


Abstract
Objectives: To raise awareness of practitioners on benign treatable conditions such as pancreatic tuberculosis (TB).
Methods: A retrospective study at King Khaled University Hospital, Riyadh, Saudi Arabia of all patient charts presented with pancreatic mass for a period of 10 years (2007-2017) with a study duration of 4 years between 2013 and 2017. Patients with confirmed diagnosis of pancreatic cancer were excluded. A written ethical approval was obtained accordingly.
Results: All adult patient charts were retrospectively reviewed with a pancreatic mass for a period of 10 years (2007-2017). Nine patients were identified with proven diagnosis of TB. The data were obtained based on demographic features, sign and symptoms, duration of illness, imaging, ultrasound, contrast enhanced computed tomography scan, cytology or histopathology, polymerase chain reaction, culture and follow up with anti-tuberculous therapy and samples for cytology or histology. The histological findings of granuloma with caseation or positive culture were used confirming the diagnosis of TB. All patients were immunocompetent and screened for human immunodeficiency viruses before starting anti-TB treatment. Results were negative. All patients who underwent fine needle aspiration (FNA) and endoscopic ultrasound (EUS) for suspicious pancreatic mass were provided trial of antibiotics as cases of pancreatic tuberculosis showed dramatic improvement during follow up and cured from the disease.
Conclusion: The EUS and FNA are good tools to confirm malignancy and rule out benign treatable conditions like TB for any patient with a pancreatic mass suspicious for carcinoma.
Tuberculosis (TB) is a health problem arising mostly in immunocompromised individuals. There has been an elevated progression of cases reported in immunocompetent patients, more typical in developing countries.1
Pancreatic TB is extremely a rare infection and usually present clinically and radiologically similar to pancreatic adenocarcinoma. Furthermore, the actual transmission of the virus to the pancreas is yet unknown, but there are several approaches that have been proposed. It can be via blood-borne or lymphatic spreading from an occult lesion or invasion from contiguous lymph nodes or from an occult focus in the lungs.1 The practice of using endoscopic ultrasound (EUS), histology and cytology evaluation of pancreatic lesions are an advantage to classify pancreatic TB, preventing repeated surgical interventions with major morbidity and mortality.
The aim of this study is to Raise awareness of practitioners about benign treatable conditions such as Pancreatic Tuberculosis.
Methods
A retrospective review on charts of all pancreatic mass patients presented at King Khaled University Hospital, Riyadh, Saudi Arabia for over 10 years (2007-2017) with a study duration of 4 years from 2013 to 2017. Nine patients were found positive of TB. Demographic information, abnormalities, illness duration, diagnostic tests (chest x-ray, ultrasound [US], contrast enhanced computed tomography [CT] scan), cytology or histopathology, PCR (polymerase chain reaction), culture and intervention data on anti-TB therapy were gathered. Cytological or histological specimen results had been collected through US guided fine needle aspiration (FNA). Diagnosis of TB had been confirmed based on the histopathological results of granuloma with caseation or positive culture. All patients are immunocompetent (human immunodeficiency viruses [HIV] screened, before starting anti-TB treatment, and results were negative). The references search method was conducted through online browsing. The study is in accordance with Helsinki Declaration. Ethical approval was obtained
Case Report
Case 1
A 44-year-old Saudi male, known case of hyperlipidemia, presented with a 2-year history of fever, night sweats, abdominal pain and lethargy. Physical examination was unremarkable. Chest x-ray was normal. Computed tomography scan of the abdomen showed multiloculated cystic lesion at the tail of pancreas with multiple mediastinal lymph nodes. Endoscopic ultrasound and FNA were performed and showed necrotizing granulomatous inflammation.
Case 2
A 53-year-old Saudi male came with a one year history of upper abdominal pain, anorexia and weight loss. He had a history of hemoptysis. Physical examination was unremarkable. Chest x-ray showed multiple nodules. Computed tomography abdomen revealed a hypodense mass in the body of the pancreas with multiple enlarged lymph nodes, with 2 pulmonary nodules. Endoscopic ultrasound with FNA showed necrotizing granulomatous inflammation. Additional surgical biopsy was taken from a peritoneal nodule that showed granulomatous inflammation (disseminated TB).
Case 3
A 43-year-old Filipino male presented with nausea, vomiting and jaundice. Physical examination was unremarkable. Chest x-ray was normal. Ultrasound showed a dilated common bile duct. Endoscopic retrograde cholangiopancreatography (ERCP) was carired out and showed a bile duct with a stricture, a stent was inserted. Computed tomography abdomen showed multiple lymph nodes in porta hepatitis and peripancreatic area. Endoscopic ultrasound was performed and FNA from one of the peripancreatic lymph nodes revealed necrotizing granulomatous inflammation. Positive culture for TB (disseminated TB).
Case 4
A 21-year-old Saudi female admitted for abdominal pain, weight loss, vomiting, night sweats and fever for 2 months. She reported exposure to a TB patient 8 months before admission. On examination, there was tenderness in the epigastric area, with a small mass measuring 2x3 cm in the upper abdomen. The mass was tender, well defined, hard, and deep. Patient had no peripheral lymphadenopathy and no organomegaly. Chest x-ray was normal. Computed tomography scan of the abdomen showed peripancreatic hypodense cystic lesions. Endoscopic ultrasound and FNA was carried out and the biopsy showed necrotizing granulomatous inflammation and the PCR test came positive for TB.
Case 5
A 52-year-old Saudi female came with a 6 month history of upper abdominal pain associated with vomiting and weight loss. Physical examination was unremarkablea. Chest x-ray was normal. Computed tomography scan of the abdomen showed an ill-defined heterogeneous mass in the head and neck of pancreas invading the major vessels with multiple enlarged lymph nodes. The lesions were cystic in nature. Endoscopic ultrasound was carried out with FNA and did not show granulomas but mucin was positive. She was diagnosed as inoperable cystadenocarcinoma of pancreas. Tuberculosis culture came back later as positive.
Case 6
A 65-year-old Saudi female presented with abdominal pain for 3 years. On examination, a left cervical lymph nodes was palpable, tenderness in the epigastric area were noted. Chest x-ray was normal. Computed tomography scan showed a pancreatic head mass with multiple enlarged lymph nodes, and multiple mediastinal lymph nodes. Endoscopic ultrasound was carried out with FNA and showed necrotizing granulomatous inflammation (disseminated TB).
Case 7
A 15-year-old Saudi boy presented with fever, shortness of breath, abdominal pain and loss of weight. On examination, he had peripheral cyanosis and nail clubbing. Chest x-ray showed increased broncho-vesicular marking with prominent hilar shadows. Computed tomography chest revealed 2 small end vascular pulmonary nodules in the right upper and lower lobe, multiple mediastinal and hilar lymph nodes of variable sizes. Computed tomography abdomen revealed multiple abdominal lymph nodes in the gastro-splenic, porta hepatis, and near the pancreatic head with larger lymph node at the gastro-splenic area measuring approximately 4.7x4 cm. Endoscopic ultrasound with FNA showed multiple matted, large paraortic and celiac lymphadenopathy, suggestive of disseminated TB.
Case 8
A 59-year-old male, known case of chronic pancreatitis presented with recurrent abdominal pain, vomiting for one month and weight loss. On examination, abdomen was mildly tender in epigastric area, liver was palpable (liver span 14 cm), no splenomegaly or ascites. Chest x-ray showed fibroatelectatic changes in both lower zones. Computed tomography chest revealed bilateral lobe consolidation and left pleural effusion. Computed tomography abdomen scan showed a heterogeneous mass at the head of the pancreas with classification; and lymph nodes were noted at porta hepatis. Endoscopic ultrasound showed a solid mass with cystic component and FNA confirmed granulomatous inflammation.
Case 9
A 28-year-old Saudi male presented with a mass in peripancreatic area, discovered incidentally during pre-operative investigation of laparoscopic sleeve gastrectomy operation. He had abdominal pain only. Computed tomography chest, abdomen, pelvis showed upper abdominal and mediastinal lymphadenopathy along with peripancreatic homogeneously hypovascular soft tissue lesion residing in the gastrohepatic area, encasing the celiac trunk branches as well as main portal vein which was however patent. Endoscopic US was carried out with FNA from celiac lymph nodes showed necrotizing granulomatous lymphadenitis (disseminated TB).
The patients’ demographics, symptoms, radiological findings, culture and presence of extra pancreatic TB are summarized in Table 1.
Patient’s demographics, symptoms, radiological findings, culture, and presence of extra pancreatic tuberculosis.
Management and results. All patients underwent anti-TB treatment after discussion with infection diseases team and the aim was to treat according to the National Tuberculosis Control and Prevention Program (NTCPP) guidelines.
Case 1
Patient started for 6 months on isonicotinylhydrazide (INH), ethambutol, pyridoxine, pyrazinamide, vitamin (vit) B6. Had hyperlipidemia, on atorvastatin which has interaction with rifampicin. Other alternatives were used. Followed up in the clinic, showed improvement.
Case 2
Patient started on isoniazid, rifampicin, ethambutol, pyrazinamide, vit B6. Followed up in the clinic for 9 months with improvement, then follow-ups were missed.
Case 3
Patient started on rifampicin, INH, pyrazinamide, ethambutol, pyridoxine, followed up in the clinic, showed improvement.
Case 4
Patient started on rifampicin, INH, pyrazinamide, ethambutol, pyridoxine. Followed up in the clinic, and showed improvement.
Case 5
Developed anti-TB medication toxicity, after starting the drugs (isoniazid, ethambutol, pyrazinamid). She developed drug-induced hepatitis and treatment was suspended until liver function test had improved. The drugs were started gradually again, and aspartate aminotransferase (AST) levels were measured as follow-up. After 2 months, she complained of fatigue, postural dizziness, heat intolerance and significant weight loss. As a result, the aim was to decrease the dose of Isoniazid. After 4 months, she reported pain and burning sensation in her left side of the body from head to toe, headache and dizziness. A neurological examination showed hyper-reflexia bilaterally in her lower limbs and power of 4/5 bilaterally in all her body muscles, but no signs of meningeal irritation. Thus, rifampicin was added and isoniazid was stopped. Subsequently, she finished her treatment course with no major issues.
Case 6
Patient started on rifampicin, INH, pyrazinamide, ethambutol, pyridoxine, vit B6. Followed up in the clinic, showed improvement.
Case 7
Patient started on rifampicin, INH, pyrazinamide, ethambutol, pyridoxine, vit B6. Followed up in the clinic, showed improvement.
Case 8
Patient started on rifampicin, INH, pyrazinamide, ethambutol, pyridoxine, vit B6. Followed up in the clinic, and showed improvement.
Case 9
Ethambutol, Pyrazinamide, Rifampicin, INH, vit B6. Followed up in the clinic, showed improvement.
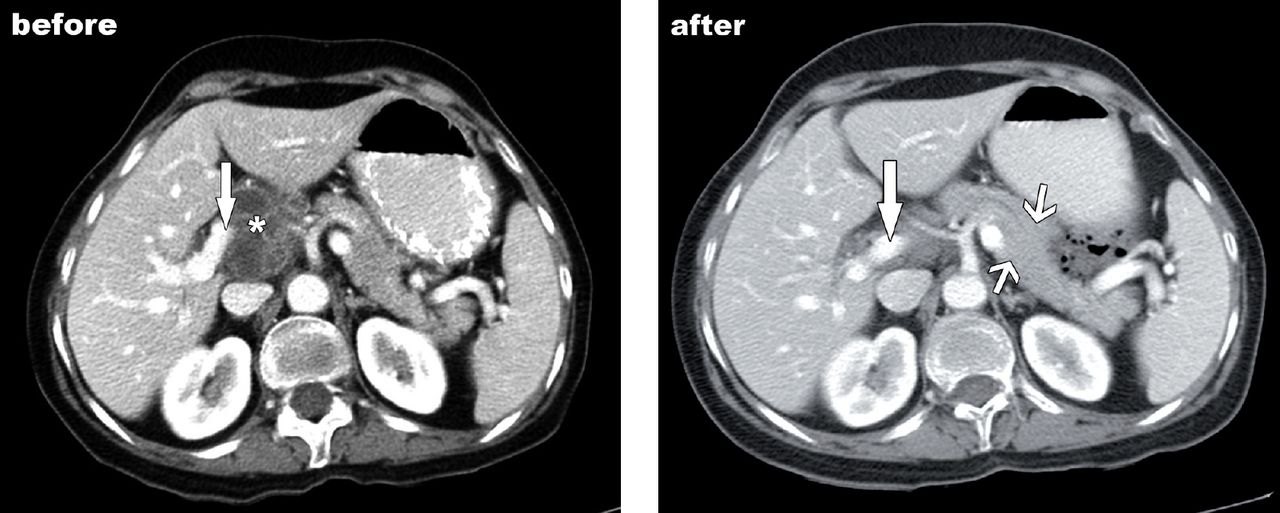
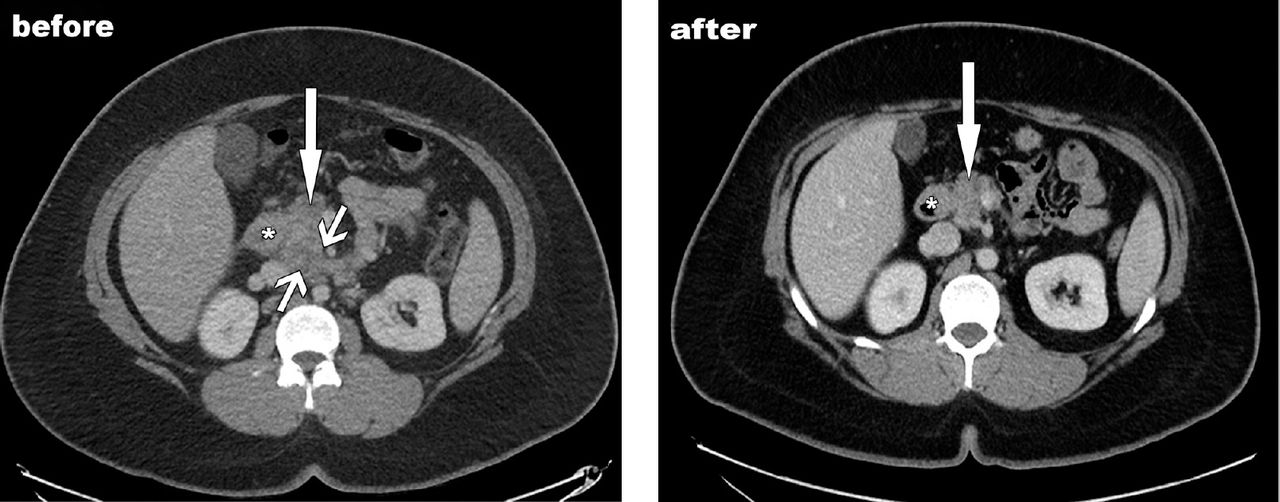
All patients fully improved without significant side effects (except case no. 5) and showed good responses physically, clinically and radiologically (cases 5 and 9, shown in Figures 1 & 2).
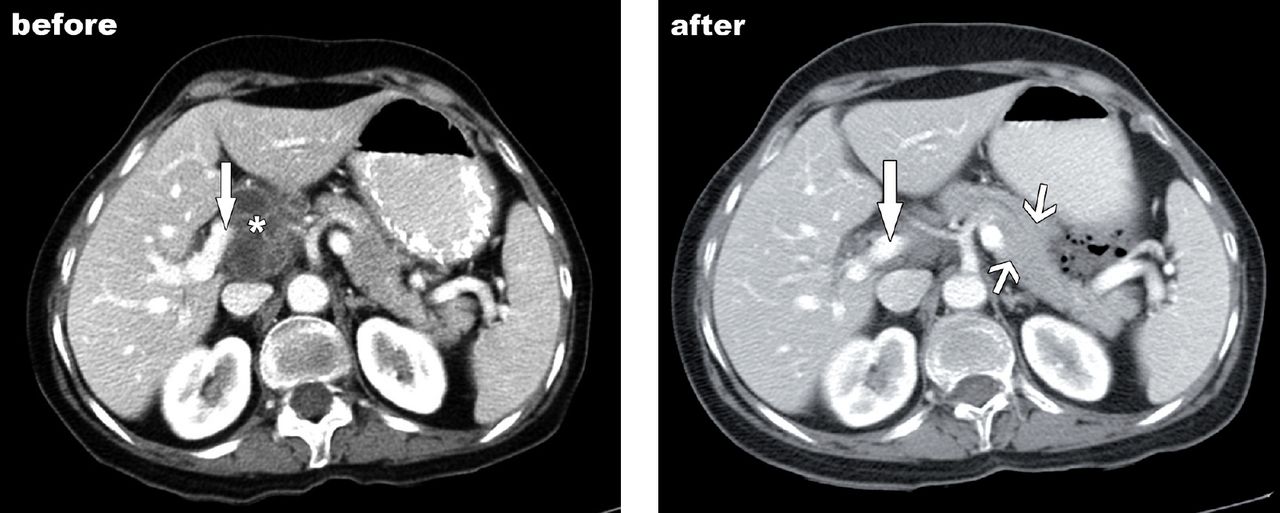
Computed tomography of case 5 A) before and B) after. The white arrows - portal vein, opposing arrow heads - pancreas, asterisk(*) - portahepatic cyst like mass (necrotic lymphadenopathy due to tuberculosis).

Computed tomography of case 9 A) before and B) after. asterisk (*) - duodenum, arrow - dead of pancreas, opposing arrow-heads - hypodense matted lymphadenopathy tuberculosis.
Discussion
In this series, patients presented with variable signs and symptoms indicating involvement of many organs and most importantly pancreas with TB. Pancreatic TB is a rare entity which seldom affects the pancreas alone and focal pancreatic involvement without TB elsewhere in an immunocompetent patient is more rare. In western countries, there were also reports of confirmed increased frequency of pancreatic TB. The identified number of such cases in immunocompetent patients increased over the past decade. The increased occurrence is possibly brought in by globalization, increased use of immunosuppressants, the global resurgence of mycobacterium TB and the HIV pandemic.2
The presentation of common clinical features of pancreatic TB were unclear. Symptoms such as epigastric pain, weight loss, and low-grade fever are non-specific symptoms, which usually rise to the possibility of an abdominal malignancy. Pancreatic adenocarcinoma is the leading diagnosis in most reported cases of TB of the pancreas. Early detection is very significant to prevent redundant diagnostic or therapeutic procedures, since pancreatic TB is usually treated medically with excellent results.3
Biopsies result from the mass showed high sensitivity of cultures 77% with antibiotic sensitivity but it can take up to 8 weeks to get the results, granulomas with or without caseation is sensitive in over 60% of cases and Ziehl-Neelsen stain is sensitive only in 50% of the cases.4
Fine needle aspiration cytology/biopsy is generally considered as a useful test and only few cases of pancreatic TB have been diagnosed by FNA cytology/biopsy. The percentage of success of the image guided percutaneous FNA cytology or biopsy in diagnosing pancreatic TB is less than 50%.2 Endoscopic US-FNA cytology/biopsy has proven to be an excellent tool for the cytological diagnosis of pancreatic and peri pancreatic masses. The diagnostic accuracy of EUS-FNA was reported to be 76% to 95% for pancreatic cancer and 46% for focal inflammation.2 Because of the rarity of pancreatic/peri pancreatic TB, the diagnostic accuracy of EUS-FNA for this condition is difficult to determine. In a recent randomized controlled study, comparing EUS-guided biopsy and CT- or US-guided biopsy for determination of pancreatic mass etiology, no statistical difference was found in terms of accuracy.5 There is no known negative impact of tumor cell seeding with EUS-guided FNA of cystic or solid pancreatic masses.2
In our series, we have questionable cases suspected to be isolated pancreatic TB, but we could not confirm it. Only 28 cases have been reported in the literature worldwide (1994).6 However, in a study from India between 1999-2004 detected pancreatic TB in 8.3% of the 384 patients who were diagnosed with abdominal TB.7 Also, a study by Chaudhary,8 encountered 5 cases of pancreatic TB in the last 10 years. Out of these 5 cases, pancreatic TB was a part of generalized disease.9 In 1941, Auerbach10 reported autopsy results of 1656 TB patients. Pancreas was involved in 14 cases (4.7%) as part of generalized TB but no isolated pancreatic TB cases were found.8 Bhansali11 did not report a single case of pancreatic TB in a series of 300 cases of abdominal tuberculosis.11 It was suggested that the pancreas is usually spared because of the presence of pancreatic enzymes, which interfere with the seeding of mycobacterium TB.12
Overall, the healthcare system in Saudi Arabia has improved dramatically and the government applied strict implementation of vaccination within the country. As such, physicians ruled out TB especially pancreatic in the differential diagnosis of any pancreatic mass.
In conclusion, in any patient presenting with a pancreatic mass suspicious for carcinoma, EUS and FNA are good tools to perform in order to confirm malignancy and rule out benign treatable conditions like TB.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Acknowledgment
The authors would like to thank Dr. Muteb Alkubaeer, Consultant, General Radiologist for attesting the clarity and correctness of the CT scan and Scribendi (www.scribendi.com) for editing the language
- Received May 19, 2019.
- Accepted August 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.