


REVIEW ARTICLE
Pulmonary edema post-adenotonsillectomy in children
Ahmed & Almutairi present epidemiological data on the prevalence of post-adenotonsillectomy pulmonary edema (pATPE), and address the mechanisms of development, types, etiology, pathophysiology, and management of pATPE. In order to minimize postoperative intensive care unit admission rates of pATPE, utilization of preoperative clinical assessment, operative/postoperative monitoring tools, and procedural precautions are discussed. They conclude that pATPE is a rare but life-threatening complication that requires immediate intervention. Young age (<3 years) or the presence of some comorbid conditions such as asthma, history of prematurity, craniofacial malformations, Down syndrome and severe OSA may increase the risk of developing PE in children undergoing adenotonsillectomy. With prompt diagnosis and intervention, most pATPE patients can be treated without incident. Since PE develops in a matter of minutes after adenotonsillectomy, simply monitoring oxygen saturation using pulse oximetry in the operating room and in the post-anesthesia care unit usually identifies patients at risk and in need of in-patient hospitalization rather than ICU admission.
see page 551
ORIGINAL ARTICLES
Regulation of Lipocalin-2 oncogene and its impact on gene polymorphisms on breast cancer patients in Jeddah, Saudi Arabia
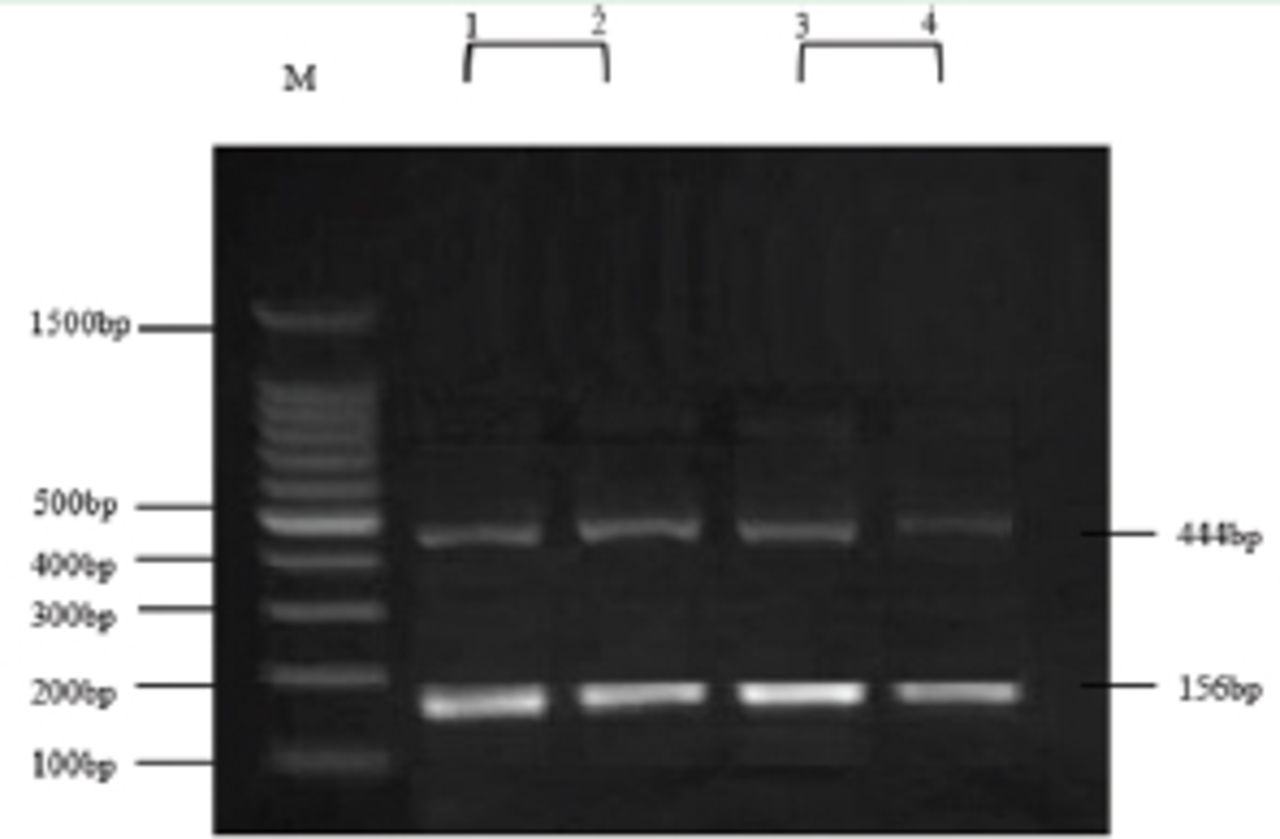
Linjawi et al identify the impact of Lipocalin-2 (LCN2) gene polymorphisms on breast cancer patients in western Saudi Arabia. The results have shown that 100% of the genotypes were normal allele (G/G). In contrast, the plasma level of LCN2 was considerably elevated among patients as compared to control (p=0.001), and higher in invasive ductal carcinoma patients (p=0.001). The LCN2 protein expression in plasma level was significantly elevated among patients, particularly who demonstrated invasive ductal carcinoma. They conclude that There is no significant relationship between breast cancer patients and LCN2 gene polymorphisms (rs11556770).

Genotypes for lipocalin-2 gene. Lane M: DNA marker. Lane 102: homozygous G/G normal gene type that produce double band of size 444 and 156bp (normal samples). Lane 3-4: homozygous G/G normal gene type that produce double band of size 444 and 156bp (breast cancer samples)
see page 558
Vascular endothelial growth factor and soluble vascular endothelial growth factor receptor-1 in patients with end-stage renal disease. Associations with laboratory findings, comorbidities, and medications
Erturk et al show the levels of vascular endothelial growth factor (VEGF), soluble vascular endothelial growth factor receptor-1 (sVEGFR-1) in patients with end-stage renal disease (ESRD) and to show the associations with clinical findings such as demographic features, laboratory findings, comorbidities, and medications. The VEGF level of ESRD group was not significantly higher (0.280±0.264) than the control group (0.321±0.210) (p=0.475). The sVEGFR-1 level of ESRD group was significantly higher (0.217±0.135) than the control group (0.068±0.047) (p<0.001). The correlation between VEGF and sVEGFR-1 was significant and negative (r=-0.246, p=0.036). Average VEGF level of ESRD patients using recombinant human erythropoietin (rhEPO) was significantly higher (0.567±0.28) than the ESRD patients not using rhEPO (0.246±0.24) (p=0.025).
see page 586
CASE REPORT
Neonatal subcutaneous fat necrosis with hypercalcemia treatment using calcitonin
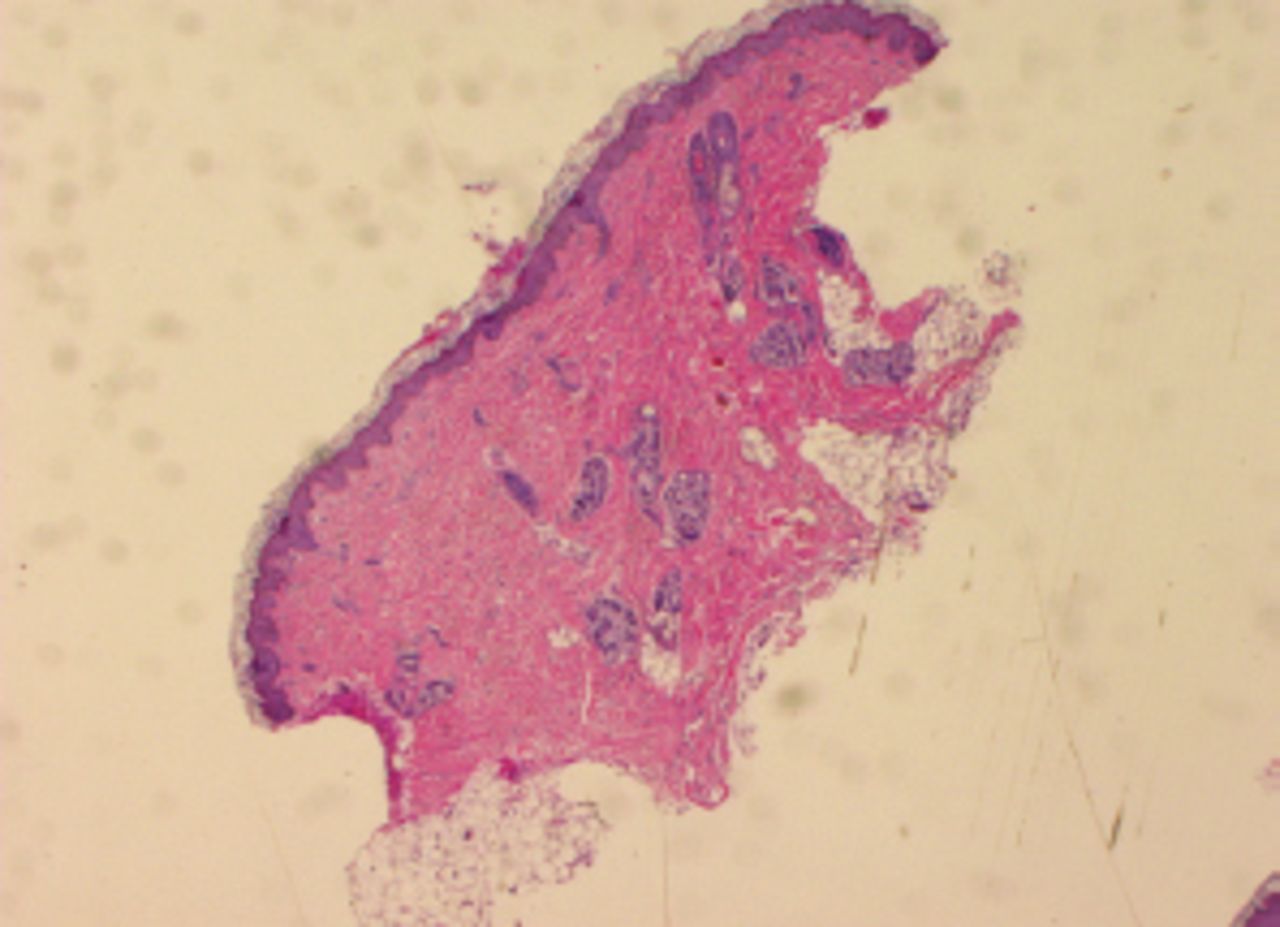
Alsofyani presents the case of a term infant who developed extensive subcutaneous fat necrosis in the first week of life after significant perinatal hypoxic injury. Her condition was complicated by hypercalcemia resistant to prolonged medical treatment with hyperhydration, diuretic and steroid but eventually the infant responded to high doses of calcitonin. The newborn was delivered after a complicated pregnancy due to maternal hypertension and oligohydramnios of unknown etiology. The umbilical cord was removed at a local polyclinic. The newborn was of an unknown birth weight and Apgar score.

Adipose tissue was mostly necrotic, exhibited residual viable foci, and contained swollen adipocytes with intracellular radial eosinophilic crystals (40 X magnification used with hematoxylin and eosin (H&E) stain)
see page 622
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.