,23-28 included only patients with STEMI who underwent PCI. Two studies21,22 included only patients with STEMI, but did not control whether these patients underwent PCI. The HSUA was associated with higher short-term mortality (RR=3.19, 95% CI: 2.68–3.79). Mild heterogeneity (I2=26.0%, p=0.189) and no publication bias by the Begg test (z=0.07, p=0.945) were observed. After excluding the study18 with the shortest FUT, the effect was not much changed (RR=3.09, 95% CI: 2.58–3.71). However, among-study heterogeneity (I2=21.7%, p=0.237) (Figure 3) was significantly decreased, and no publication bias by the Begg test (z=0.00, p=1.00) was found. In the subgroup analysis on whether the patients underwent PCI and HSUA cut-off level, the HSUA was associated with higher short-term mortality (RR=2.69, 95% CI: 2.09–3.46) (Figure 3) in the PCI and high cut-off subgroups, higher short-term mortality (RR=6.70, 95% CI: 3.14–14.31) (Figure 3) in the PCI and low cut-off subgroups. The heterogeneity among studies was likely attributable to the short FUT.

Forest plot for random effects analysis of risks of AMI short-term morbidity associated with HSUA. AMI - acute myocardial infarction, PCI - percutaneous coronary intervention, HSUA - high werum acid, RR - relative risk, CI - confidence interval
Mid/long-term (≥6 months) MACE
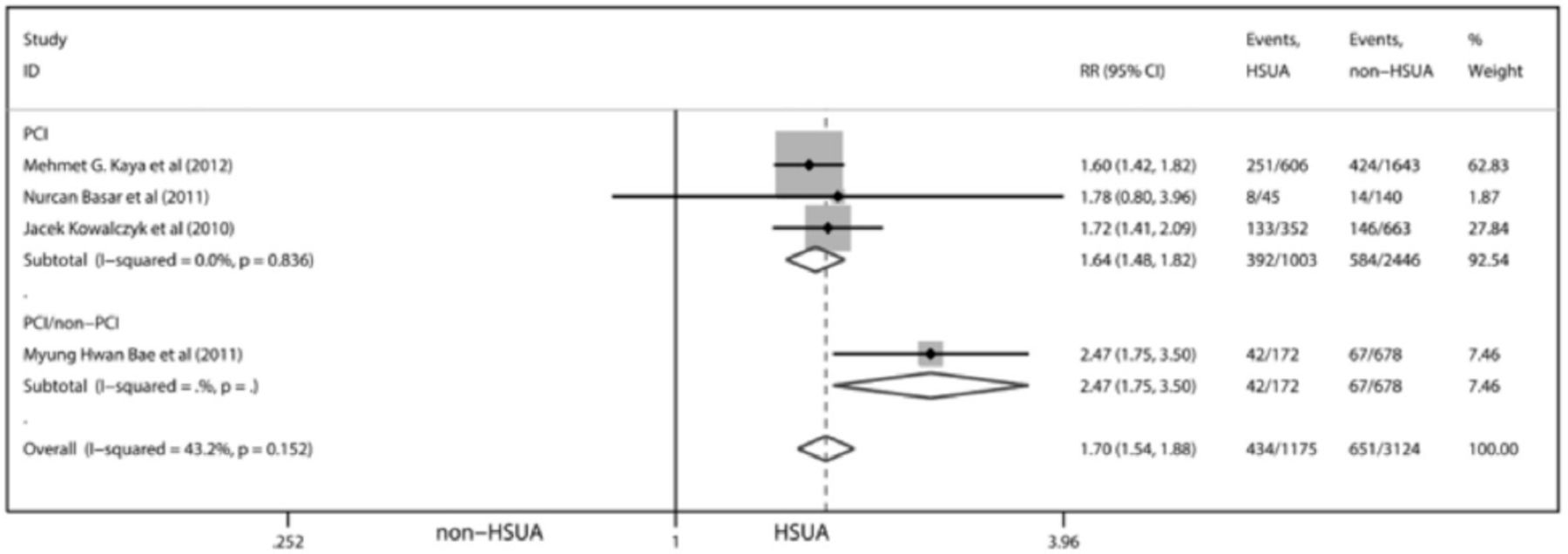
Five studies (4733 participants) reported mid/long-term MACE, wherein one study25 included patients with STEMI and NSTEMI in the cohort and did not control whether these patients underwent PCI; 4 studies19,23,26,28 included only patients with STEMI who underwent PCI. HSUA was associated with higher mid/long-term MACE (RR=1.74, 95% CI: 1.58–1.92) with mild heterogeneity (I2=48.9%, p=0.098) and no publication bias by the Begg test (z=0.73, p=0.462). After excluding the study19 with significantly lower HSUA cut-off level than that in other studies, the effect was not much changed (RR=1.70, 95% CI: 1.54–1.88). The study heterogeneity (I2=43.2%, p=0.152) (Figure 4) decreased, and no publication bias by the Begg test (z=0.34, p=0.734) was observed. In a subgroup analysis of studies that included only patients who underwent PCI, the mid/long-term MACE RR was not much changed (RR=1.64, 95% CI: 1.48–1.82), but the among-study heterogeneity (I2=0%, p=0.836) decreased significantly (Figure 4). The heterogeneity among studies was mainly attributable to the AMI type and whether patients underwent PCI.

Forest plot for random effects analysis of risks of AMI mid/long-term MACE risk associated with HSUA. AMI - acute myocardial infarction, PCI - percutaneous coronary intervention, HSUA - high werum acid, RR - relative risk, CI - confidence interval
Short-term (≤30 days) MACE
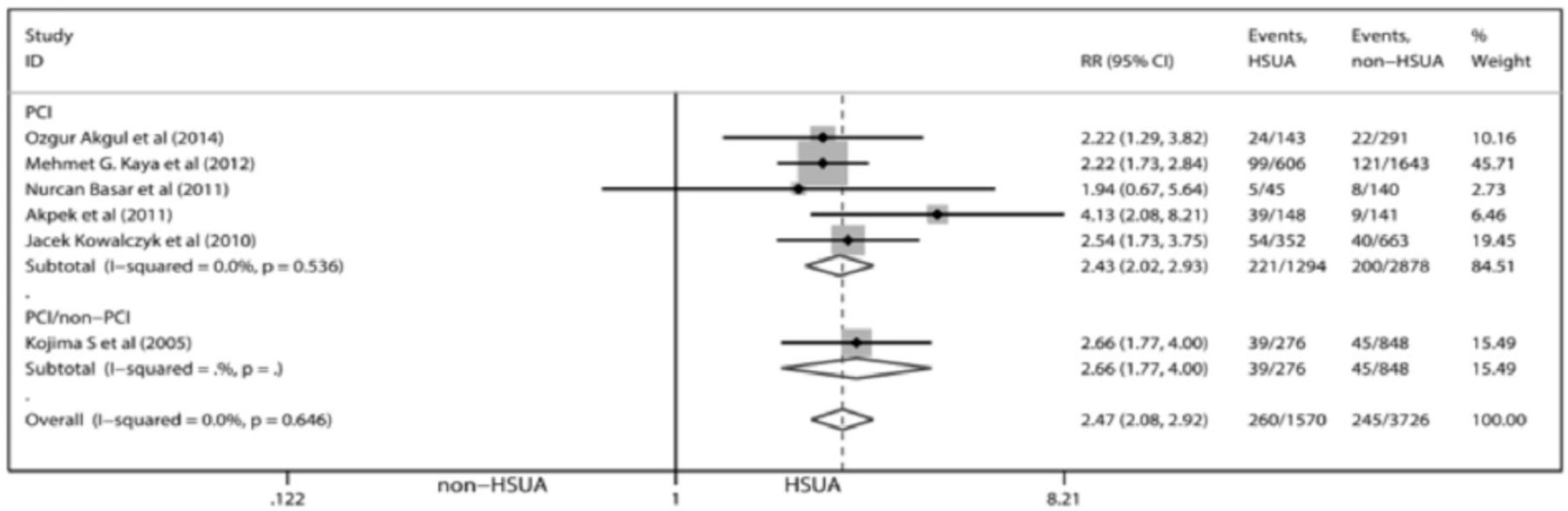
Six studies (5296 participants) reported short-term MACE, wherein one study30 included patients with STEMI and NSTEMI in the cohort and did not control whether these patients underwent PCI; 5 studies19,23,24,26,28 included only patients with STEMI who underwent PCI. HSUA was associated with higher short-term MACE (RR=2.47, 95% CI: 2.08–2.92), no heterogeneity (I2=0.00%, p=0.646) (Figure 5), and no publication bias by the Begg test (z=0.38, p=0.707). In the PCI subgroup, the short-term MACE risk (RR=2.43, 95% CI: 2.02–2.93) was not different with the PCI/non-PCI subgroup (Figure 5).

Forest plot for random effects analysis of risks of AMI short-term MACE risk associated with HSUA. AMI - acute myocardial infarction, PCI - percutaneous coronary intervention, HSUA - high werum acid, RR - relative risk, CI - confidence interval
Discussion
The main finding of this systematic review and meta-analysis showed that HSUA level (including hyperuricemia and high-normal values) significantly increased short-term mortality (<30 days), mid/long-term mortality (>6 months), short-term MACE, and mid/long-term MACE of patients after AMI. Furthermore, a clear subgroup analysis was performed by different HSUA cut-off levels, different treatments (whether these patients underwent PCI), different AMI types, etc. The association is still statistically significant. With respect to short-term mortality, the HSUA cut-off level in two studies was significantly lower than that in other studies, and the RR of overall effect of the two studies were significantly higher than that of other study patients. This might indicate that the mild increase in SUA level (normal range) begun to significantly affect the short-term prognosis of patients who underwent PCI after STEMI, and this conclusion has not been raised before.
Uric acid is a xanthine metabolite and plays a role as an antioxidant. During tissue ischemia, xanthine oxidoreductase might catalyze xanthine to uric acid, and uric acid appeared as compensatory increase.31-36 Recent studies have established that uric acid was associated with cardiovascular disease. Patients with AMI with high SUA levels were found to more likely die than those with lower SUA levels.37,38 Therefore, high uric acid levels might be a risk factor for MACE and mortality even in younger patients (<35 years) with AMI.39-41 Angiotensin receptor blocker and statins were well known to be useful for patients with metabolic syndrome. Metabolic syndrome was identified as a multiple risk factor (high blood pressure, visceral obesity, dyslipidemia, and dysglycemia) for cardiovascular disease.42-44 Some reviews suggested that hyperuricemia (with or without urate deposition) can be considered as a component of the metabolic syndrome.44,45 Recent studies confirm that uric acid weakened the role of losartan, atorvastatin, and fenofibrate to reduce cardiovascular risk.46-48 Furthermore, allopurinol can reduce the casual and 24-h ambulatory blood pressure of adolescent patients with newly diagnosed hypertension compared with placebo in a random trial.49,50 A study including 245 consecutive patients with stable angina pectoris showed that a significant increase in SUA level may cause platelet resistance for patients with CHD.51 However, some studies showed that the SUA level did not influence the response of platelet to ticagrelor, clopidogrel, and aspirin,52 and SUA level did not increase platelet aggregation during dual antiplatelet therapy whether aspirin was combined with tigriolor or combined with clopidogrel.53 Nevertheless, it needed a large random clinical trial and long-term follow up to determine the safety and efficacy of lowering UA therapy in cardiovascular disease.
This meta-analysis has several limitations. First, most studies were retrospective. Although these studies considered a multitude of lifestyle, diet, and comorbidities, many unmeasured and residual confounding factors in studies difficult to rule out must be acknowledged. Second, the design of each study cannot be perfectly consistent. Some differences were found among these studies with respect to age range, FUT, AMI type, and so on. Hence, the inherent limitation to this meta-analysis is the potential heterogeneity among these studies. Third, the differences in various factors in PCI surgery might increase heterogeneity among studies of the PCI subgroup. Finally, the HSUA cut-off level was different in each study, with some as high as 7.5 mg/dL and some as low as 5.4 mg/dL, but the HSUA cut-off level in most of these studies (10/13) was between 6 mg/dL and 7 mg/dL. We have done our best to evaluate the comprehensive effect by removing the study with significantly lower or higher HSUA cut-off levels than those in other studies.
This study also has some strengths. The sample size of these studies included in this meta-analysis was relatively large. Assessment of the quality of each study for a systematic review is necessary. However, there was no unified view regarding which method is the best to evaluate the quality of studies. We chose the NOS12 to evaluate these studies, and the NOS includes three important elements on evaluating cohort studies. The quality of the studies included in this meta-analysis was higher. We performed subgroup analysis on whether patients underwent PCI after AMI and calculated the RRs for mortality and MACE of patients who underwent PCI after AMI (STEMI). We found that the short-term mortality was significantly increased by the mildly elevated SUA levels in patients who underwent PCI after AMI, and the short-term mortality was worse than the group with higher HSUA cut-off levels.
In conclusion, this meta-analysis evidenced that HSUA level increased the mortality and risk of MACE whether short-term or mid/long-term and whether PCI was performed after AMI. Particularly, the mild elevation of SUA levels (normal range) might have begun to have a significant increase in the short-term mortality of patients with STEMI and those who underwent PCI. However, this should be conferred with further investigations and research, and this reminded us that the relative value of elevated uric acid level after PCI may be more worthy of our attention than the absolute value of uric acid.
References
*References should be primary source and numbered in the order in which they appear in the text. At the end of the article the full list of references should follow the Vancouver style.
*Unpublished data and personal communications should be cited only in the text, not as a formal reference.
*The author is responsible for the accuracy and completeness of references and for their correct textual citation.
*When a citation is referred to in the text by name, the accompanying reference must be from the original source.
*Upon acceptance of a paper all authors must be able to provide the full paper for each reference cited upon request at any time up to publication.
*Only 1-2 up to date references should be used for each particular point in the text.
Sample references are available from: http://www.nlm.nih.gov/bsd/uniform_requirements.html
Footnotes
Disclosure. The authors declare that there is no conflict of interest regarding the publication of this article, and the work was not supported or funded by any drug company. This project is funded by the Natural Science Foundation of Tianjin, China (Grant number: 16JCZDJC31900) and International Student’s Science & Technology Innovation Project (Scientific Research Project number: 2110/2GJ006) of Tianjin Medical University, China.
- Received November 8, 2016.
- Accepted March 8, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}