


Abstract
Objectives: To detect common skin-sensitizing agents among patients experiencing allergic contact dermatitis (ACD).
Methods: This was a retrospective study of 152 patients with clinically suspected ACD who underwent patch testing in an allergy clinic at King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia between January 2012 and February 2015. Of these patients, only 74 (48%) patients reacted to one or more contact allergens. This group of patients included 58 (78.4%) women and 16 (21.6%) men (mean age: 37.8±13.8 years). Patch testing was performed using the thin-layer rapid-use epicutaneous patch test panels.
Results: Nickel sulfate was the most common sensitizing agent, with 26 (35.1%) patients yielding a positive result; followed by p-phenylenediamine in 17 (22.9%), butyl-tetra-phenol formaldehyde in 12 (16.2%), gold sodium thiosulfate in 10 (13.5%), and thimerosal in 6 (8.1%) patients. Nickel reactivity was significantly higher among women (41.4%) than among men (12.5%) (p<0.0001). Similarly, gold reactivity among women (15.5%) was also higher than among men (6.2%) (p≤0.02).
Conclusion: The high level of skin sensitization due to nickel, PPD, and gold in patients with ACD emphasizes the need for measures to decrease exposure to these sensitizing agents.
Allergic contact dermatitis (ACD) is a chronic inflammatory disorder. The prevalence of ACD varies in different parts of the world,1-3 with prevalence rates of 1.5-5.4% in the US, and up to 28% in Spain.4,5 Several factors such as the type of the allergen, duration of exposure, region, age, gender, and race have been implicated in the induction of ACD and may contribute to differences in prevalence rates.6 Genetic predisposition is considered an essential prerequisite for the development of ACD.7 As opposed to irritant reaction which is considered non-specific, ACD is believed to be caused by prolonged and repeated contact with a specific allergen or hapten.8 The induction of ACD occurs following penetration of haptens into skin layers after physical contact, which binding to extracellular proteins, result in the formation of hapten-peptide complexes. These complexes are transported to draining lymph nodes resulting in T-cell activation.9 The most common sites involved in ACD are the hands, especially the fingertips, nail folds, and dorsum.10 Various allergens have been implicated in ACD. The most common allergens in the United Kingdom are nickel and fragrance mix whereas in Thailand, gold and nickel are considered the most common sensitizing allergens.11,12 Similarly, in Iran, nickel sulfate and cobalt chloride are frequently involved in the causation of ACD.13 In India, potassium dichromate and nickel sulfate, in United Arab Emirates, nickel sulfate and fragrance mix, and in Kingdom of Saudi Arabia (KSA), nickel sulfate and p-phenylenediamine have been reported as common skin-sensitizing allergens.14-16 Collectively, these data indicate that nickel sensitization is universally prevalent and is a leading sensitizing allergen. This study aimed to determine common sensitizing agents among patients with ACD attending the allergy clinic at King Khalid University Hospital, Riyadh, KSA.
Methods
This was a retrospective analysis of patch test data from 152 patients with clinically suspected ACD who were referred to the allergy clinic at King Khalid University Hospital in Riyadh, KSA between January 2012 and February 2015. Of these, 74 (48%) patients were found to have a positive patch test, reacting to one or more allergens. This group comprised 58 (78.4%) female and 16 (21.6%) male patients with a mean age of 37.8+13.8 years. Among the positive reactions, 42 (56%) patients yielded positive results for a single allergen, while 32 (43%) reacted to more than one allergen. All patients both males and females with clinical suspicion of ACD attending allergy clinic at King Khalid University Hospital were included in this study except pregnant women and patients on immunosuppressive therapy. The patch test was performed using Thin-layer Rapid-Use Epicutaneous (TRUE) patch test (Mekos Laboratories AS Mekos Laboratories AS, Herredsvejen 2, 3400 Hillerød, Denmark) containing 36 contact allergenic substances.15 Prior to patch testing, the patients were informed about the test procedure and its indications. They were advised to take a shower before being patch tested and were to avoid physical exercises, sweating, or lying on the back since the test panels were applied on their backs. They were also to avoid taking a shower during the test duration.
Patch test panels were applied on the patients’ upper back after ensuring the skin was intact and free of scars, acne, dermatitis, or any other skin condition that could interfere with the results. The patch test panels were left for 48 hours and the interpretation of the results was performed at 72 hours as patient compliance at 96 hours was inconsistent. The patch test reactions were graded from no reaction to +, ++, and +++, depending on the intensity of the reaction in accordance with the recommendations of the International Contact Dermatitis Research Group and the North American Contact Dermatitis Group.16 Statistical analysis of the data was performed using the Statistical Package for the Social Sciences version 21 (IBM, Armonk, NY, USA). The chi-square test was used to compare gender differences in the parameters. p<0.05 was considered statistically significant. chi-square was used for statistical test used analysis. Ethical approval was taken from the Institutional Review Board, King Saud University
Results
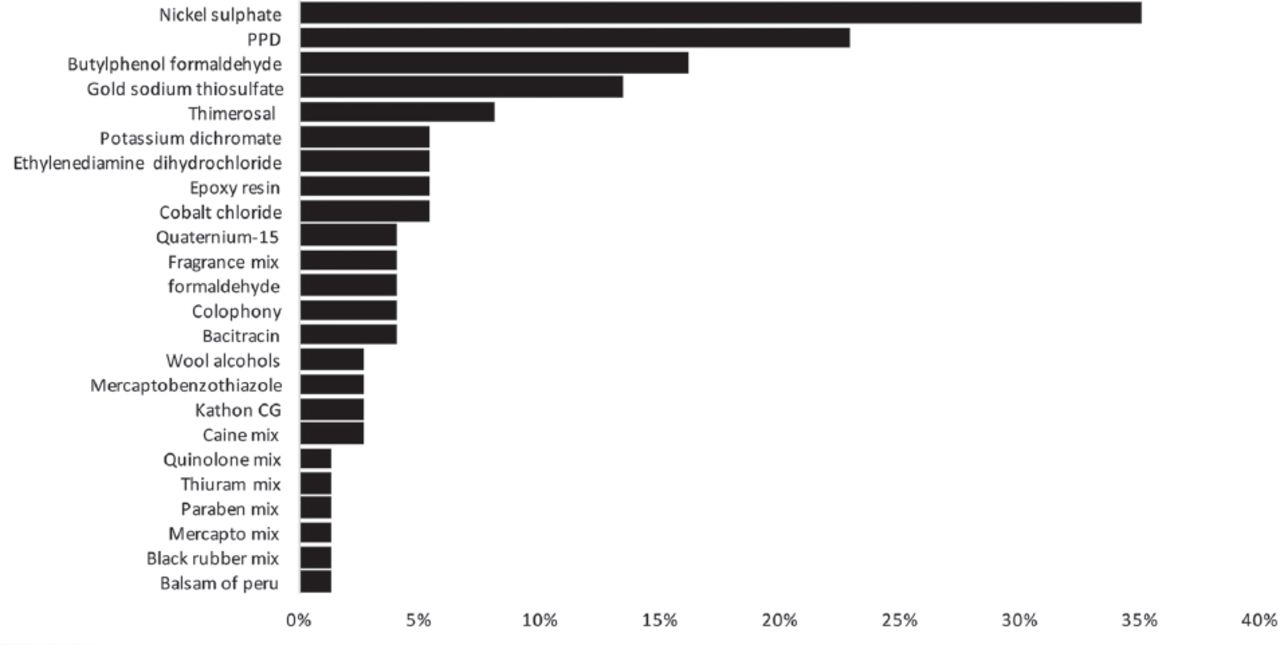
Figure 1 shows the data for the patch test reactivity among the patients with ACD. Among the allergens tested, nickel sulfate was the most common sensitizing allergen, with 26 (35.1%) patients reacting positively. The other common sensitizing allergens in descending order were p-phenylenediamine (PPD) in 17 (22.9%), butyl-tetra-phenol formaldehyde (P-TBPF) in 12 (16.2%), gold in 10 (13.5%), Thimerosal in 6 (8.1%), and potassium dichromate, cobalt chloride ethylenediamine dihydrochloride, and epoxy resin in 4 (5.4%) patients each.
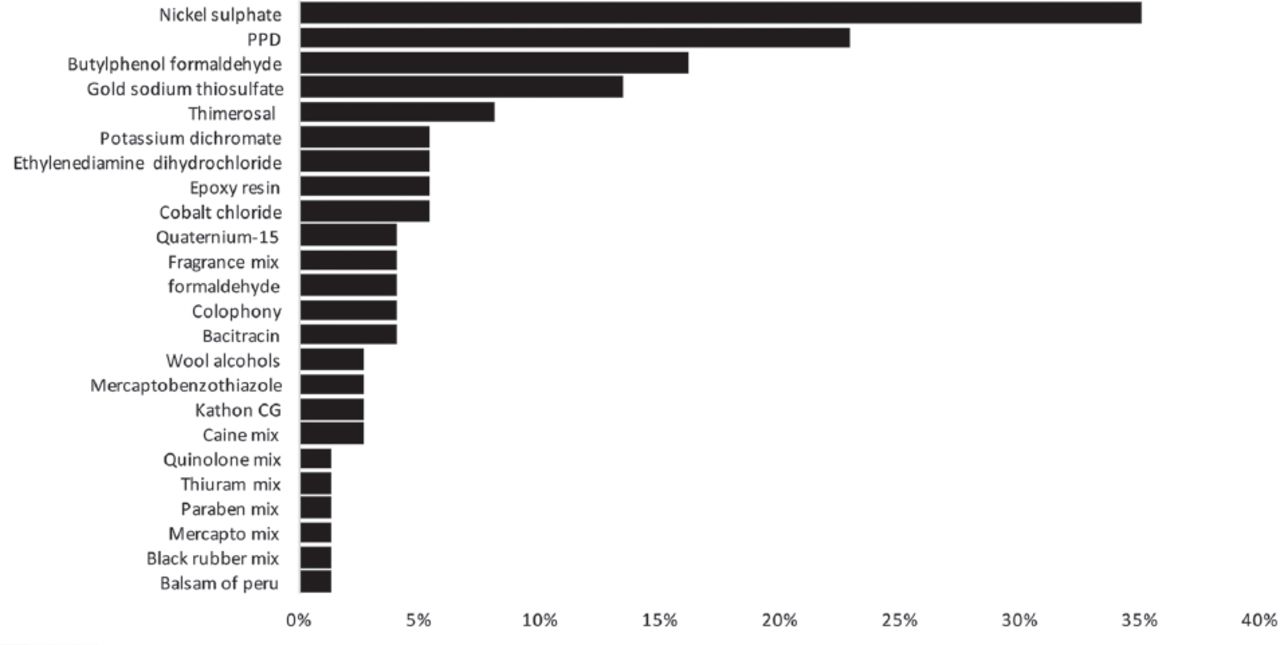
Pattern of allergens reactivity among patients with allergic contact dermatitis, PPD - p-phenylenediamine.
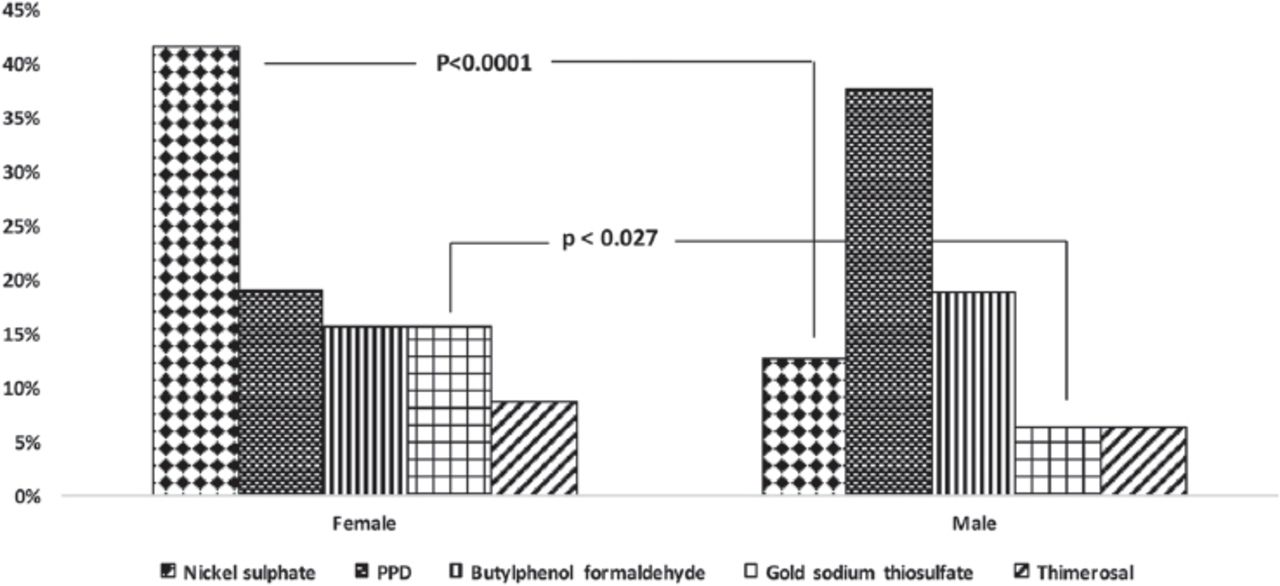
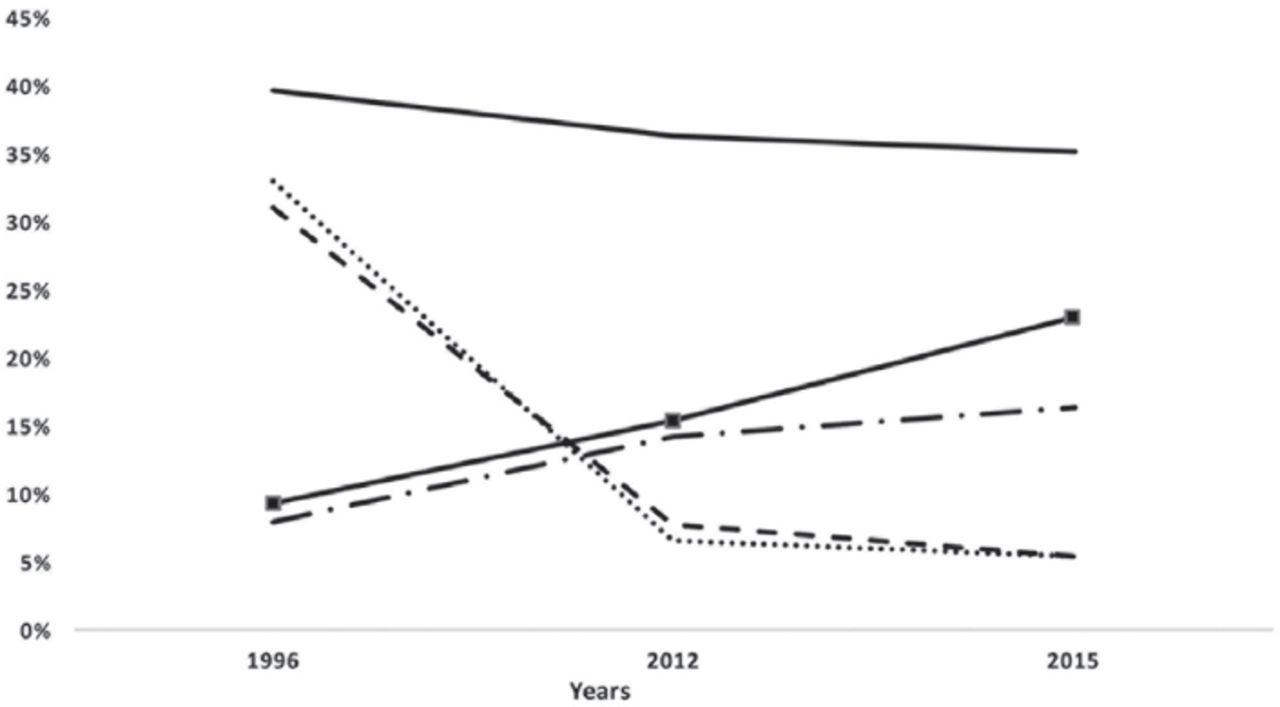
Figure 2 shows data for gender differences in patch test reactivity among patients with ACD. Nickel sulfate was the most common sensitizing allergen among women, and was significantly higher in women than in men (41.4% versus 12.5%; p<0.0001). Similarly, gold reactivity was higher in women than in men (15.5% versus 6.2%; p<0.02). Although Thimerosal reactivity was higher in women compared with men, the difference was non-significant (8.6% versus 6.2%). The most common sensitizing allergen among men was PPD, where 37.5% of men tested positive compared with 19% of women (p=0.332, non-significant). P-TBPF reactivity among men (18.7%) was higher than among women (15.5%) but the difference was not statistically significant. Figure 3 shows a comparison of the present study’s findings with that of previous studies.21,15 on patch test reactivity from the same clinic at King Khalid University Hospital over the last 2 decades. Nickel sulfate, the most frequently observed sensitizing allergen in the present study (35.1%), was consistently ranked as the most common sensitizing allergen in studies performed in 1996 (39.5%) and 2012 (36.2%).21,15 Sensitization due to PPD, the second most common sensitizing allergen in the present study (22.9%), increased in reactivity over the years from 5.4% in 1996 to 9.2% in 2012. Similarly, P-TBPF sensitization also increased from 7.9% in 1996 21, to 14.2% in 2012, and 16.2% in 2015. Sensitization to cobalt chloride and potassium dichromate have, however, declined since 1996. Cobalt reactivity in 1996 was 30.9% and declined to 7.69% in 2012 and to 5.4% in the present study. Similarly, the potassium dichromate reactivity of 32.9% in 1996 decreased to 6.59% in 2012 and to 5.4% in this study.

Comparison of patch test reactivity between male and female patients with allergic contact dermatitis.
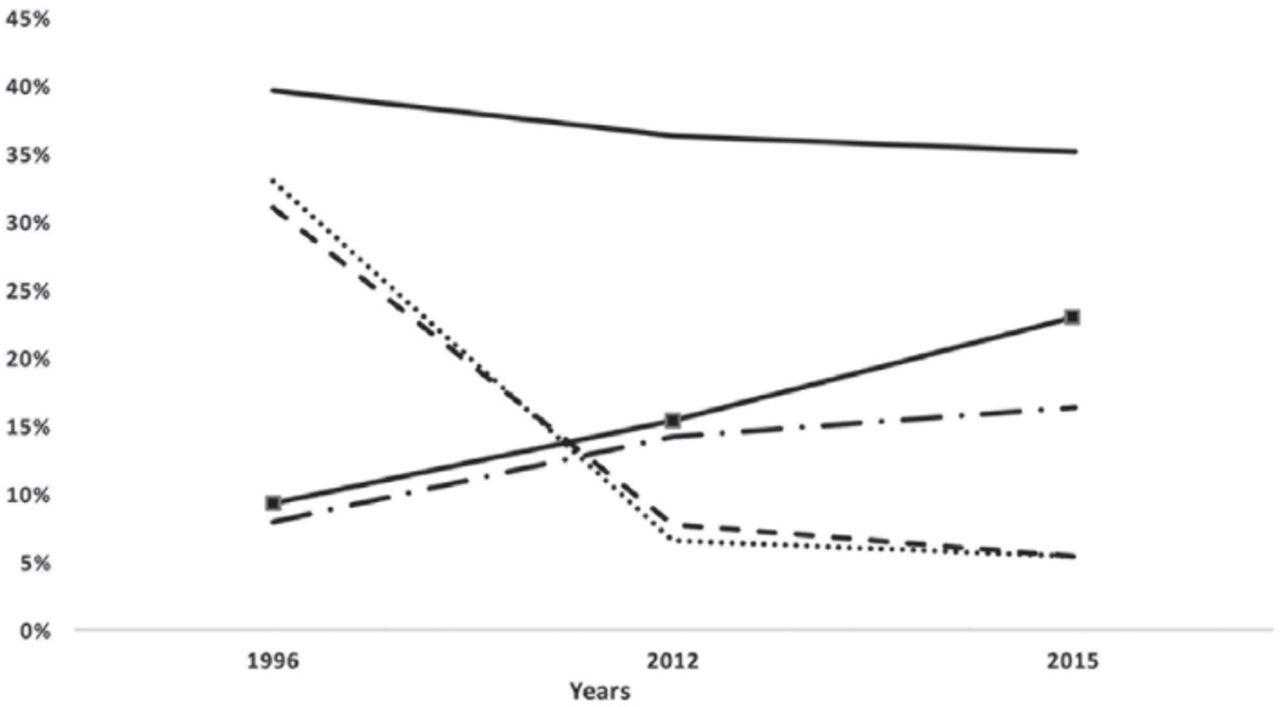
Comparison of the present data with previously published studies from King Khalid University Hospital.
Discussion
The most common sensitizing allergen in the present study was nickel sulfate. Although the present study was performed in a single center and does not represent the prevalence of nickel sensitization in KSA, the observed prevalence was notably higher than the worldwide prevalence rate of 8.6%.17 Nickel as a common sensitizing agent has been reported in a number of studies. Nickel reactivity have been reported from Italy of 27.4% and Iran 25% among patients with ACD.11,18 however, these values are less than that observed in the present study. The prevalence of nickel sensitization has also been reported from other countries and have ranged between 9% and 15%.19,20 The high level of nickel reactivity observed in the present study suggests increased exposure to the metal particularly among the female population. This is consistent with the findings of other studies performed in KSA.15,21 High prevalence rates of nickel sensitivity have been attributed to the abundant distribution of this naturally occurring metal that can be found in food, soil, and water.22 It exists in batteries, jewelry, cosmetics, clothes, wristwatches, and some household products such as washing liquids and powders.23-26 Due to the wide distribution of nickel-containing products, it is difficult to avoid exposure to the metal.15 Some European countries have achieved reduction in the prevalence of nickel sulfate sensitivity since 1991 by limiting exposure to the metal.27 This was mainly accomplished by preventing the sale of nickel-containing products that contributed to lifelong exposure to this allergen.28 Along with the reduction in the use of nickel jewelry, increased awareness regarding the avoidance of nickel products proved to be an effective measure in reducing the prevalence of nickel allergy.29 Considerable reduction in sensitization to nickel among women was observed in the Danish population following the implementation of legislation avoiding exposure to nickel products.30 The high level of nickel reactivity observed in the present and previous studies from KSA indicate increased nickel exposure among the local population.
Among the male patients, PPD was the most common allergen in the present study. p-phenylenediamine, which is usually found in hair dyes and black henna, has been implicated in ACD in the United Arab Emirates.31
A marked increase from 9.2% in 1996 to 15.3% in 2012 in patch test reactivity to PPD, reported in previous studies from KSA, suggests increased exposure to the allergen.15,21 A similar increase in the crude prevalence of PPD, from 1.4% in 1992 to 2.1% in 2009, was observed in the Swedish population where women were more frequently sensitized, most likely due to the widespread usage of hair dyes.32 Butyl-tetra-phenol formaldehyde reactivity was observed in 16.2% patients with ACD in the present study. This appeared to be higher than the 10% and 2.2% to less than 0.2% reactivity reported from North Ethiopia33 and a number of previous studies, respectively.19,34,⇓ para-tertiary-butylphenol-formaldehyde is found in leather products such as shoes, handbags, watchstraps, building materials, motor cars, and electrical products.36
In the present study, 13.5% of patients with ACD had a positive patch test for gold. It is generally believed that gold is a rare cause of ACD due to its natural characteristic as an inert metal.37 It is likely that gold has recently been included in testing panels as a sensitizing allergen and data supporting reactivity against gold are now emerging.28 Gold is widely used in jewelries and as a systemic therapeutic agent for the treatment of rheumatologic and dermatologic diseases along with its use in dental restorations.28,38,⇓ Most of women with a positive patch test for gold reflect a cultural and traditional use of gold jewelry in the local population. Similar findings have also been reported from Thailand where 30.7% of patients with ACD were found to be sensitized to gold, most likely due to the traditional and religious practices involving extensive use of gold jewelry.12 A high level of Thimerosal reactivity has been reported among children (13.3%) compared with adults (10.8%) and elderly (7%) patients from North America.40 Thimerosal is used as a preservative in several medical preparations, topical antimicrobial agents, and vaccines such as Haemophilus influenzae type b and hepatitis B vaccines. It is also used in polysaccharide vaccines for meningococcal strains A, C, Y, and W-135. There have been several public health concerns about its use in the US because of the associated toxicity to human cells.41 In this study, 8.1% of patients reacted to Thimerosal and this was less than the previously reported figure of 14.2% from KSA.15 Reduction in exposure to Thimerosal observed in the recent years, particularly in Denmark, is considered to be due to the avoidance of Thimerosal-containing vaccines.42,43 It is therefore important to identify and avoid the sources of Thimerosal exposure in the local population.
Potassium dichromate reactivity was observed in 5% of the patients in the present study. Exposure to potassium dichromate is considered to be occupational as it is a major component used in the cement and tile industry.18 Notably higher prevalence rates of potassium dichromate sensitization of 20.5% and 51% have been reported from India.44,45 A study performed in KSA in 1996 reported a 33% potassium dichromate reactivity among patients with ACD, which was attributed to increased activity in the construction industry at that time.21 The potassium dichromate reactivity observed in the present study reveals a significant reduction in exposure to the chemical. Similarly, the 31% cobalt reactivity reported in 1996 from KSA, has declined to 5% as observed in the present study.
Study limitation
It was limited by its retrospective nature and small sample size. Thus, large-scale prospective studies seem necessary in KSA to gain a better understanding of allergen exposure among the local population.
In conclusion, nickel was identified as the most common sensitizing allergen, particularly among women, whereas PPD was the second most common allergen and predominantly sensitized male patients with ACD. Comparison with previous data indicates that nickel reactivity has remained consistently high over the last 2 decades and sensitization to PPD has increased over the same period. Sensitization to gold was also notably high in this study. The high level of skin sensitization due to these substances emphasizes the need for multifaceted measures to decrease exposure to them.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. This study was supported by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia. (KSU-E-16-2086)
- Received March 30, 2017.
- Accepted June 28, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.