


Abstract
Objectives: To determine the impact of vitamin D deficiency and insufficiency on the development of anorexia in children with mild malnutrition without an obvious cause.
Methods: This cross-sectional study was conducted in Faruk Medical City, Sulaymaniyah, Kurdistan Region, Iraq, between May and September 2018. It included 39 mildly malnourished children with a poor appetite for over 3 months and 156 children who were healthy except for minor illnesses as the control group. All the children were regular attendees at the outpatient clinic and were tested for serum levels of 25-hydroxy vitamin D. We used binary logistic regression statistical analysis to measure the significance of the association between vitamin D deficiency/insufficiency and anorexia with mild malnutrition in young children.
Results: Of the 39 children in the anorexia group, 20 had vitamin D deficiency, and the remaining 6 had vitamin D insufficiency. On the other hand, 16 of the remaining children with normal appetites, showed a vitamin D deficiency, and 38 of them displayed insufficiency. Statistically significant association between vitamin D deficiency and anorexia with malnutrition was noted (odd ratio: 9.808; 95% confidence interval: 4.089 - 23.523; p=0.0001), while it was insignificant with vitamin D insufficiency.
Conclusion: This study displayed a noteworthy relationship between vitamin D deficiency and anorexia with mild malnutrition in young children.
Anorexia is a designate for poor appetite of all kinds of food. It is characterized by a decrease in the desire to eat and can be caused by any illness. In a curable disease, the appetite should improve once the underlying cause is resolved. Anorexia is prevalent among children. Short-term illnesses in children can cause temporary loss of appetite without loss of weight. However, protracted loss of appetite is associated with inadequate weight gain, which may be due to various underlying serious conditions or behavioral (non-organic) causes.1 Vitamin D is a secosteroid, that plays an essential function in calcium homeostasis and has multiple other biological effects in the body.2 It is considered a hormone which acts via nuclear receptors present in multiple organs such as the bone, brain, intestine, kidneys, immune system, and most other body parts.3 The skin is considered as the main source of vitamin D supply following the exposure to the sun’s ultraviolet radiation.4 Vitamin D deficiency is pandemic and remains underdiagnosed and undertreated worldwide. It most commonly results from inadequate sun exposure, malabsorption, or problems related to the kidney and liver.5 Deficiency of vitamin D is the main etiology of rickets in children, and osteomalacia in adults.6 Extensive study has suggested that vitamin D deficiency might be responsible for the increase in the risk of the development of numerous illnesses such as asthma, diabetes mellitus, cardiovascular problems, immune defects, infections as well as cancer, which can be treated with the regular intake of vitamin D in physiological doses or by correction of its deficiency.5,7 Previous study reported8 that vitamin D deficiency is pervasive among adolescents who suffer from anorexia nervosa and bulimia nervosa. Also, it has been noticed that obese children are more liable to be deficient in vitamin D.9
In this study, we aimed to determine the relationship between vitamin D deficiency/insufficiency and the development of anorexia, which causes mild malnutrition in young children.
Methods
This cross-sectional study was conducted in Faruk Medical City, Sulaymaniyah, Kurdistan Region, Iraq. To avoid the seasonal changes in the vitamin D levels,10,11 the data were collected prospectively during the summer months between May and September 2018. We received written informed consent from the parents of the enrolled children. The Medical Research Ethics Committee of the College of Medicine, University of Mosul, Iraq approved the study, which is consistent with the principles of the Helsinki Declaration.
In this study, we included children aged 2-6 years who visited our outpatient department, and were suffering from anorexia for over 3 months along with mild malnutrition but had no underlying serious or chronic illnesses. Children with anemia, underlying chronic illnesses, a picky eating which is a commonly encountered habit in children with a tendency to food selection, as well as diet neophobia which does not result in malnutrition, were excluded from the study.12
Since we had multiple data points for each child, the level of nutrition was diagnosed based on the deceleration of the child’s Z-score for weight-for-height. A Z-score decline of one was considered as mild malnutrition based on the American Society for Parenteral and Enteral Nutrition consensus statement on pediatric malnutrition.13 The children enrolled in this study were divided into 2 groups (anorexia with mild malnutrition group and, a normal appetite group). All these cases were registered, and had medical records in the hospital, which indicated that their previous Z-scores ranged from 0 and -0.9. In addition to a thorough physical examination, detailed nutritional, birth, family, and social histories were collected from each participant in the study. For subjects with malnutrition in the anorexia group, further tests including, complete blood count, urinalysis, and other clinically directed blood tests such as iron profile, celiac screening, thyroid function tests, and other radiological investigations, were performed to rule out any possible underlying illnesses that may be responsible for anorexia and mild malnutrition.
Both groups were tested for 25-hydroxyvitamin D serum levels. Given that the normal range for 25-hydroxyvitamin D in healthy subjects is 20-50 ng/ml, a cut-off value of 20 ng/ml was chosen based on the recommendations of the 2016 Global Consensus. Levels between 12-20 ng/ml indicated vitamin D insufficiency, and those below 12 ng/ml indicated vitamin D deficiency.10,11
The Google Scholar search engine and the PubMed electronic database have been used to find prior related researches using keywords like vitamin D deficiency, anorexia, malnutrition, and leptin.
Cobas e 411analyzer (Roche Diagnostics GmbH, Mannheim, Germany) was used for the measurement of 25-hydroxyvitamin D (Elecsys®Vitamin D total), ferritin (Elecsys® Ferritin, Roche Diagnostics International.) and thyroid function tests (The Elecsys TSH, Elecsys® T4). Swelab Alfa Plus hematology analyzer (Spånga, Sweden) was used for the determination of complete blood count, and Chorus Elisa kits (Diesse Diagnostica Senese Spa, Monteriggioni, Italy) were used for the celiac screen (CHORUS TTG-A).
Statistical analysis
To evaluate the role of vitamin D deficiency/insufficiency in the occurrence of anorexia with poor weight gain, we used binary logistic regression analysis, in which the data of cases with anorexia and malnutrition were considered as the dependent variable (we implemented 1.0 as a binary model for the analysis of values of cases with anorexia and malnutrition), and 3 independent variables (predictors) according to vitamin D serum levels (normal, insufficient as well as vitamin D deficient values). We calculated the odds ratio as well as the confidence interval for each association. Significance was determined using the Chi-square test (with one-degree freedom), and a p-value of less than 0.05 was considered to be significant. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 23 (IBM Corp, Armonk, NY, USA).14
Results
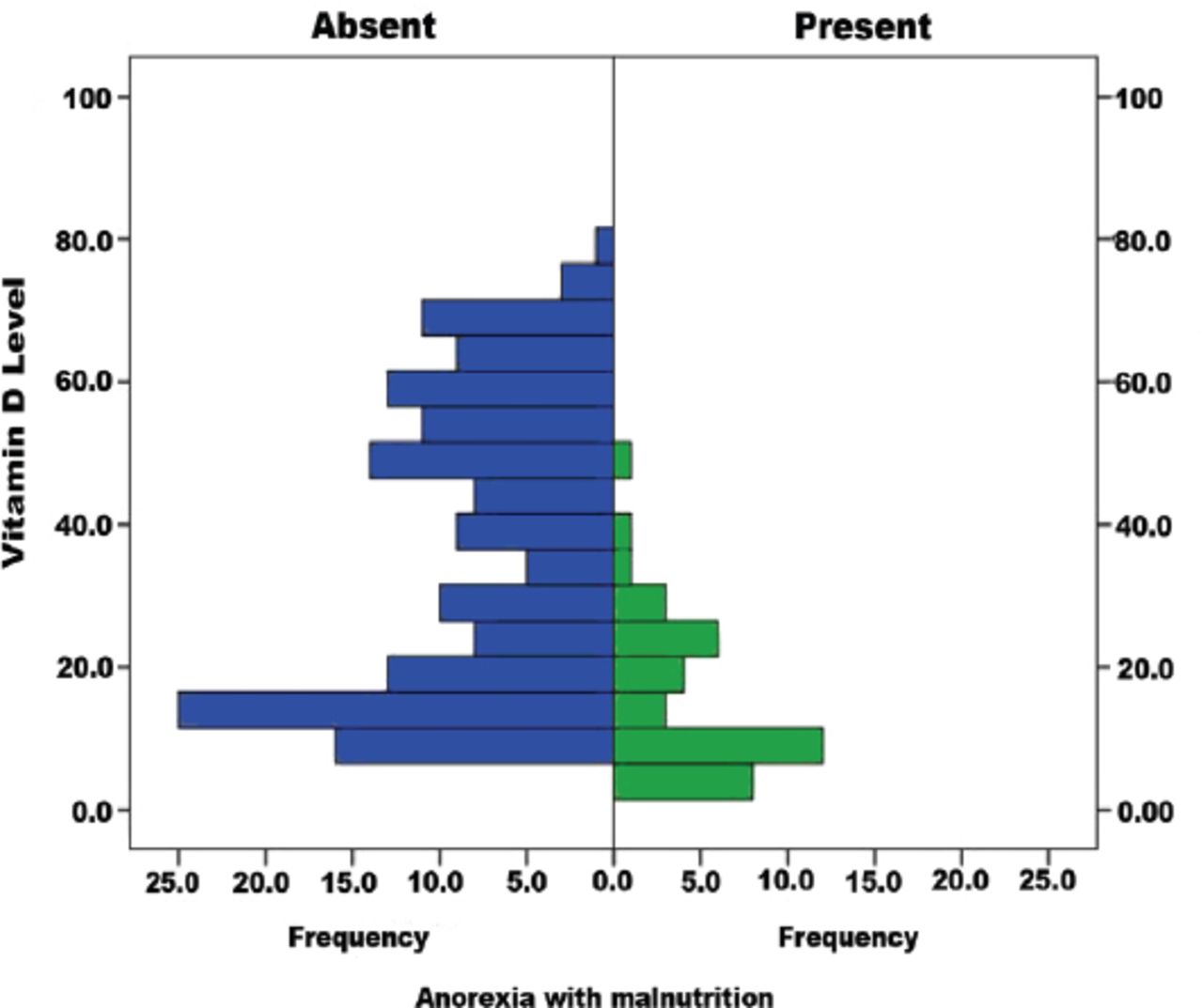
We enrolled a total number of 195 children, of which 39 (mean age: 50.3±14.3 months) had anorexia and mild malnutrition (anorexia group). The remaining children (mean age: 48.98±15.2 months) formed the normal appetite group (Table 1). While more than half of the subjects in the anorexia group had vitamin D deficiency, a small proportion of them had vitamin D insufficiency. The majority of the children in the normal appetite group had normal vitamin D levels (Figure 1). Our results revealed a significant association between vitamin D deficiency and loss of appetite with mild malnutrition in children aged 2-6 years, whereas vitamin D insufficiency showed no significant association (Table 2). Mean vitamin D levels shown in Table 3 indicate that girls were predominant among children with vitamin D deficiency/insufficiency in both groups.
Distribution of subjects based on gender and vitamin D levels (N=195).

Relationship of vitamin D levels with the development of anorexia and malnutrition.
Statistical analysis using logistic regression showing the significance of association of low vitamin D levels with anorexia.
Vitamin D levels in the anorexia and normal appetite groups.
Discussion
Vitamin D is a key element required for maintaining good health.15 Our study shows a significant association between vitamin D levels and anorexia, which could, in turn, contribute to mild malnutrition seen in children aged 2-6 years. Our results are in line with the report published by Combs et al,16 which showed that loss of appetite is a symptom of vitamin D deficiency. Another study by Maetani et al17 has described an inverse relationship between levels of vitamin D and leptin hormone (also known as the anorexigenic hormone). Underlying this inverse relationship is the D - mediated inhibition of leptin hormone, which could account for the decrease in appetite and weight loss in vitamin D deficient subjects.17 Hajimohammadi et al18 also suggested a similar relationship between levels of vitamin D and leptin hormone in his meta-analysis of several observational studies. Many studies in adolescents have reported a significant association between vitamin D deficiency and eating disorders like anorexia nervosa and its sequel.8,19 However, the findings on vitamin D and eating disorders have been conflicting. Horlick20 has reported that vitamin D deficiency interferes with the secretion of the appetite-suppressing hormone, leptin, leading to an increase in appetite.20 Other studies have also shown that obese children are more prone to vitamin D deficiency.9,21 Additionally, the role of vitamin D in the loss of both appetite and weight has been demonstrated in conditions of vitamin D toxicity.22
Our study also highlighted the differences in the effects of vitamin D levels on anorexia based on gender. Most of the children with vitamin D deficiency and insufficiency in the anorexia and control groups were girls, which can be explained by the type of clothing they wear, covering most of their body. Moreover, compared to boys, girls spend less time playing outdoors, thereby reducing their sun exposure, which is essential for vitamin D synthesis. A study of vitamin D in children of school age in Saudi Arabia has also revealed that girls are more liable to have vitamin D deficiency when compared to boys.23
Study limitations
First is the small sample size, which was due to the short study period to avoid seasonal variations in the levels of vitamin D. Second, despite the efforts to exclude subjects with underlying chronic diseases that cause anorexia and poor weight gain, the possibility of having included such children cannot be totally ruled out. Third, the study does not test the association between vitamin D deficiency and the other more severe forms of malnutrition. Fourth, there is no follow-up so the causality is limited. Finally, although we tried to exclude toddlers with unclear picky eating behaviors, the unintended inclusion of such children could have influenced the results.
In conclusion, the role of vitamin D deficiency in the emergence of anorexia with mild malnutrition among young children, which could be added as a new finding to what is already known of its relation with eating disorders in adolescents. Our findings reveal a significant association between vitamin D deficiency and anorexia with poor weight gain in children, thereby suggesting that vitamin D deficiency might be the consequence of anorexia, or it could be a factor contributing to anorexia in children younger than 6 years of age.
Further studies are recommended to validate our findings and to determine if vitamin D supplements or therapeutic correction of vitamin D deficiency can help lower the risk of anorexia as well as resolve the eating disorders in children.
Acknowledgment
We would like to thank Editage (www.editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 30, 2019.
- Accepted September 24, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.