


Abstract
Objectives: To assess the compliance with the 2006 American College of Critical Care-Pediatric Advanced Life Support (ACCM-PALS) guidelines for sepsis management, and the 2012 surviving sepsis campaign (SSC), for the management of pediatric patients with sepsis and to identify the main barriers to adherence to these guidelines.
Methods: In November 2015, a prospective cohort study in which a web based electronic survey using a case scenario to explore the usual management of a child with severe sepsis was designed and sent to all consultant pediatric intensivists practicing in Kingdom of Saudi Arabia (KSA). Adherences to 2012 SSC guidelines and to 4 algorithmic time-specific goals outlined in the ACCM-PALS guidelines were measured.
Results: Sixty-one (76%) of 80 consultant pediatric intensivists working in KSA responded to the survey. Of the 61 respondents, 94% reported administering antibiotics within one hour of the child presentation, 98% reported starting resuscitation by giving fluid boluses, 93% reported starting vasopressor if the patient remained hypotensive despite fluid resuscitation, and 86% reported they would start hydrocortisone in case of catecholamine refractory shock. In total, 80% of the intensivists reported full adherence to all of the 4 components in the ACCM-PALS bundle; 50% reported that the absence of a locally written protocol was the main barrier to adherence to the SSC guidelines.
Conclusion: Pediatric intensivists reported good adherence to the 2006 ACCM-PALS guidelines and 2012 SSC guidelines with some variability in interpretation of the recommendations. The absence of a written protocol was the main reported barrier to adherence to these guidelines.
Sepsis is a leading cause of mortality among pediatric patients admitted in the pediatric intensive care units (PICU) worldwide. The hospital mortality rate due to septic shock in the pediatric population in developed countries is 8.9%,1 while that in developing countries ranges from 24% to 58%.2,3 The international sepsis forum (ISF) was launched in 1997; the ISF and number of collaborators developed guidelines for the management of severe sepsis and septic shock.4 These guidelines were used by the surviving sepsis campaign (SSC) as the starting point for a guideline revision that led to the sepsis bundles and global database. The ISF was a founding partner of the SSC along with the Society of Critical Care Medicine and the European Society of Intensive Care Medicine. The SSC announced its ‘Barcelona Declaration’ in 2002, which was subsequently followed by various iterations of the “Surviving Sepsis Guidelines”, lastly updated in 2012.5 These recommendations include a section on specific pediatric considerations, providing recommendations that are intended to guide clinical practice. These guidelines recommendations are in line with the American College of Critical Care Medicine-Pediatric Advanced Life Support (ACCM-PALS) guidelines for the management of septic shock in pediatric patients.6 Although several studies have shown that compliance with these sepsis guidelines were associated with better outcomes in patients with severe sepsis and septic shock,7,8 adherence to these guidelines is not consistent among pediatric health care providers.9-11 The aim of this study was to describe the initial management of pediatric patients with severe sepsis, to assess the compliance of this management with the 2006 ACCM-PALS guidelines for sepsis management, and the 2012 SSC guidelines, and to identify barriers to adherence to these guidelines in the Kingdom Saudi Arabia (KSA).
Methods
Study design
This was a prospective cohort study using a de-identified, web based electronic survey (Survey Monkey) regarding the management of pediatric patients with severe sepsis and septic shock; the survey was sent via electronic mail to physicians. The study was approved by the investigational review board at King Fahad Medical City, Riyadh, KSA. Since the study presented, no more than minimal risk of harm to subjects and involved no procedures for which written consent is normally required outside of the research context, the principle of implied consent was used. This study was conducted in line with the Strengthening the Reporting of Observational Studies in Epidemiology for Respondent-Driven Sampling Studies (STROBE-RDS) Guidelines.12 Participants were asked to describe the management of hypothetical patient, as described in the survey, as they would do in practice in their intensive care unit (ICU). Questions regarding investigations, fluid and catecholamine management, intubation, and specific treatments (antibiotics, steroids, transfusions, and insulin) were included. Participants were also asked to identify the main barriers to the application of the SSC guidelines in their center.
Development of the written questionnaire
The questionnaire was a modified version adapted with permission from the survey carried out by Santchi et al,9 it was translated into English, and adjusted to the updated 2012 SSC guidelines. Participants were asked to describe the usual management of a hypothetical patient in the ICU. The provided case scenario was a 2-year-old boy, otherwise healthy, brought to the emergency room by his parents with shock presentation after 2 days of viral illness. On examination, his heart rate was 185 beats/min, the blood pressure was 67/35 mm Hg, the respiratory rate was 40 cycles/min, he had a temperature of 39.8°C. He was lethargic, responding only to painful stimuli, with moderate retractions. Peripheral perfusion was impaired with mottled skin; peripheral pulses were weak, and the capillary refill time was 5 seconds. Participants were asked to respond to specific questions addressing the investigations that they would undertake for this patient, their typical fluid, and catecholamine management, intubation timing, and medications used, as well as steroid, transfusion, and insulin indications.
Study population
All consultant pediatric intensivists practicing in KSA were considered eligible to participate in the study. They were identified from the Saudi critical society database, Riyadh, KSA We choose to send the survey to all pediatric intensivists and not only PICU directors in order to decrease population selection bias. On November 1, 2015, the survey was sent out via e-mail to 80 eligible participants. To improve the participant response rate and in order to increase the study size a reminder was sent via -email every month, until the closure of the study on October 31, 2015.
Statistical analysis
Categorical data were expressed as frequencies (%), whereas continuous data were expressed as medians and interquartile ranges (IQR). Compliance with guidelines was determined for the 4 main components of the ACCM-PALS guidelines for the management of the septic shock algorithm: fluid boluses, antibiotics, inotrope for fluid refractory shock, and hydrocortisone for catecholamine resistant shock. Data sets were analyzed for the current study were available from the corresponding author upon request.
Results
Respondent demographics
Of the 80 eligible consultant pediatric intensivists working in Saudi Arabia, 61(76%) responded to the questionnaire. Saudi nationals comprised 77% (n= 47) of intensivists, with 23% (n=14) from other nationalities. Approximately 60% had been working for less than 10 years as consultant pediatric intensivists: 30% for <5years, 32% for 5-10 years, and 38% for >10 years. Thirty-four intensivists (55%) were working in the medical and surgical non-cardiac PICU, 12 (20%) in a cardiac PICU, 12 (20%) in a general and cardiac PICU, and 3 (5%) in a purely medical PICU. The institutions for which the intensivists were working were academic for 75% of those enrolled. The median number of beds in the PICUs was 15, (IQR 5-34). Sixty percent of the respondents had been working in a PICU with an admission rate of 500 to 1000 per year, 33 (33%) in a PICU with an admission rate less than 500 per year and 7 (7%) in a PICU with an admission rate of more than1000 per year.
ACCCM-PALS algorithm for the management of septic shock
Almost all respondent (93.5%) reported administering antibiotics within one hour of the child’s presentation, 98% reported starting initial resuscitation by giving fluid boluses of 20 mL/kg crystalloids or colloids, 93% reported starting vasopressor if the patient remained hypotensive despite aggressive fluid resuscitation and 86% reported that they would start hydrocortisone in case of catecholamine refractory shock. Forty-nine (80%) intensivists reported full adherence with all of the 4 components in the ACCM-PALS bundle.
Hemodynamic support
Crystalloids were the first choice of fluid resuscitation among most pediatric intensivists (88%). Colloids were the first choice in 12%, 25% considered colloids if there were no improvements with the second bolus of crystalloids, 15% reported never using colloids for fluid resuscitation in septic patients, and 48% of the respondent used colloids if there was concomitant hypoalbuminemia.
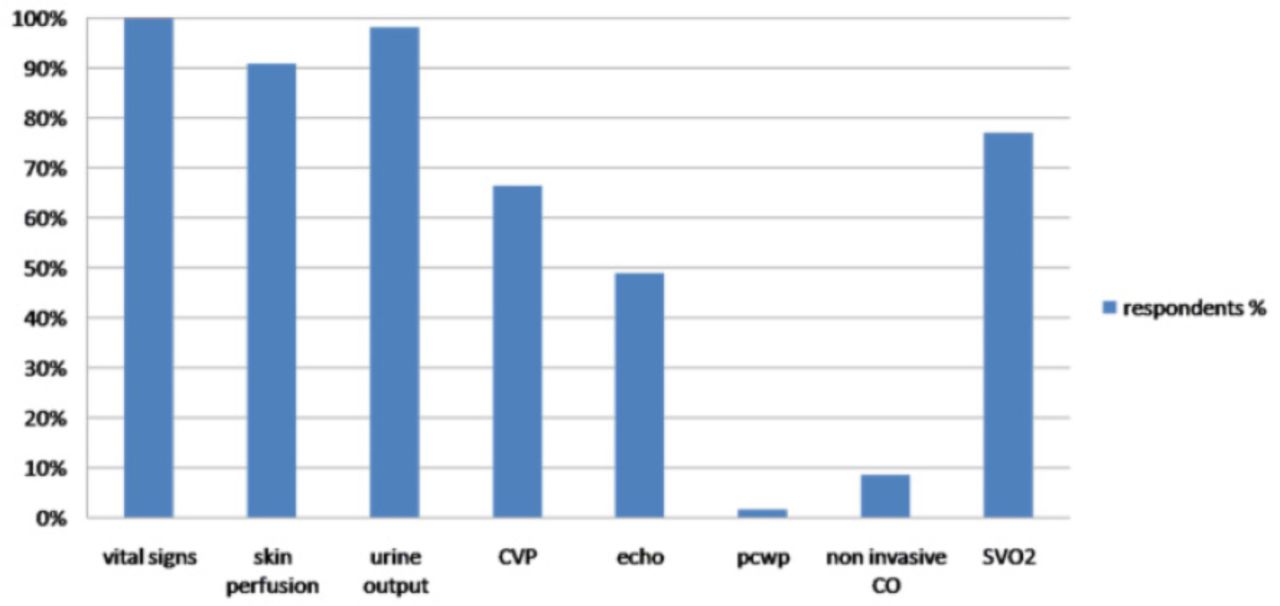
The clinical assessment (vital signs, urine output and skin perfusion) was reported as the most important parameter used to monitor clinical response to fluid resuscitation among surveyed pediatric intensivist (90-100%). Only 11 intensivists (18%) targeted a specific central venous pressure (CVP) level (8-12 or other level) during shock management. Figure 1 illustrates the parameters used to monitor clinical response to fluid resuscitation.

Parameters used to monitor clinical response to fluid resuscitation among surveyed pediatric intensive care consultants in Saudi Arabia. CVP – central venous pressure, PCWP – pulmonary capillary wedge pressure, ScvO2 – central venous oxygen saturation, echo – echocardiography, non invasive CO- noninvasive cardiac output.
More than two-thirds (72%) of the respondents reported considering catecholamines if the patient’s condition did not improve after 40-60 mL/kg of fluid resuscitation; 13% reported they would consider it after 20-40 mL/kg of fluid resuscitation and 15% after 60-80 mL/kg of fluid resuscitation. When considering the addition of catecholamines surveyed intensivist were divided; 29 intensivists (48%) reported they would start dopamine while 26 (44%) and 2 (3%) said they would consider starting epinephrine or norepinephrine. None reported using either dobutamine or vasopressin as a first choice.
Intubation would be considered by 53 (87%) intensivists if the patient remained hemodynamically unstable or if they had an altered mental status despite fluid resuscitation. Eight (13%) intensivists reported they would intubate the patient early upon arrival or with the first fluid bolus. Ketamine was the drug of choice as the sedating agent for intubation among 47 (77%) intensivists; 41% (n=19) of these intensivists reported they would use it alone and 59% (n=28) reported they would use it in combination with opiates/opioids, or midazolam. Three (5%) intensivists reported they would use etomidate in combination with an opiate to intubate pediatric patients in septic shock. None reported using propofol or barbiturates. Atropine would be used by 41% of intensivists, and short acting muscle relaxant by 74%.
Corticosteroids would be administered by 87% (n=53) of the intensivists for vasopressor refractory septic shock, while 8% (n=5) would consider corticosteroid only if the patient had reduced cortisol levels. Two (3%) respondents said they would give corticosteroids from the onset of the septic shock, one (2%) intensivist would never prescribe steroids for septic shock, and none reported conducting ACTH test before administering a steroid.
Supportive therapy for severe sepsis
The intensivists were asked regarding their transfusion practices in case that the patient became hemodynamically stable on 2 catecholamines with mixed venous oxygen saturation (ScvO2) of 60%. The following proportions indicated that they would consider blood transfusion under the given conditions: 2% if hemoglobin was below 12g/dl, 53% if hemoglobin was below 10g/dl, 8% if hemoglobin was below 9g/dl, 17% if hemoglobin was below 8g/dl and 20% if hemoglobin was below 7 g/dl.
Most of the pediatric intensivist (71%) reported that they would not give insulin if the patient developed hyperglycemia (blood glucose ≥10.5 mmol/L). The remaining respondents (26%) reported they would use an insulin infusion; they reported following an insulin protocol for most cases (82%).
Barriers for the surviving sepsis campaign guidelines
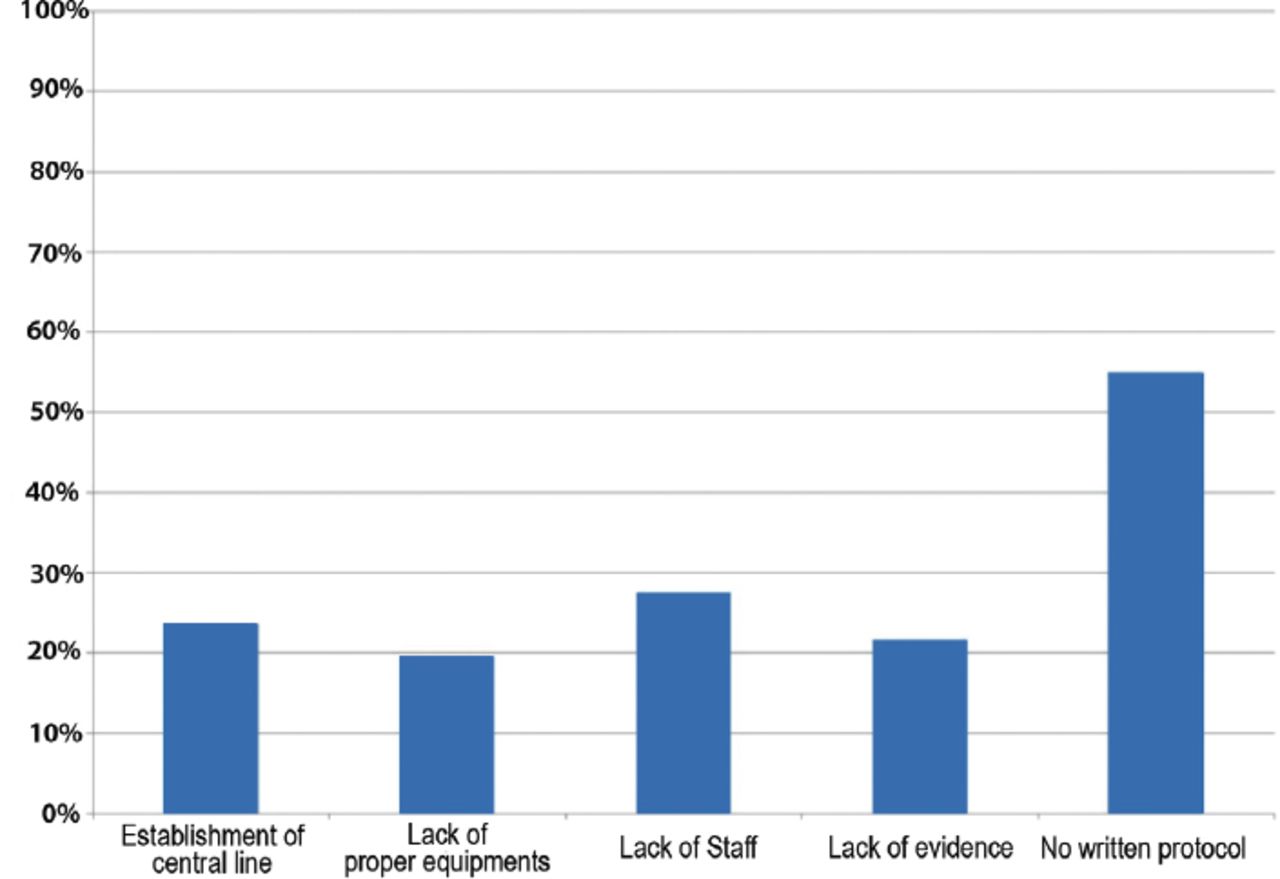
The most frequently reported barrier to the application of the SSC guidelines was the absence of a written protocol (55%), followed by the lack of staff, or equipment (47%), the difficulty in the establishment of a central venous catheter (24%), and the lack of evidence regarding the effectiveness of the recommendation (22%) (Figure 2).

Reported barriers to the uniform application of the surviving sepsis campaign guidelines
Discussion
The findings of this survey indicates a good, at least presumed, compliance of pediatric intensivists in KSA to the SSC guidelines with regards to fluid resuscitation, and initiation of vasopressors and early antibiotic therapy. Although previous studies have not shown a difference in outcomes when using crystalloids or colloid for fluid resuscitation,13,14 most respondents reported using crystalloids as the first choice for fluid resuscitation. Pediatric intensivists mainly use clinical parameters to assess fluid responsiveness as therapeutic end points (vital signs, urine output and skin perfusion), ScvO2, and CVP were second choices for assessment. Evaluation of the cardiac output via echocardiography and other noninvasive techniques are used much less frequently. Most of the responses, CVP was integrated as one of the parameters to evaluate fluid responsiveness rather than targeting a certain level of CVP. Recently, 3 trials in adult patients15-17 failed to demonstrate superiority of CVP and ScvO2 monitoring in patients with septic shock who received timely antibiotics and fluid resuscitation when compared with controls. Based on this evidence, the SSC committee has revised the 6-hour bundle to include, focused exam (vital signs, cardiopulmonary, capillary refill, pulse, and skin findings), in addition to a cardiovascular ultrasound, and dynamic assessment of fluid responsiveness.18 To date, there have been no similar studies in the pediatric population.
Pediatric intensivists are unanimous in initiating a vasopressor for fluid refractory shock; however, there were varying opinions regarding the types of vasopressors to be used. The pediatric guidelines recommend dopamine as the first vasopressor for fluid refractory shock (grade 2C), and in cases of dopamine refractory shock, the choice will be guided by the patient’s hemodynamic status.5 Interestingly, the first choice of vasopressor indicated by respondents was different from that recommended within the sepsis guidelines; and of respondents indicated they would use dopamine (48%) or epinephrine (43%). A decreased trend to use dopamine as the first choice vasopressor in cases of fluid refractory septic shock in pediatrics was reported in previous studies;9,19 furthermore, a recent randomized controlled trial of dopamine versus epinephrine as the first-line vasoactive drug in fluid refractory septic shock in children showed that patients treated with epinephrine had higher survival rates.20 Epinephrine use was associated with 6.5 times the odds of survival. These findings may lead to changes in practices regarding the choice of vasoactive agents commonly used.
Another interesting result from this survey is that the favored inducing agent for intubation in pediatric patients with septic shock was ketamine; Santchi et al9 reported a similar finding. The popularity of this drug for use among patients with septic shock could be explained by its relative ability to maintain cardiovascular stability.21
Almost all surveyed intensivists considered hydrocortisone therapy in children with fluid-refractory, catecholamine-resistant shock, and suspected or proven absolute adrenal insufficiency as recommended by the sepsis guidelines (grade 1A). A recent survey of practice regarding the use of steroid supplementation in pediatric sepsis showed that although corticosteroids are used at most centers for the treatment of pediatric sepsis, a significant variation in attitudes and use exists.22
A few of the sepsis guideline recommendations were less consensual among pediatric intensivists. First, when asked to state their hemoglobin threshold for blood transfusion in septic patients once the patient’s condition had stabilized and the ScvO2 was <70%, the respondent had a broad range of opinions. The optimal hemoglobin level for a critically ill pediatric patient with severe sepsis is not known. A multicenter trial reported no difference in mortality in hemodynamically stable critically ill children managed with a transfusion threshold of 7 g/dL compared with those managed with a transfusion threshold of 9.5 g/dL.23 Another randomized controlled trial of early goal-directed therapy for pediatric septic shock using the threshold hemoglobin level of 10 g/dL for patients with a SvcO2 <70% in the first 72 hours of PICU admission showed improved survival rate.6 Based on this rationale, the SSC guidelines recommend hemoglobin levels of 10 g/dL during resuscitation of low superior vena cava oxygen saturation shock (<70%), and a lower hemoglobin target >7g/dL after stabilization and recovery from shock and hypoxemia (grade 1B).
Second, more than two-thirds of intensivists reported not starting insulin infusion if blood glucose was >10.5 mmol/L; similar result was found in a previous survey.9 The pediatric guidelines suggest controlling hyperglycemia using a similar target as in adults (≤180 mg/dL), and highlight that glucose infusion should accompany insulin therapy in newborns and children. The grade of this recommendation is 2C, reflecting the absence of strong evidence of the benefit of tight glucose control in pediatric septic shock, and considering the known risk of hypoglycemia in this patient population. Pediatric intensivists showed a clear reluctance to comply with this specific recommendation. Previous surveys on glucose control in critically ill children reported that significant disparity exists between pediatric intensivists’ beliefs and actual practice regarding glycemic control, with the exception of few centers reporting the use of a consistent standard approach to screen and manage hyperglycemia.24,25 The fear of management-induced hypoglycemia was a the barrier to tight glucose control.26
Study limitation
The high level of compliance to the various aspects of the sepsis bundles did not exclude the presence of a perception reality gap. Indeed, what intensivists think they are doing is not necessarily what they are exactly doing in real life. In the sepNet trial,26 intensive care unit directors perceived adherence to sepsis guidelines to be higher than they actually were. Another possible limitation of this study was the time of intervention by pediatric intensivists, as some of the septic shock patients were initially managed by the emergency room physician.
In conclusions, this study indicates a high level of awareness of and adherence to the SSC guidelines among pediatric intensivists working in KSA. We found several variations in practice that reflect current beliefs. These results could be fairly generalized to the pediatric intensivists working in the gulf region, as most of them have similar level of training, similar PICUs settings, and similar populations’.
Withdrawal policy
By submission, the author grants the journal right of first publication. Therefore, the journal discourages unethical withdrawal of manuscript from the publication process after peer review. The corresponding author should send a formal request signed by all co-authors stating the reason for withdrawing the manuscript. Withdrawal of manuscript is only considered valid when the editor accepts, or approves the reason to withdraw the manuscript from publication. Subsequently, the author must receive a confirmation from the editorial office. Only at that stage, authors are free to submit the manuscript elsewhere.
No response from the authors to all journal communication after review and acceptance is also considered unethical withdrawal. Withdrawn manuscripts noted to have already been submitted or published in another journal will be subjected to sanctions in accordance with the journal policy. The journal will take disciplinary measures for unacceptable withdrawal of manuscripts. An embargo of 5 years will be enforced for the author and their co-authors, and their institute will be notified of this action.
Acknowledgment
Authors gratefully thank Professor Francis Leclerc, Jeanne de Flandre Hospital, Lille, France, for allowing them to utilize and adapt the questionnaire used for this study. Authors also thank all the members of Saudi Critical Care Society, Pediatric Chapter who responded to the survey.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. (IRB log number: 16-118)
- Received November 17, 2016.
- Accepted March 8, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}