


Clinical Presentation
A 36-year-old man presented to Rheumatology Clinic complaining of bilateral knee pain for 4 years, aggravated by movement and relieved by rest. He used to take NSAID and analgesics. There was no joint swelling, no morning stiffness, or other joint involvement. Past medical history was unremarkable. Clinical examination showed swelling of the upper part of left tibia medially, which was slightly warm.
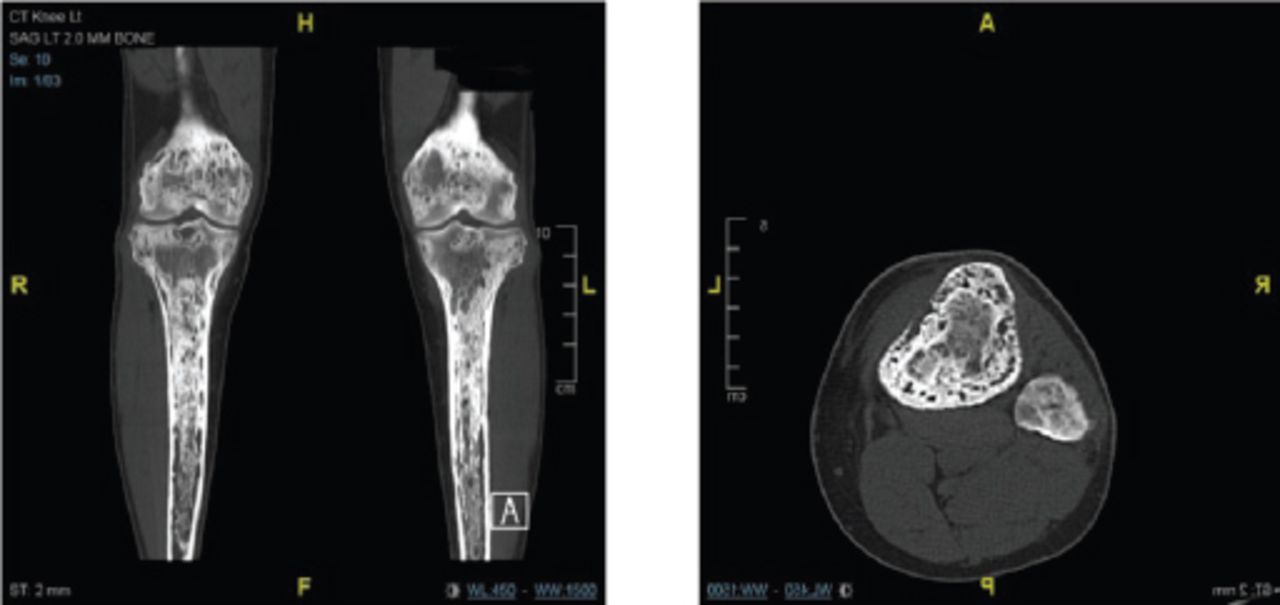
Laboratory investigations showed slightly elevated ESR=34, and slightly elevated platelets=597. CBC, LFT, urea and creatinine RF, Anti-CCP, ANA, ANCA were all negative. The patient had x-ray of the knees, tibias (Figure 1 A & 1B) and humerus (Figure 1C & 1D). It showed bilateral mottling and heterogeneous texture of the visualized bones. The rest of skeletal survey including pelvis and skull was normal. Computed tomography (CT scan) of the left knee and legs showed extensive intramedullary sclerosis with thick trabiculation associated with a spare areas at the metaepiphysis around the knee joints (Figure 2). He had bone technetium scan (TC-99), there is intense symmetrical radiotracer uptake seen involving the distal 2/3rd of both femoral bones, whole tibial bones, mid segment of humeral shafts, both ulnar and radial bones as well as tarsal bones bilaterally. There is also uptake in the right clavicle, mandible and maxilla (upper alveolar margin) (Figure 3).
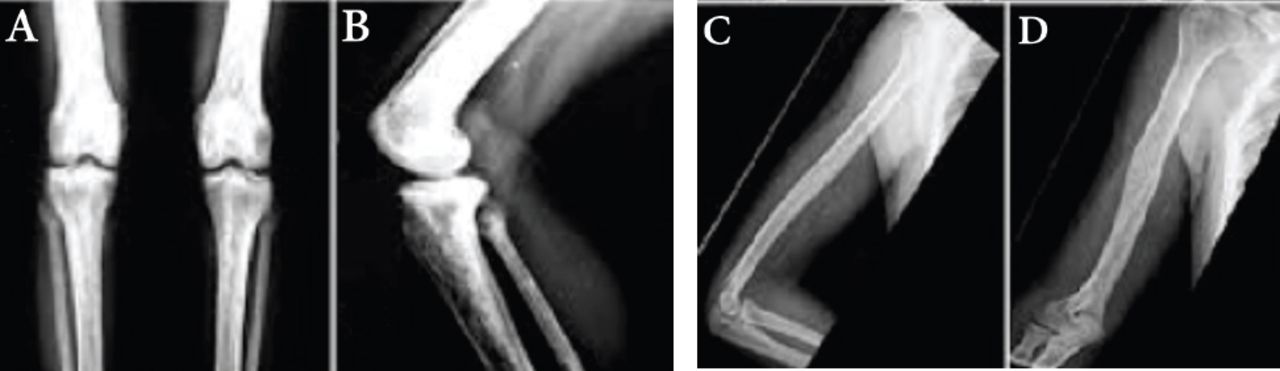
X-ray of the knees, tibias (a,b) and Humerus (c,d) showed bilateral mottling and heterogeneous texture of the visualized bones.

CT of the knee and legs showed extensive intramedullary sclerosis with thick trabiculation associated with a spare areas at the metaepiphysis around the knee joints.

Bilateral symmetrical intense radiotracer uptake of the long bones.
Question
1. What is the differentiated diagnosis?
Answers
Paget’s disease
Gaucher’s disease
Erdhiem - Chester disease
The patient underwent bone biopsy from the left upper tibia (Figure 4).
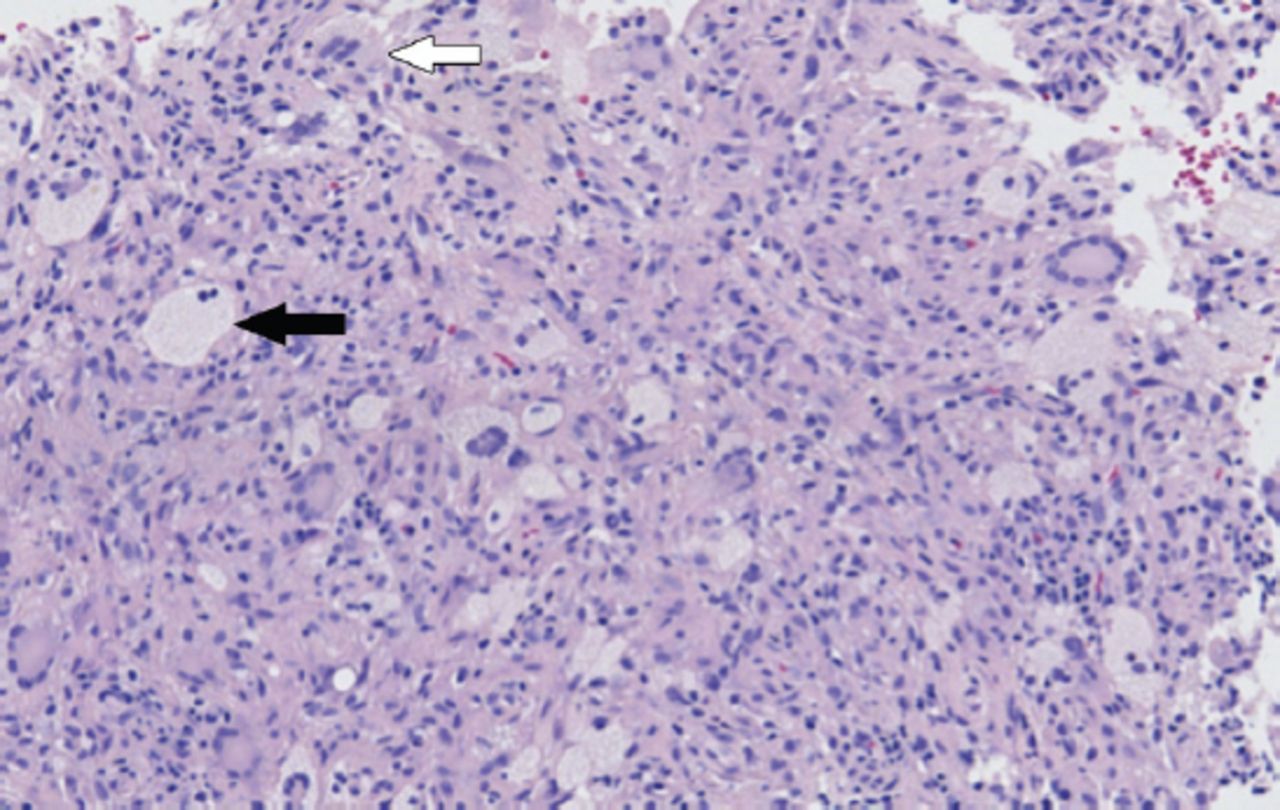
Diffuse infiltration by foamy histiocytes (Black arrow) and fibrosis and rare Touton-like giant cells (white arrow).
Question
What is the diagnosis?
Answer
Erdhiem - Chester disease
Erdheim-Chester disease
Erdheim-Chester disease (ECD) is a rare form of a non-langerhans histiocytic disorder. Originally, it was known as “Lipid Granulomatosis” by Jakob Erdheim in 1930.1 It is a multifocal disorder characterized by osteosclerotic lesions affecting the long bones.
Erdheim-Chester disease has numerous signs and symptoms. The symptoms are mainly due to skeletal involvement that occurs in 96% of patients. Bone pain is the most common consequence of skeletal involvement. It usually manifests around the knees and ankles. However, it occurs in only about 50% of cases.2 The bones more commonly affected are the femur, tibia, and fibula and less commonly the ulna, radius, and humerus. The differential diagnosis (DDx) includes, Paget’s disease, osteomyelitis, and lymphoma.
Moreover, ECD may progress to the central nervous system (CNS) and its adjacent structures. Central nervous system involvement is seen in 51% of patients and is responsible for 29% of deaths. Central diabetes insipidus is the most common manifestation of CNS involvement in ECD. Exophthalmos, cerebellar ataxia, and panhypopituitarism may also occur. The DDx is mainly Langerhans cell histiocytosis. Erdheim-Chester disease may progress to involve the cardiovascular system leading to congestive heart failure, myocardial infarction, and thromboembolism among others. Also, periaortic fibrosis is the most common cardiovascular lesion. The DDx of cardiac involvement in ECD is a cardiac myxoma. Pulmonary involvement associated with ECD occurs in 43% of patients. It can be diagnosed by detecting typical histiocyets in the lung. Due to the fact that ECD is a known cause of interstitial lung disease, radiological hallmarks of interstitial lung disease is highly likely to be ECD. The DDx of pulmonary involvement in ECD includes, interstitial pneumonia and pulmonary Langerhans’ cell histiocytosis.
ECD may involve the retroperitoneal space. However, it is mainly asymptomatic involvement. The DDx includes idiopathic retroperitoneal fibrosis (Ormond’s disease).
Moreover, a number of general symptoms may be associated with ECD. They include, fever, weight loss, weakness, and night sweats. The histological appearance typically seen in ECD is CD68(+), CD1a(−), S-100(−/low) non langerhans cell histiocytes. Also, ECD lesions of a pulmonary origin are positive for factor XIIIa. Microscopically, xanthogranulomatosis, proliferating fibroblasts, lack of eosinophils, lymphocytic aggregates and Touton giant cells are noticed. The diagnosis of ECD depends on histological and radiological criteria. The histological criterion is the most important to diagnose ECD and are sufficient to confirm the diagnosis. The imaging studies used to diagnose ECD are radiographs and Tc-99m MDP Bone Scintigraphy. The radiographs will demonstrate bilateral symmetric osteosclerotic lesions, whereas Tc-99m MDP Bone Scintigraphy show abnormally strong labeling of the distal ends of the long bones.
Due to the rarity of the disease, no treatment plan is universally accepted. One of the widely used drugs is systemic corticosteroids. They are used to control the symptoms; however, they are only transiently effective. Also, interferon-a successfully stabilizes the disease in the majority of cases.3 The adverse effects of interferon- a include asthenia, pruritis, myalgia, and thrombocytopenia. An alternative to interferon-a is Peginterferon alfa-2a. Chemotherapy only provided temporary relief. Also, if the lesions grew rapidly, then surgical debulking may be attempted. All in all, treatment is mainly dependent on the stabilization of the disease.
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.