


Abstract
Objectives: To investigate the awareness and usage of oral and maxillofacial pathology (OMFP) subspecialty services among pathologists in Saudi Arabia.
Methods: In this cross-sectional study, we conducted an electronic questionnaire survey of pathologists in all regions of Saudi Arabia. The study was conducted between July 2015 and August 2016. The questionnaire comprised 19 questions to evaluate the knowledge of pathologists regarding microscopic OMFP and their perceptions towards this subspecialty.
Results: Most of the pathologists surveyed (94.6%) were aware of the OMFP subspecialty and its scope of practice. Although most of the pathologists recognized the importance and need of this subspecialty, 70% of them never referred or consulted an oral pathologist as they either diagnosed the cases themselves or did not know any oral pathologist (57.7%). The pathologists had the greatest difficulty in identifying and diagnosing odontogenic tumors, salivary gland tumors, and odontogenic cysts.
Conclusion: Pathologists are aware of the OMFP subspecialty, but their utilization of the services offered by OMFP specialists in Saudi Arabia is quite low despite the strong demand for OMFP services.
Pathology, as a medical specialty, is now facing an increasing demand to improve patient safety, diagnostic quality, and accuracy, which highlighting on the importance of subspecialization.1 Oral and maxillofacial pathology (OMFP) is a subspecialty that focuses on the clinical, radiographic, and microscopic diagnosis of pathological conditions affecting the oral and maxillofacial regions.2 The importance of microscopic diagnosis of tissues collected during oral surgical procedures cannot be underestimated, and the failure to submit biopsy samples for analysis could result in postponed or ignored diagnosis.3 The hiring and consultation of oral and maxillofacial diagnostic histopathology specialists by general pathologists at hospitals or private laboratories are limited. Previous surveys and reports of oral pathology diagnostic services have suggested that experienced pathologists diagnosed oral and maxillofacial diseases by themselves despite they could not have the equivalent level of proficiency when examining oral samples.4 A study conducted at Johns Hopkins Hospital, Baltimore, MD, USA revealed that head and neck lesions were the third most erroneously diagnosed lesions after female reproductive system and gastrointestinal system lesions due to a shortage of experience among pathologists with diagnostic histopathological patterns of head and neck lesions and the lack of sufficient exposure to these lesions.5,6 A misdiagnosed malignant lesion or other serious pathology could potentially result in an unfavorable prognosis and management of patients. Major disagreements in the diagnosis of head and neck pathologies have been reported previously, with the extent of discordance ranging from 7% to 16.3%.6,7 Such discordance could have serious consequences on prognosis and extent of management. In Kingdom of Saudi Arabia (KSA), OMFP is a distinct registered specialty at the Saudi Commission for Health Specialties (SCFHS), but there are no clear guidelines regarding who is qualified to practice OMFP and what is the scope of their practice. This study aimed to assess the level of awareness of the OMFP subspecialty among pathologists and to clarify the patterns of utilization of this service at diagnostic laboratories.
Methods
In this cross-sectional study, we electronically distributed an English language questionnaire survey by e-mail to all pathologists and residents whose e-mails were available at the online websites of different institutions from different regions of KSA. The questionnaire inquired regarding the pathologists’ knowledge and position about OMFP services based on previous survey conducted at United Kingdom.8 A reminder was sent 2 weeks and one month after sending the initial e-mails. The study was conducted between July 2015 and August 2016. All incomplete answered questionnaires were excluded from the study. The pathologists participated voluntarily in the study and were informed about the confidentiality of their responses.
The questionnaire was adopted and modified using Barret and Speight survey;8 and comprised 19 questions in different formats. The participants were requested to answer yes/no, multiple-choice, and free-text questions. The questionnaire started with questions on the demographic data of the participants, including age, gender, position, and years of experience. Next section of the survey focused on the knowledge of microscopic OMFP and the perception regarding this subspecialty among the participating pathologists.
Additional questions included whether the pathologists aware of qualification of OMFP specialists and number of OMFP specimens received yearly in their service. To validate the questionnaire, we distributed it in paper and pretested among 18 pathologists from different hospital to ensure the clarity of the contents. Based on this pretest, we kept some questions with unlimited answer such as “ranking” and “the most difficult/ challenging specimens to diagnose”. Adding the word “challenging” beside the word difficult was recommended by many expert participants. We made final modifications to the questionnaire before electronically sending it to the participants. The research ethics board of King Abdulaziz University Faculty of Dentistry, Jeddah, KSA approved the study (protocol number 15-053), which was conducted in compliance with the Helsinki Declaration.
Statistical analysis of the data collected was analyzed using the Statistical Package for the Social Sciences version 22 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to derive values in the form of counts and percentages in order to define the characteristics of the study variables.
Results
We e-mailed the questionnaire to 104 pathologists from different regions in KSA. The survey was viewed by 77 recipients and completed by 37, with an overall response rate of 36% from all the pathologists and residents who opened the survey. Approximately 40% of the respondents were 40 to 50 years old, and the male to female ratio was 1.5:1. The demographic data of the participants are listed in Table 1.
Demographic data of 37 pathologists included in the study.
Most of the respondents were familiar with the OMFP subspecialty (94.6%), and only 5.4% had never heard about it. However, the respondents’ knowledge about the qualifications of the OMFP specialists varied highly. Moreover, the respondents were unsure whether the OMFP specialists had graduated from medical or dental schools and whether they underwent residency in the anatomic pathology department or in the OMFP department only. Approximately 48.6% of the respondents considered that an OMFP specialist should have American or Canadian board to practice (Table 2).
Qualification of OMFP based on pathologists’ opinion in Kingdom of Saudi Arabia.
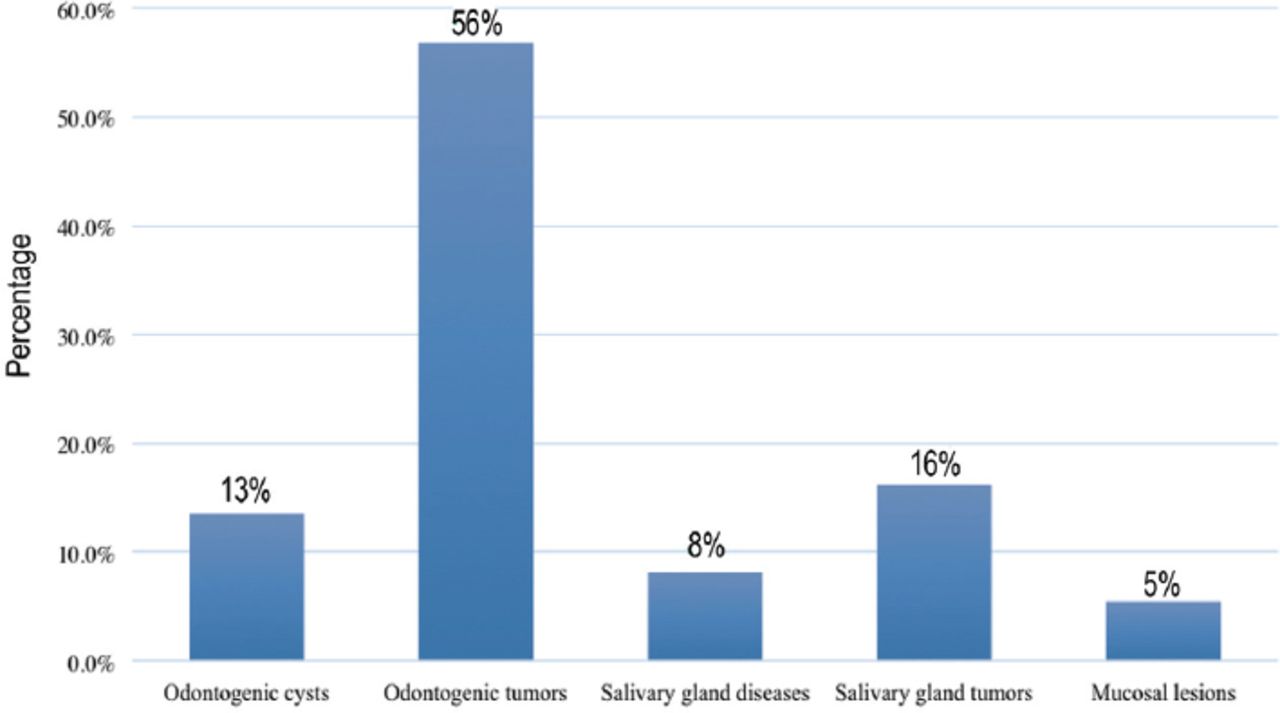
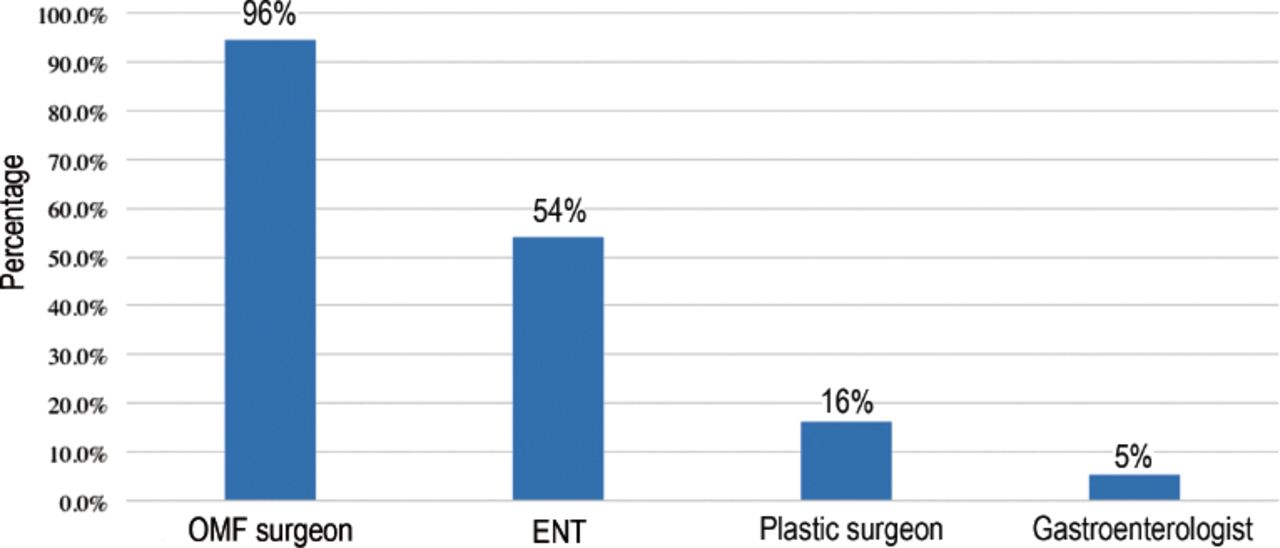
Seventy-eight percent of the respondents reported receiving more than 3000 oral and maxillofacial specimens per year at their services. Among these specimens, odontogenic tumors were the most difficult to diagnose, followed by salivary gland tumors and odontogenic cysts (Figure 1). According to the respondents, most of these specimens were sent in by oral and maxillofacial surgeons (94.6%), followed by ear-nose-tongue surgeons (54%). Each respondent could choose one or more options, as appropriate. Only 16% of the pathologists reported receiving OMFP specimens from plastic surgeons, and 5% reported receiving them from gastroenterologists (Figure 2). During their years of practice, 70% of the pathologists had not referred or consulted an OMFP specialist because they diagnosed the cases themselves, 57.7% did not know any OMFP specialist, 5% had difficulty communicating and sending the specimens to an OMFP specialist, and one respondent (3.3%) said he did not know oral pathology specialty.
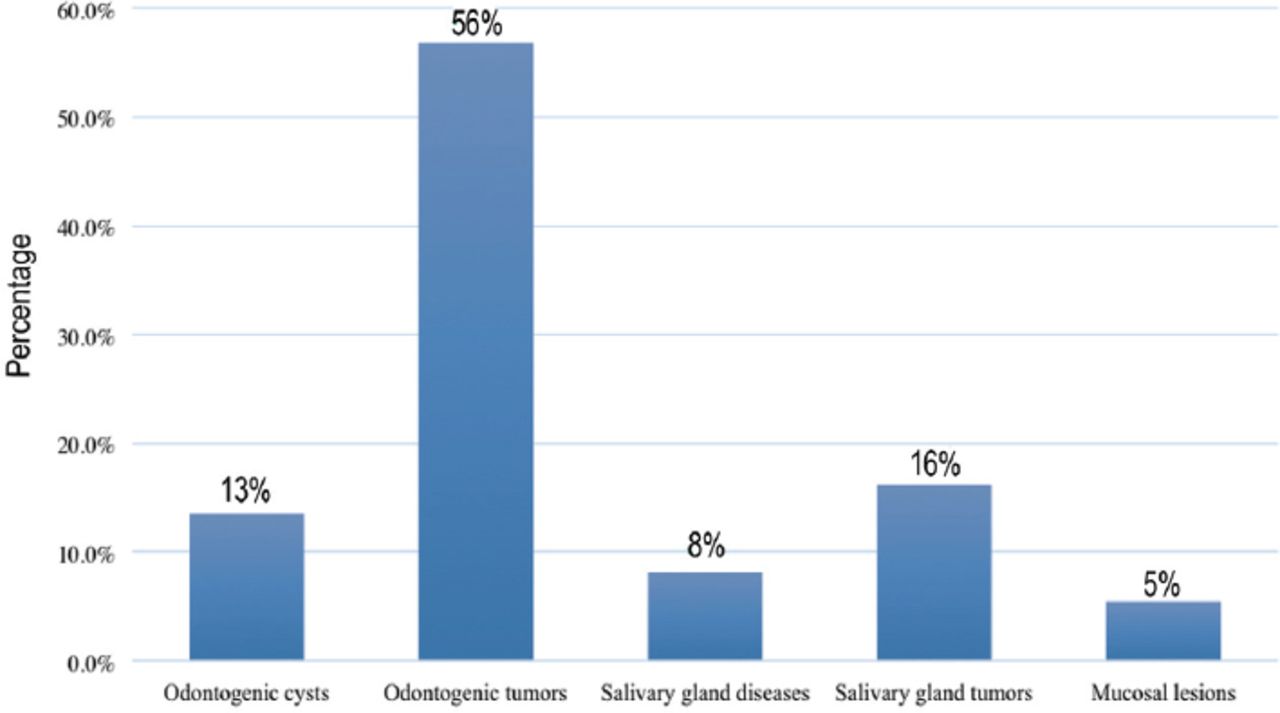
The oral and maxillofacial pathological lesions that are the most difficult to diagnose for general pathologists.

Source of specimens of oral and maxillofacial (OMF) pathology based on the pathologists’ opinions. ENT - ear-nose-tongue surgeon
In the last 4 years, the pathologists had referred or requested a second opinion from an OMFP specialist for odontogenic tumors, odontogenic cysts, salivary gland tumors and diseases, mucosal lesions, and bone pathology. The percentage of nature of the specimens sent for referral is illustrated in Figure 3. Despite the need for this specialty and most of the respondents feeling that they had a very good experience dealing with oral pathologists, 37% of the histopathologists did not hire an OMFP specialist at their department or laboratory. Furthermore, 29.7% were unsure if they needed oral pathology services and stated they would refer the application to their administrative office to decide if there was a need for such a specialty in their laboratory. They felt that this specialty should be hired in healthcare centers receiving large numbers of head and neck specimens or at tertiary medical centers. One consultant commented that OMFP specialists should not be hired as full-time pathologists and should be consulted on a case-by-case basis. One specialist was afraid that subspecialization would prevent general pathologists from gaining experience in identifying lesions from specific areas such as the head and neck.
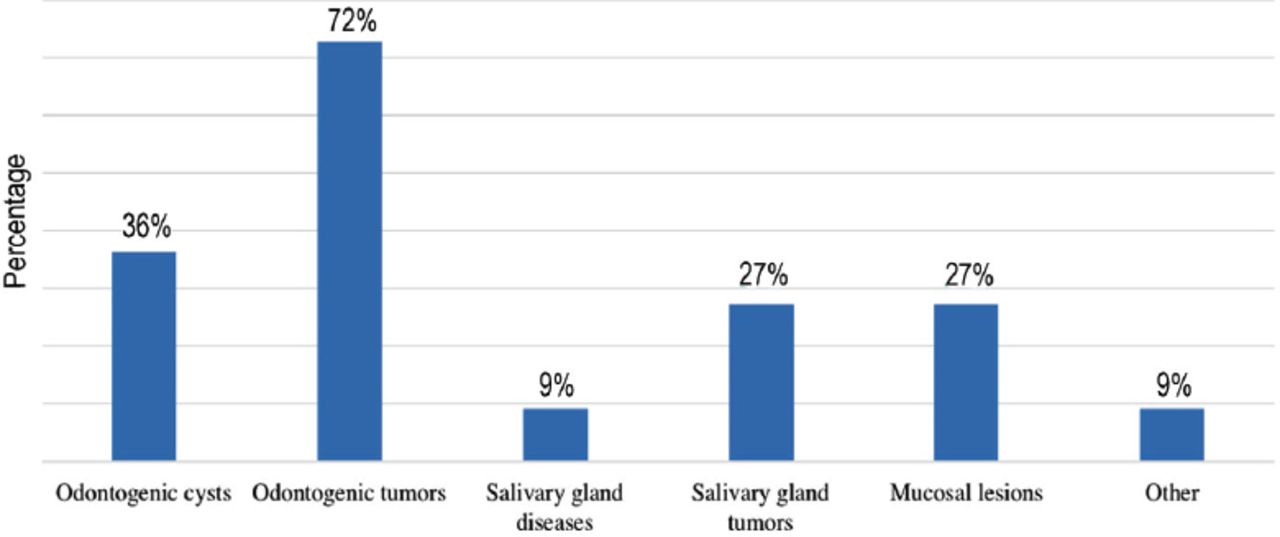
The nature of the specimens sent to oral and maxillofacial pathology specialists for a second opinion.
Discussion
This survey was conducted to clarify the pathologists’ attitude towards and knowledge of the services provided by OMFP specialists and their utilization of the specialty. Only one previous study has aimed to define the subspecialty and its use by histopathologists in the UK.8 The results of the current study showed that 94.6% of the respondent pathologists were aware of the OMFP services and considered that 94.6% of the OMFP specimens were sent by oral and maxillofacial surgeons. Seventy percent of the respondents never sent any specimen for a second opinion or consultation to an OMFP specialist during their experience because of various reasons. The respondents stated that the most difficult lesions to diagnose were odontogenic tumors (72.7%).
Oral and maxillofacial pathology is a recognized specialty in many countries wherein the practitioners undergo training for 4 years after their dental degrees. It is mandatory for the OMFP trainees to rotate at general/anatomic pathology, autopsy, and molecular pathology services. Exposure to other pathology subspecialties such as gastroenterology, otorhinolaryngology, endocrinology, dermatology, and hematopathology is also mandatory. To be considered a qualified OMFP specialist in some countries, a diploma or a fellowship is also needed from accrediting organizations, such as the American Board of Oral and Maxillofacial Pathology in the USA or the Royal Colleges of Pathology in the UK and Australia, whereas other countries provide academic degrees such as masters or doctor of philosophy.9 Approximately 94.6% of the respondents were aware of the OMFP qualification requirements and their scope of capabilities, but we were surprised that only 32.4% of the pathologists were prepared to consider hiring an OMFP specialist at their department. These results are not consistent with those of a previous study conducted in the UK by Barret and Speight8 wherein 96% of the participants were aware of the specialty and 92% used it. Regional differences exist, thus OMFP specialists are responsible for informing their own society and referral groups about the scope of their service, experience, and areas of interest. Second opinion or outside cases are the major source of referrals to an OMFP practice.10,11 A 10-year study at Johns Hopkins Cancer Center (Baltimore, Maryland, USA) showed that the diagnoses in 7% of outside cases of head and neck lesions were later changed or modified. The tumor classification had to be changed in approximately 61% of the cases; the classification changed from benign to malignant in 24% and vice versa in 15%. These findings reflect the difficult nature of head and neck or oral and maxillofacial pathologies and their complex classification. The lack of significant information in reports of head and neck tumors, such as margin status, perineural invasion, extracapsular invasion of the involved lymph nodes, and p16 immunohistochemistry, may indicate the need for a second opinion from an OMFP specialist. This is also important because accurate assessment of these tumor characteristics has a deep impact on the patient’s prognosis.7
A study conducted at the Mayo Clinic (Rochester, Minnesota, USA) assessed the discordance between diagnoses made on the basis of histopathology slide reviews at external institutions and at the Mayo Clinic, where the specimens were sent for definitive diagnosis. The most common disagreements were in gastrointestinal (GI) pathology (18%), followed by lymphoid pathology (16%), and breast pathology (10%). Disagreements in cases of head and neck pathologies were seen in 7% of the cases. There was 23% overall disagreement in the cases analyzed, which led to a change in tumor classification from benign to malignant across all specialties.12 Another study conducted at the University of Iowa (Iowa City, Iowa, USA) found a major disagreement in the diagnoses (approximately 2.3%) most common in gynecological, GI, dermatological, and head and neck pathologies, with 1.2% of these disagreements prompting a total change in case management.13
Subspecialization is highly encouraged in all specialties of pathology, and many studies have proven the importance of a second opinion, such that each pathologist reports cases within his/her area of expertise and interest. This will increase the proficiency, productivity, and efficiency of work the pathologists conduct.14,15 Moreover, this will help organize the diagnostic workload and reduce the turnaround time and costs.10 Furthermore, pathologists are now regularly dealing with subspecialized surgeons, and having specimens analyzed by subspecialized pathologists will make the diagnostic process more efficient because the diagnosis will be performed by someone with expertise in that subspecialty. This will also help establish a “one-stop-shopping” service for the clients.14,16
A previous study on dental schools in the USA reported that each laboratory diagnosed on average 3400 specimens per year, and malignant specimens accounted for 3% of the total number.11 This finding is consistent with that of our study, in which 78% of the respondents said they received more than 3000 OMFP specimens yearly. In our survey, general pathologists would refer difficult cases, such as odontogenic tumors and cysts, salivary gland tumors, and mucosal lesions, to oral pathologists; however, in a UK survey conducted in 1996, the pathologists considered salivary gland lesions, odontogenic tumors, and mucosal lesions as the most difficult.8 The sample size of the current survey was of concern because of the limited number of pathologists in KSA. Despite this limitation, the response rate of the questionnaire was 36%. The practicing oral pathologists in KSA are commonly employed by the government and should be licensed by the SCFHS. However, their scope of practice has not been specified, and it remains unclear whether their domain should be limited to the oral and maxillofacial region or should also include the head and neck region. There is a clear need for this subspecialty in KSA and a greater need to develop training programs covering advancements in the field of oral pathology.
Kingdom of Saudi Arabia is the largest among the Gulf Cooperation Council countries, with a mix of urban and rural regions. This study shows that despite there being great recognition regarding the OMFP subspecialty among medical pathology consultants, their posture regarding referring the cases and consulting OMFP specialists is quite poor.
In conclusion, there is a significant need to increase awareness regarding OMFP as a specialty branch and to encourage referral and/or hiring of OMFP specialists at tertiary centers with central pathology laboratories, irrespective of whether they are government owned or in the private sector.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded.
- Received December 12, 2016.
- Accepted March 8, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.