


Abstract
Objectives: To perform a meta-analysis for celiac diseases (CD) among at-risk populations in Kingdom of Saudi Arabia (KSA), as well as a comparison with our previously reported meta-analysis in the normal population.
Methods: In March 2018, at King Abdulaziz University, Jeddah, KSA we commenced a retrospective comprehensive database and journal search for CD among at-risk populations in SA. Data from each of the relevant articles were analyzed using the Statistical Package for Social Science Version 20 (Armonk, NY: IBM Corp.). and the comprehensive meta-analysis program (CMA). The collected data were part of a retrospective literature review and analysis. Thus, a written ethical approval was not obtained before commencing the study.
Results: Sixteen articles were found covering type-1 diabetes mellitus (DM), short stature (SS), and down syndrome (DS). Ages 1-50 years. The prevalence of seropositive-CD was 15.6% with high heterogeneity (I2=80.353), while prevalence of biopsy-proven CD was 10.6% with high heterogeneity (I2=73.359). Another article reported the CD prevalence in the at-risk population as 18.4% for the seroprevalence and 6.9% for the biopsy-proven CD. Anti-transglutaminase (anti-tTG) was used in 12 studies; in the remaining 4 studies (EMA in 2, ARA with AGA in one and no details given in one study).
Conclusion: Both the prevalence of biopsy-proven CD (10.6%) and seroprevalence (15.6%) were higher than those we previously reported in the normal population (1.4% and 2.7%). The female-to-male ratio (1.9/1) of CD patients was the same in normal and at-risk populations in SA. Meta-analysis for prevalence of CD in DM, SS, and DS separately in SA is recommended.
Celiac disease (CD) is not uncommon in the Kingdom of Saudi Arabia (KSA), with prevalences (in normal populations) of biopsy-proven CD of 1.4% and seroprevalence of 2.7%.1 People at risk for CD include both genders, of any age or race, having a biological relative with CD, having HLA-DQ2 and HLA-DQ8 genes, having some autoimmune diseases or having CD-associated symptoms.2 The global prevalence of CD among at-risk groups is 5% to 10%, which include Down and Turner syndromes, type 1 diabetes, and autoimmune thyroid disease.3 In USA, the prevalence of CD was found to be 2.6% in second-degree relatives and 4.5% in first-degree relatives, with a similar profile in Europe.4 Short stature (SS) has also been identified among the at-risk group for CD. Globally, CD in SS ranges from 0.05-59.1% depending on the region of the study.5,6 In KSA, one article reported the prevalence of CD in the at-risk population as 6.9% for the biopsy-proven CD and 18.4% for the seroprevalence.7 The inclusion criteria in that study included chronic diarrhea, abdominal pain or/and T1DM, thyroid disease, failure to thrive (FTT), SS, anemia, and associated neurological diseases; for which the celiac profile was routinely requested. Additionally, 16 articles8-23 were found to be concerned specifically with certain at-risk status: T1DM,8-15 SS16-20 and Down syndrome.21-23 The aim of this study is to perform a meta-analysis for CD among at-risk populations in KSA, as well as a comparison with our previously reported meta-analysis in the normal population.
Methods
Strategy for systematic search and study selection
We retrospectively conducted our systematic review study at King Abdulaziz University, Jeddah, KSA between week 3 of March 2018. A comprehensive database and journal search was used according to the following keywords: “celiac disease in Saudi Arabia”, “celiac disease in Saudi children” and “prevalence of celiac disease in Saudi Arabia”, followed by a selection process (inclusion/exclusion for the pertinent studies), which was described in detailed in our previous systematic review.24 The pooled studies were retrieved via PubMed (US National Library of Medicine, with no specific period), Ovid, EBSCO, and Scholar Google. Few additional related articles were obtained through the library of King Fahd Research Centre, King Abdulaziz University, and directly from the editorial department of the 2 local journals: Saudi Journal of Internal Medicine and Journal of King Abdulaziz University Medical Science. Checking for duplication was carried out between articles via their titles, author(s) and year of publication. Then, 2 selection processes were followed: after matching for duplication, articles that were concerned with CD in KSA were selected (first selection), and their data were recorded using the Statistical Package for Social Science Version 20 (Armonk, NY: IBM Corp.). Articles that are concerned with the at-risk group (T1DM), Down syndrome (DS) and short stature (SS)] were further selected (second selection) and kept as a separate SPSS file that was used in this study.
Statistical analysis
Data was performed by SPSS (Armonk, NY: IBM Corp.); and by the Comprehensive Meta-analysis program (CMA) (Biostat, USA, Version 3). I squared (I2) was used to evaluate heterogeneity. I squared values of 0% denotes no heterogeneity, 25% denotes low heterogeneity, 25%-49% denotes moderate heterogeneity and >50% denotes high heterogeneity.25 The results were illustrated in tabulated form, diagrams, and figures.
Results
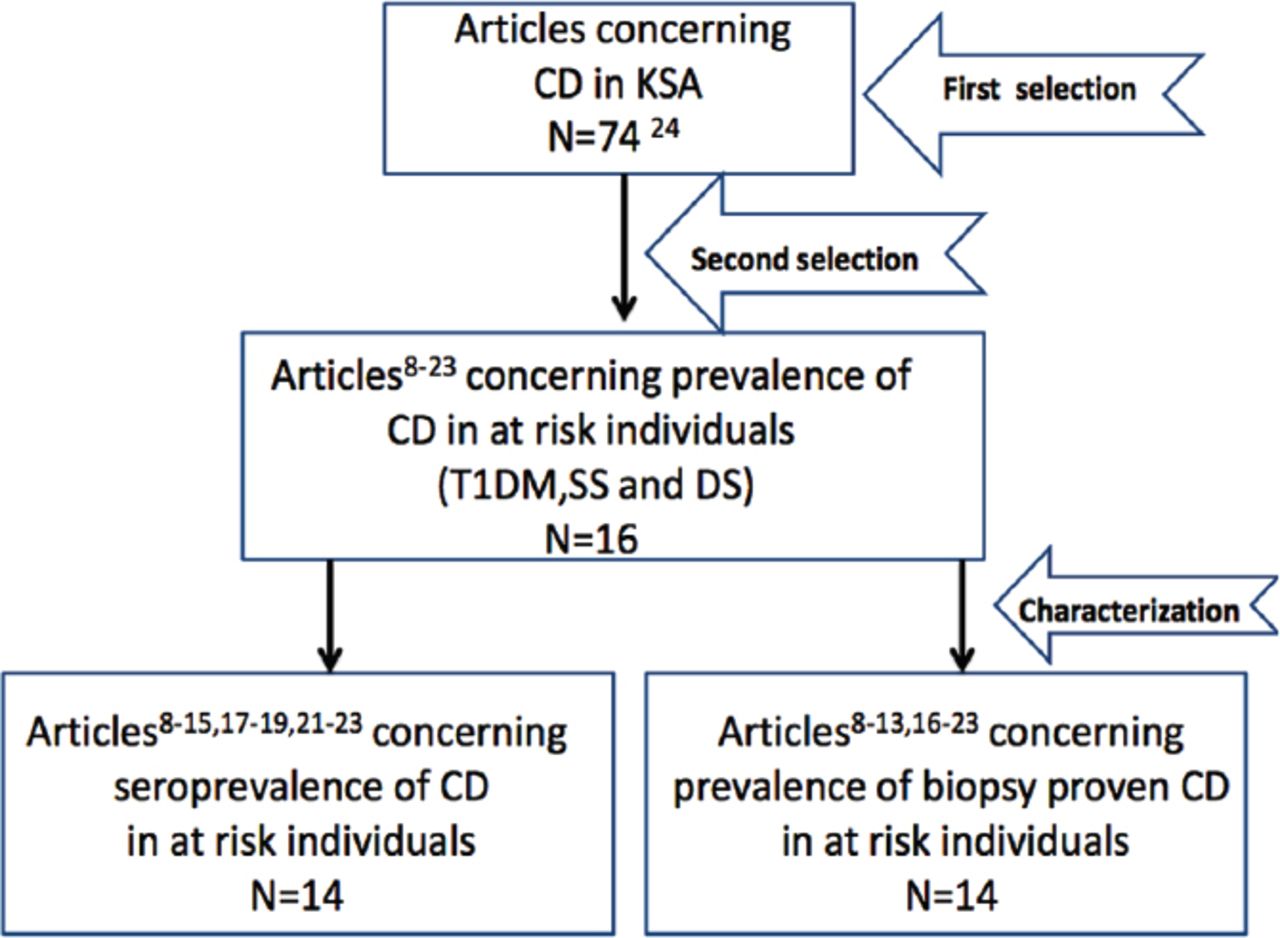
Selection and characterization of the pertinent studies (Figure 1 & Table 1)

PRISMA flow-diagram showing the selection process of the pertinent studies. CD- celiac diseases, KSA - Kingdom of Saudi Arabia, T1DM - type 1 diabetes mellitus, SS - short stature, DS - Down syndrome
Characterization of the identified studies on prevalence of celiac disease (CD) in Saudi Arabia.
Seventy-four articles were retrieved (following the matching for duplication and the first selection process) that were concerned with CD in KSA, from which we obtained 16 articles (second selection) concerning CD in at-risk individuals (Figure 1), that are arranged according to the type of the disorder. The data from these studies were recorded using the SPSS Version 20. Characterization of these studies is shown in Table 1. These studies covered a wide range of ages (1-50 years) and different age groups (Table 1): children and adolescents (10 articles); children and adolescents and adults (4 articles); children (one article); no mention (one article). These studies covered 3 regions in KSA (Table 1): Riyadh (8 articles), the western region (6 articles) and Southern region (2 articles). Table 1 also illustrates the different cohorts and prevalence for both seropositivity and biopsy-proven conditions.
Table 2 describes the total cohorts, the total number of positivity and rates for both seropositivity and biopsy-proven positivity. The seropositivity total cohort was 2169 (range: 51-430), with a total positivity of 306 and positivity rate of 14.1% (Table 2), while the biopsy-proven total cohort was 1919 (range was 51-430), with a total positivity of 179 and positivity rate of 9.3%. Table 2 shows higher rates by meta-analysis (Tables 3 & 4) for both seropositivity (15.6%) and biopsy-proven positivity (10.6%).
Rate of celiac disease in at-risk population; a comparison between the results of the traditional statistical analysis and meta-analysis.
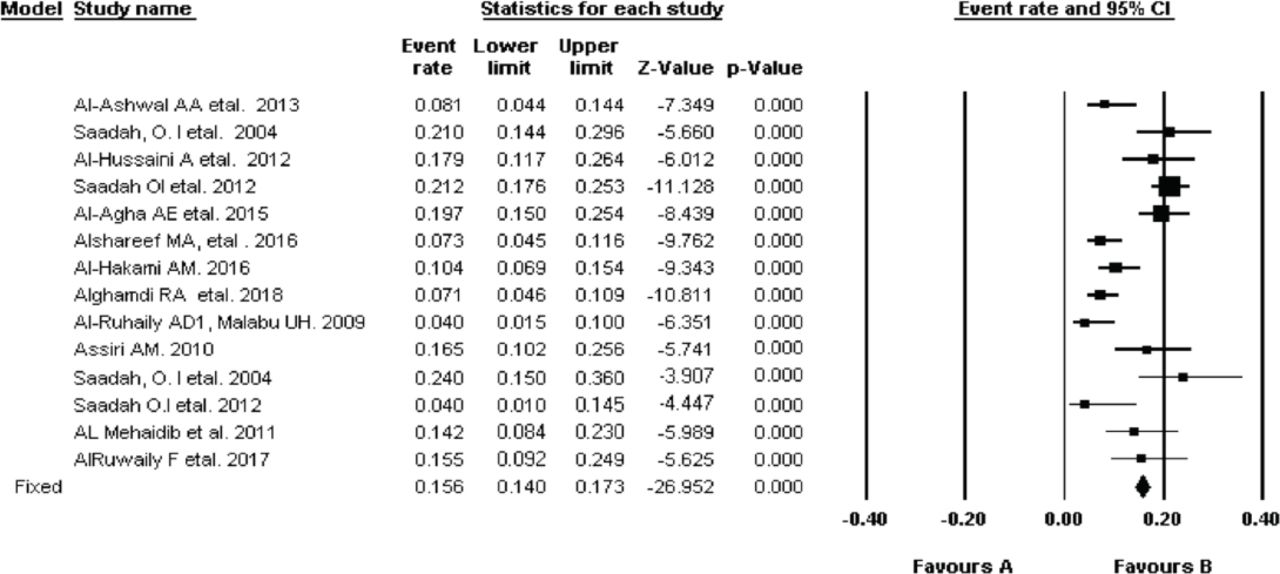
Seropositivity prevalence (by fixed and random models) with the heterogeneity between studies.
Prevalence of biopsy-proven positivity (by fixed and random models) with the heterogeneity between studies.
Meta-analysis
Meta-analysis was performed using the Comprehensive Meta-analysis program (CMA). Meta analysis was performed for the 14 articles concerning seroprevalence of CD in at risk individuals [articles 8-15,17-19,21-23], and for the 14 articles concerning prevalence of biopsy-proven CD in at-risk individuals [articles 8-13,16-23]. The meta-analysis of seropositivity prevalence (Tables 3 & 5; and Figure 2 & 3) showed that CD prevalence (by fixed model) for serologically-proven CD (one serology at least) was 15.6% (95% CI = 14-17.3) with high heterogeneity (I2 = 80.353). While meta-analysis for prevalence of biopsy-proven positivity (for 14 articles, by fixed model) (Tables 4 & 6, Figures 4 & 5) was 10.6% (95% CI=9.5-12.5) with high heterogeneity (I2 = 73.459).
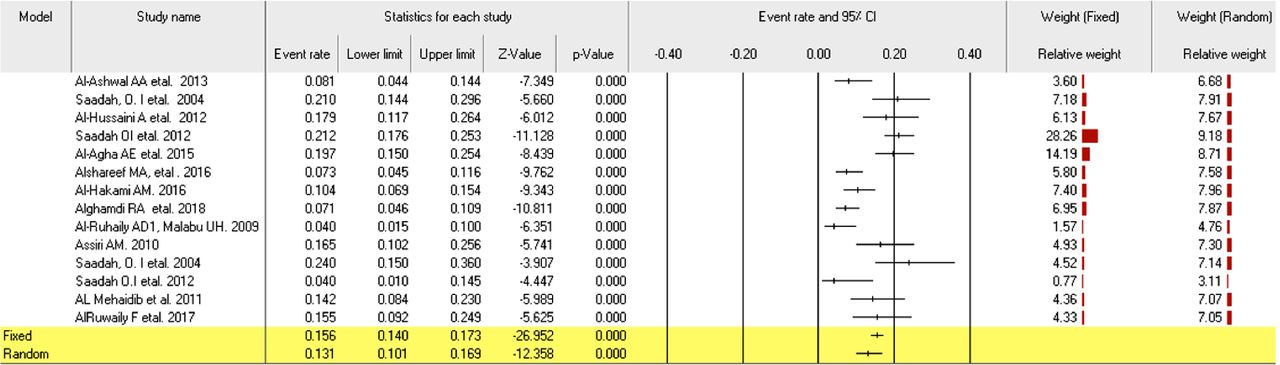
Data for meta-analysis of the seropositivity prevalence.

Seropositivity prevalence (by fixed and random models) with statistics and relative weight for each study.

Prevalence of biopsy-proven positivity (by fixed and random models) with the heterogeneity between studies.
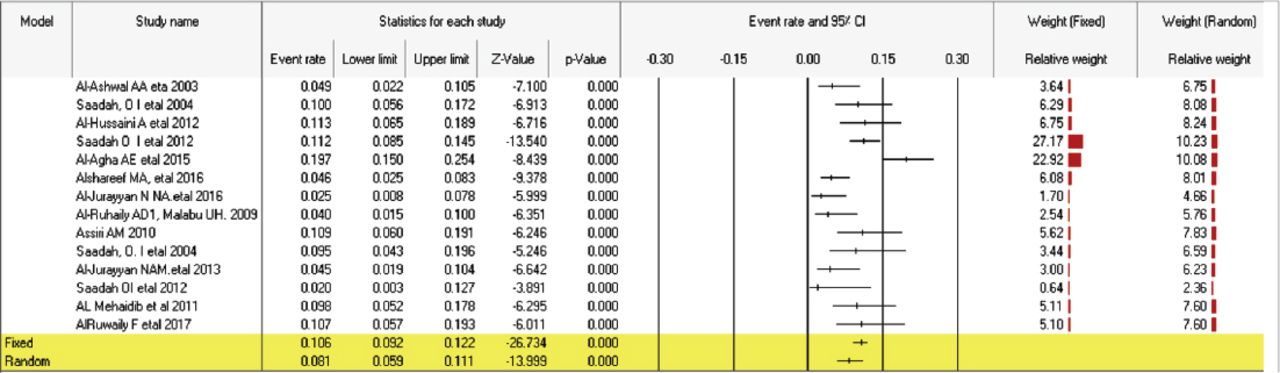
Data for meta-analysis of the biopsy-proven positivity.

Prevalence of biopsy-proven celiac diseases (by fixed and random models) with statistics and relative weight for each study.
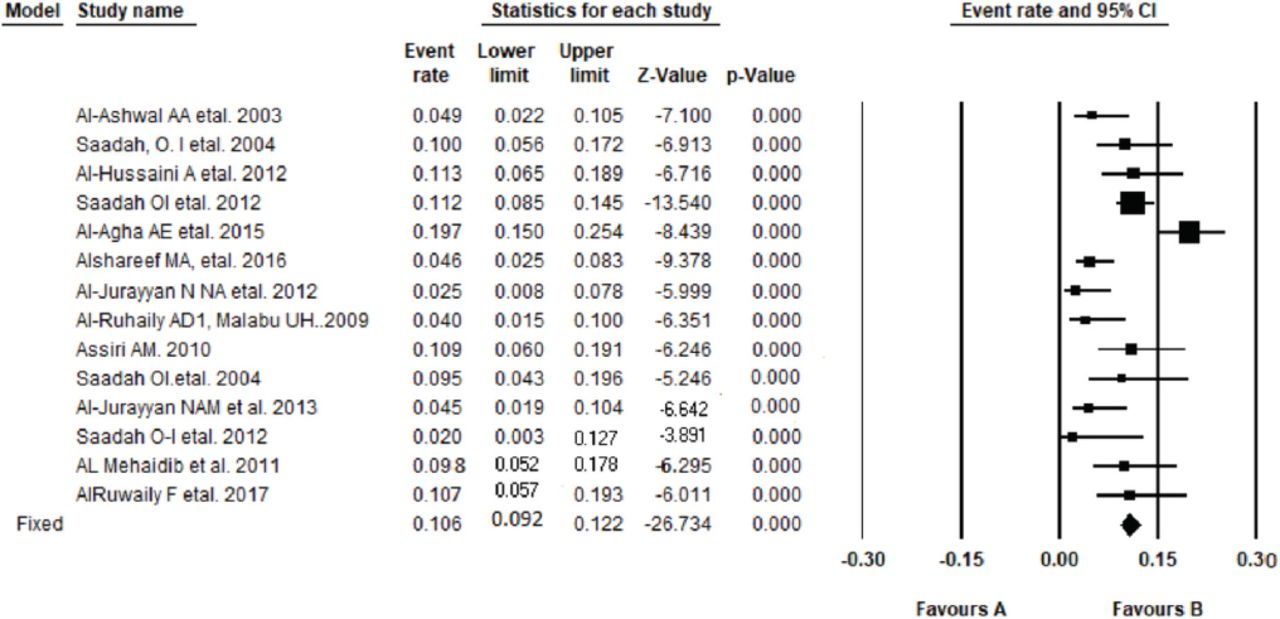
Forest plot of the meta-analysis for prevalence of biopsy-proven celiac diseases.
Other studies concerning autoimmune diseases versus CD in KSA
Five articles26-30 concerning autoimmune diseases were not included in the at-risk group of this study. This included two animal studies, two studies of one case each and one study of 42 children (24 females; age range between 5-15 years) with juvenile rheumatoid arthritis (JRA). In the latter study, the seroprevalence of CD was 42.8% (18/42), while the prevalence of biopsy-proven CD was 2.3% (1/42).
Female to male ratio
Gender information was found in 10 articles (Table 7). The ratio of the total female (120) over the total male (58) was 2/1 (Tables 7 & 8). Regarding the regions, the western region showed the highest F/M ratio (24/8 = 3/1) followed by the southern region (35/16 = 2.1/1) and Riyadh (61/34 = 1.8/1) (Table 8).
Pattern of serology and biopsy in the identified studies on prevalence of at-risk individuals for celiac disease (CD) in Saudi Arabia.
Conditions of the celiac disease at-risk studies and their distribution according to regions in Saudi Arabia.
Duration span
The included 16 studies were published between 2004 and 2018, covering a long period from 1990 until 2014, with 5 retrospective studies without year limitation.9-11,19,22
The pattern of serology and biopsy
In the 16 included studies, anti-tTG was used in 12 studies (anti-tTG alone in 5 studies; with EMA in 3; with AGA in one; with EMA and AGA in 2; with EMA and AGA and ARA in one), and biopsy was used in 14 studies. Without anti-tTG: EMA was used in 2 studies: ARA with AGA (one study) and one study without details (Table 7).
Conditions of the CD at-risk studies and their distribution according to regions in KSA
The 16 studies are related to 3 regions (Riyadh, western and southern). Riyadh showed the highest at-risk studies (8 studies) followed by the western region (6 studies) and southern region (2 studies) (Table 8). Riyadh had the most studies for SS and DS (4 out of 5 studies for SS and 2 out of 3 for DS), followed by the western region (one out of 5 for SS and one out of 3 for DS), while the western region showed the highest for T1DM studies (4 out of 8 studies) followed by Riyadh and the southern region (2 studies each).
Prevalence of CD in different at-risk conditions (T1DM, DS, SS) in KSA
The reported biopsy-proven prevalence showed considerable range variations among studies of the 3 conditions: 7.6-19.7% for DM, 2-10.7% for DS, and 2.5-10.9% for SS (Table 9). However, the calculated biopsy-proven prevalence of CD was highest in DM (10.8 [132/1215]), followed by DS (8.4% [19/226]) and lowest in SS (5.85 [28/478]).
Rate of celiac disease in different at-risk populations (total at-risk, type1 diabetes mellitus (DM1), short stature(SS) and Down syndrome (DS).
Discussion
Celiac disease is more common in at-risk people, such as having a biological relative with CD, having HLA-DQ2 and HLA-DQ8 genes, having CD symptoms or having some autoimmune diseases.2 For genetic-based CD, there is an increased risk (3-6%) for developing CD among those with a relative having CD2. Likewise, having HLA-DQ2 and HLA-DQ8 haplotypes is associated with increased risk for developing CD, while their absence excludes the possibility of CD31. Globally, approximately 95% of people with CD have the HLA-DQ2 gene, and most of the remaining 5% have the HLA-DQ8 gene.2 However, it is reported that HLA-DQ2 and HLA-DQ8 were present in 98.6% of patients with CD, and in 40% of the global general population who were without a diagnosis of CD.32 However, HLA-DQ in KSA has been recently reported to be one of the highest frequencies (52.7%) among healthy general populations worldwide.33 Having the HLA-DQ gene indicates that the person is at risk for developing CD, but does not indicate a definite CD; thus, a positive HLA-DQ test should be followed by CD profile tests (blood and histology) for the determination of presence or absence of CD.34
Screening of CD is becoming increasingly common in first-degree relatives and patients with T1DM.35,36 The presence of an autoimmune disease (such as CD) increases the likelihood of developing other autoimmune diseases, such as T1DM,37,38 autoimmune thyroid disease,39,40 autoimmune hepatitis41 and DS;42 thus, these conditions, in addition to first-degree relatives, are usually termed as high-prevalence or at-risk groups, in which screening of CD (in contrast to the general population) is considered to have a favourable cost-benefit ratio.43 The current study represents the first and only meta-analysis concerning the prevalence of CD in at-risk individuals in KSA. This meta-analysis included more than 2000 at-risk individuals from 16 studies in KSA. The 16 articles were covering the at-risk population (T1DM, SS and DSe). Two articles of them were without endoscopy results, and the other 2 only showed the biopsy-confirmed results. Thus, both seroprevalence CD and prevalence of biopsy-confirmed CD were calculated in 14 articles each. By meta-analysis, the prevalence of biopsy-proven CD (10.6%) and seroprevalence (15.6%) were both high, with high heterogeneity (I2 = 73.459 and I2 = 80.353); while with a traditional statistics approach by SPSS analysis, 14.1% had seropositivity and 9.3% had biopsy-proven CD. Meta-analysis allows a more objective appraisal than the traditional statistical analysis, since it takes into account the relative weight of each involved study and, thus, provides a more precise estimate, in addition to the heterogeneity between the results of individual studies.44 The global prevalence of CD among at-risk groups (Down and Turner syndromes, type 1 diabetes, and autoimmune thyroid disease) have been reported to range from 5% to 10%.3 In KSA, one article reported the prevalence in the at-risk population as 18.4% and 6.9% for the seroprevalence and biopsy-proven CD respectively.7
Other articles 26-30 were found concerning autoimmune diseases. These articles include two animal studies, in addition to one case study (2 articles). One study addressed 42 children (24 females; age ranged between 5–15 years) with juvenile rheumatoid arthritis (JRA). The latter study showed a considerable difference between seroprevalence of CD (42.8%) and the prevalence of biopsy-proven CD (2.3%) and was not involved in the current meta-analysis. In comparison with the CD prevalence in normal populations in KSA,1 both the prevalence of biopsy-proven CD (10.6%) and seroprevalence (15.6%) were higher than that in the normal population (1.4% and 2.7%). Similar to the normal population1 the total number of the CD females among the at-risk population was twice as much as the CD males (1.9/1). The reported prevalence in the current study showed that biopsy-proven prevalence of CD was highest in DM (10.8 [132/1215]), followed by DS (8.4% [19/226]) and lowest in SS (5.85 [28/478]); this is in contrast to the report of Costa Gomes et al42 from Brazil that biopsy-proven CD prevalence in DS is almost three-times higher than that in DM [DM1=5/111 (4.5%), DS=10/77 (13.0%)].
One limitation is the absence of uniform performance of small intestine biopsies in seropositive patients, as (in seven studies) 51 out of 134 seropositive patients (38%) refused endoscopy; another limitation is the lack of gender ratio in some studies.
In conclusion, concerning CD in at-risk individuals in KSA, both the prevalence of biopsy-proven CD (10.6%) and seroprevalence (15.6%) were high, with high heterogeneity (I2 = 73.459 and I2 =90.353) between studies; and both are higher than those in the normal population (1.4% and 2.7%). The female-to-male ratio (1.9/1) of CD patients was the same in the normal and at-risk populations in KSA.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}