


Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42844.
An obese 74-year-old man with diabetes, hypertension, dyslipidemia, and mild systolic heart failure presented to the emergency department with a 2-week history of shortness of breath and orthopnea. This was associated with a constant cough that was productive with yellowish sputum as well as mild to moderate, sharp, bilateral flank and back pain. However, he denied hemoptysis, chest pain, and dysuria. He was dependent on a wheelchair as a result of residual right-sided weakness following a stroke that occurred 2 years prior to this presentation. The stroke also resulted in intermittent difficulty in swallowing that manifests as occasional choking on both solids and liquids. The patient was not compliant with medications or fluid restriction for heart failure and he suffered a fall from the wheelchair a few days prior to his presentation.
He was slightly tachypneic (respiratory rate 26 breaths/minute) with 85% oxygen saturation on room air. However, his heart rate (99 beats/minute), blood pressure (145/92 mmHg), and temperature were normal. Heart sounds were normal and the breath sounds were vesicular, but there were fine inspiratory crepitations, and the breath sounds decreased bibasally. There was bilateral lower limb pitting edema to the mid-calf. Although examination of the abdomen was unremarkable, both flanks were tender-predominantly over the lower ribs posteriorly. There was no new focal neurological deficit, and there was no evidence of aspiration on bedside swallowing assessment.
The complete blood count, creatinine, and electrolytes were normal; brain natriuretic peptide was 34 pmol/L. Renal tract ultrasound was unremarkable, and computed tomography (CT) of the abdomen excluded renal calculi. His chest x-ray (Figure 1) demonstrated small bilateral pleural effusions with bilateral interstitial infiltrates and Kerley B lines. These findings are consistent with pulmonary edema. The interstitial infiltration in the left lower zone was more prominent than that on the right. The presence of air bronchograms and the silhouette sign of the left heart border and diaphragm suggested left lingula and lower lobe consolidation. However, the dense radio-opaque shadow with irregular borders projected over the medial aspect of the right lower lobe was most intriguing.
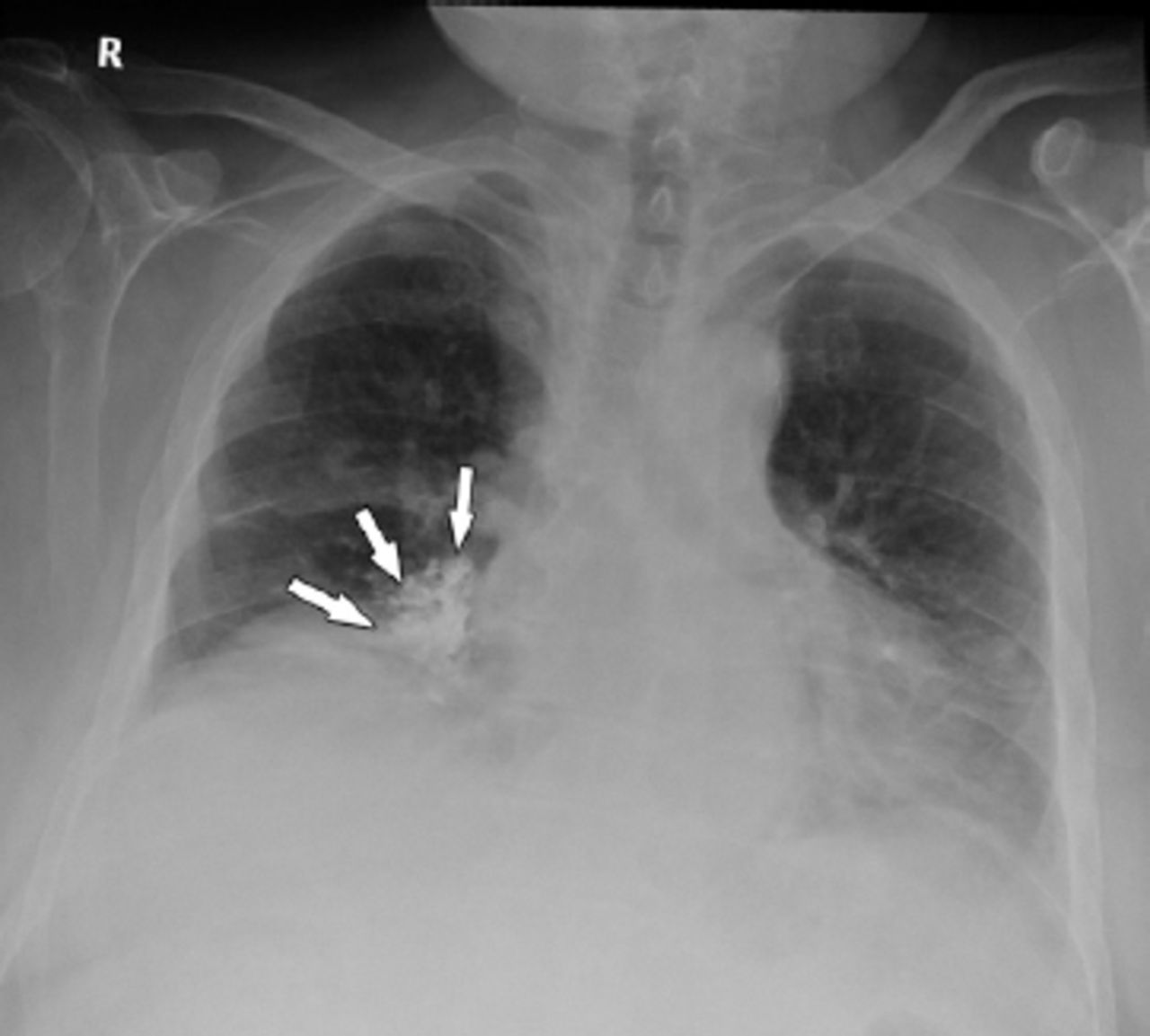
Antero-posterior chest x-ray, showing a small bilateral pleural effusion with interstitial infiltrate more on the left lower zone, silhouette sign of the left heart border, kerley B lines, and a dense focal opacity with irregular borders at the medial aspect of the right lower lobe.
Question
1. What is the cause of the dense radio-opaque shadow projected over the medial aspect of the right lower lobe?
Answer
1. Previous aspiration of a radio-opaque contrast agent into the right lower lobe (barium).
Discussion
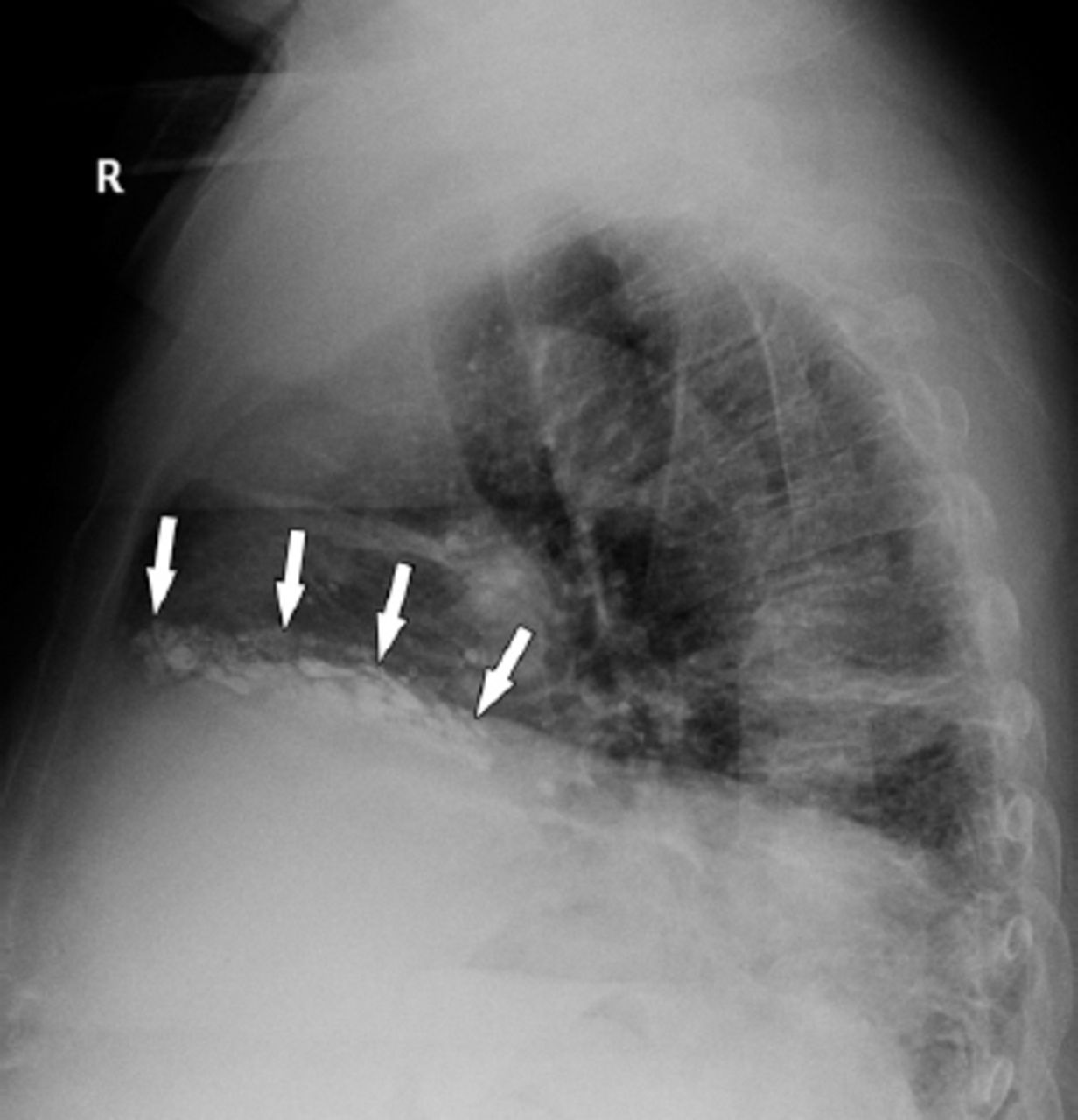
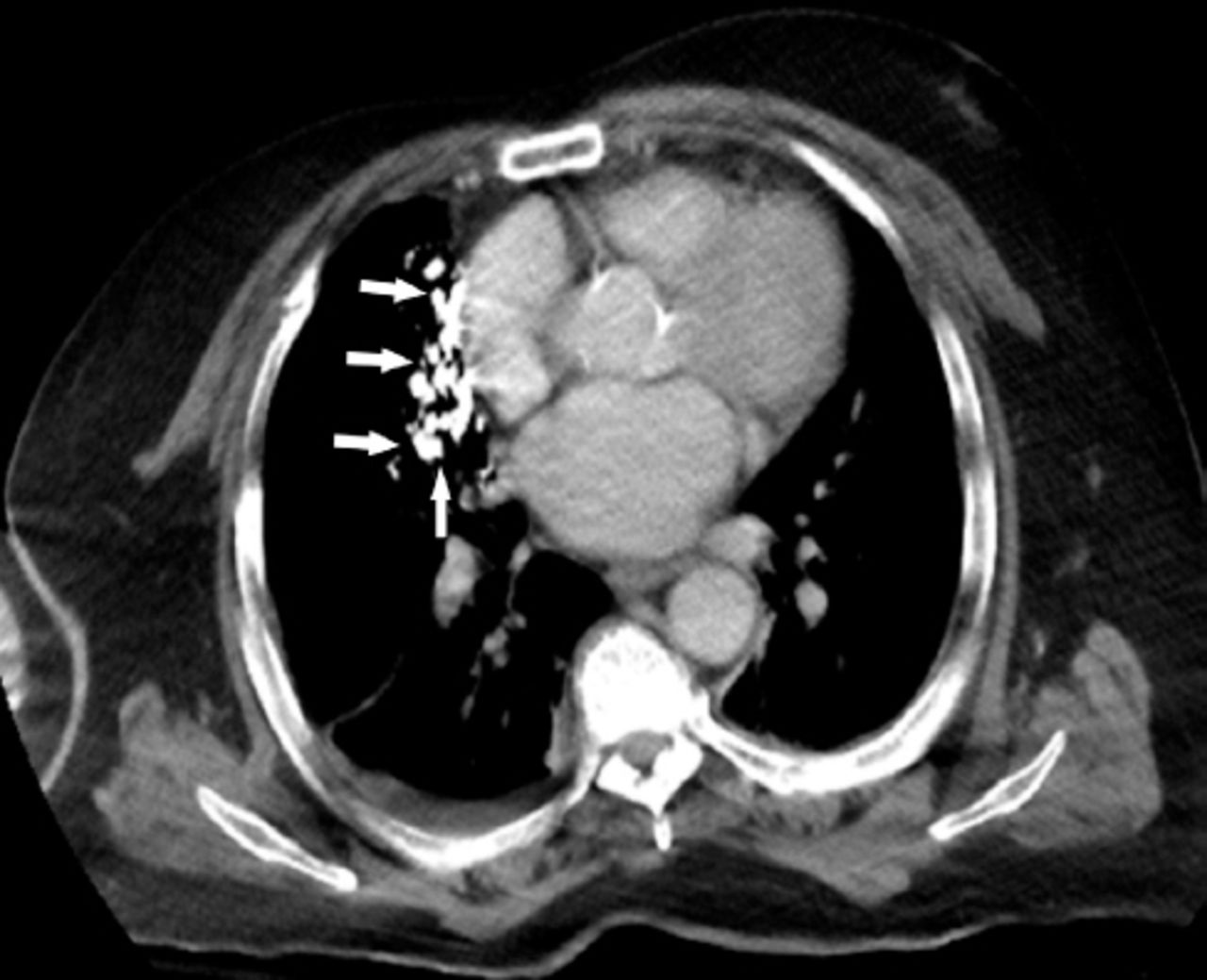
A lateral chest x-ray (Figure 2) revealed that this area consisted of multiple small radio-opaque opacities in the distribution of the bronchioles of the right lower lobe. This abnormality was confirmed on chest CT (Figure 3) suggesting aspiration of a radio-opaque contrast agent such as barium. Upon reviewing of previous imaging, it was noted that the patient had aspirated during a modified barium swallow test (Figure 4) performed 2 years prior to this presentation to assess the patient’s swallowing after his stroke.
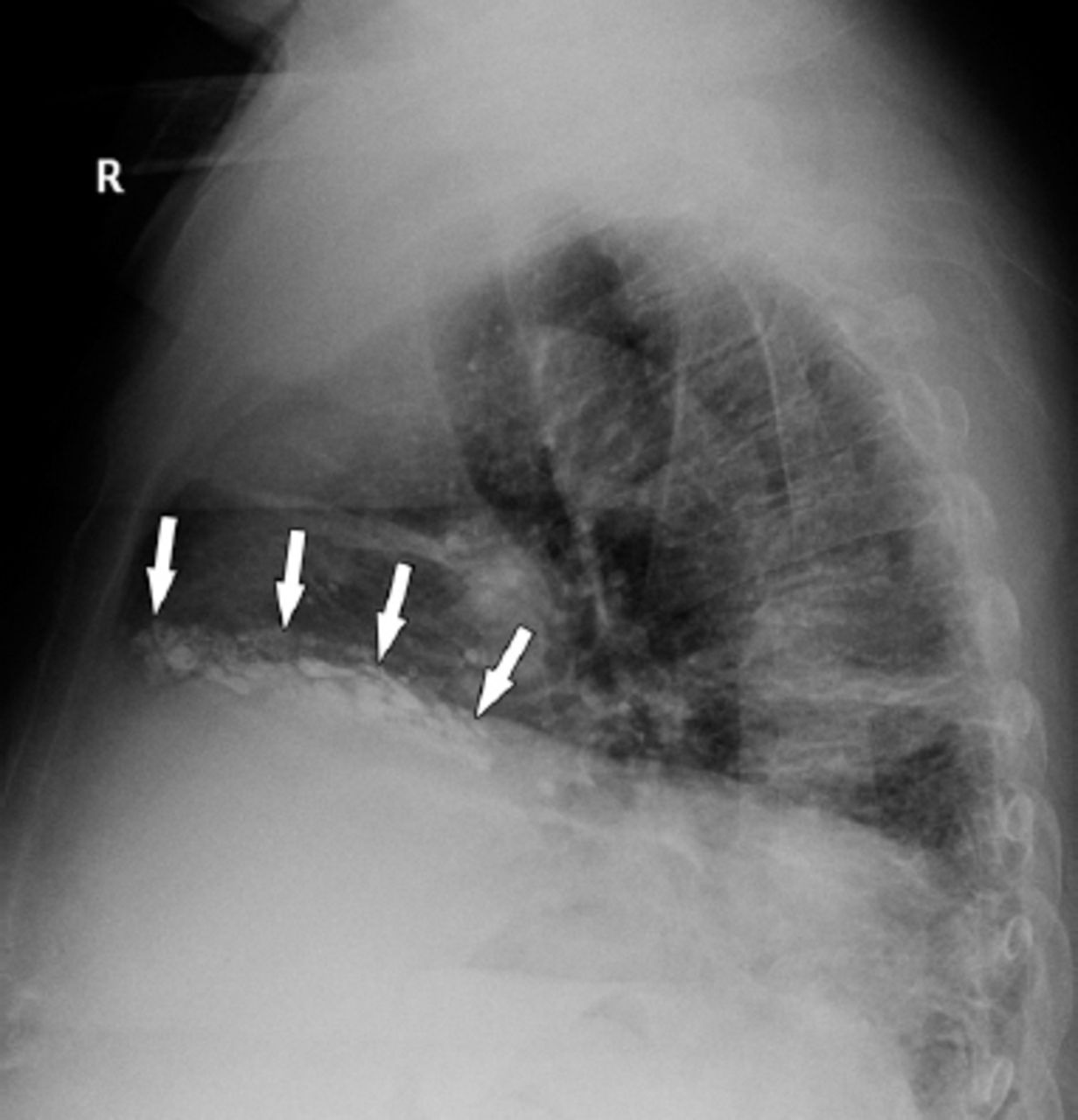
Lateral chest x-ray showing multiple small radio-opaque opacities in the distribution of the bronchioles of the right lower lobe
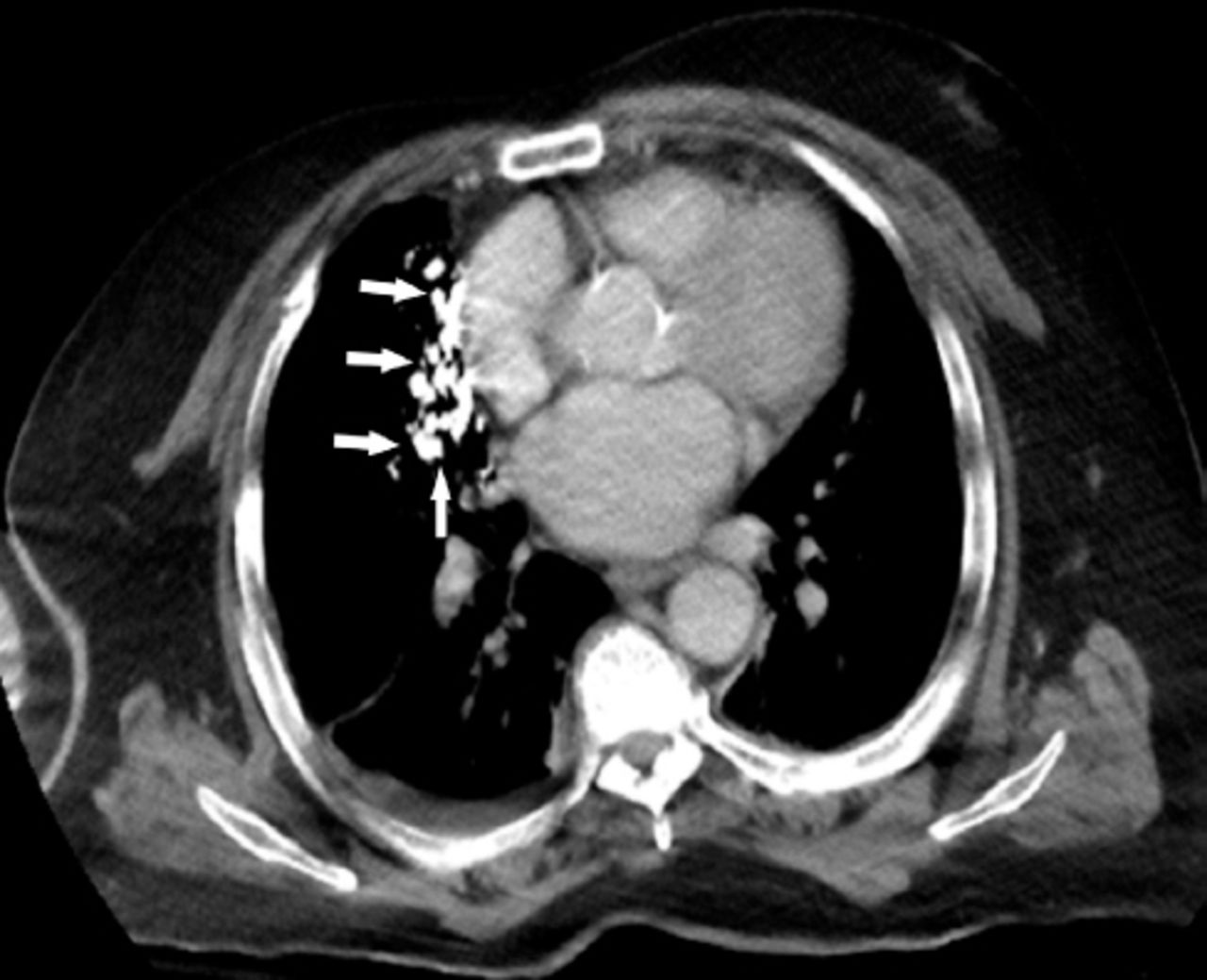
Chest CT showing multiple small radio-opaque opacities within the bronchioles of the right lower lobe.

Modified barium swallow showing barium aspiration during the procedure.
The chest CT (Figure 3) also demonstrated bilateral traumatic lower anterior and posterior rib fractures (the cause of the patient’s pain) as well as bi-basal interstitial infiltrates suggestive of pneumonia. The patient was treated for community-acquired pneumonia and cardiac failure with oxygen, intravenous diuretics, and antibiotics. He was also given topical and oral analgesia for the rib pain. These interventions significantly improved his symptoms.
Barium aspiration is a rare complication of any gastrointestinal study using barium sulfate as an oral contrast agent.1 The risk of barium aspiration increases in the presence of dysphagia secondary to dysfunction of swallowing or disorders of the central nervous system (for example, Parkinson’s or cerebral palsy, alcoholism or head and neck cancers).2 Barium is inert and does not cause clinical complications in small amounts; it can remain in situ silently for years.1 Aspiration of large amounts of barium can cause fatal respiratory failure, sepsis, chemical pneumonitis, and recurrent pneumonia.3 However, whether the pathophysiology and symptomatology are due to barium or the co-incident aspiration of gastric contents remains unclear.3 The mortality associated with aspiration of large amounts of barium is high: approximately 30-50% in patients presenting with circulatory shock or apnea.4
When aspirated, barium usually settles in the most gravitationally dependent areas of the lung. Thus, the exact location depends on the patient’s posture when the aspiration occurred and clearance mechanisms such as coughing.3 In adults, the right main bronchus is more vertical than the left. The right lung is therefore more likely to be affected by aspiration than the left. If aspiration occurs whilst the patient is upright, then the basal segments of the lower lobes are most likely to be affected. The middle lobes are more likely to be affected if the patient aspirates whilst leaning forward (for example, if vomiting or coughing). The posterior segments of the upper lobes and superior segments of the lower lobes are more likely to be affected if the patient aspirates while recumbent.2
All lobes of both lungs can be affected if large amounts of barium are aspirated (example in patients with tracheoesophageal fistula).5 Aspirated barium is usually visible on x-rays as dense radio-opaque shadows with a similar density to iron and tin.6 This is because the atomic number of barium (z=56) is high.7 The temporal resolution is time dependent.7 Plain chest x-ray is the screening test of choice for barium aspiration; high-resolution CT is used in severe cases for prognostication.4
Barium aspiration may cause mild interstitial lung fibrosis3 that results from phagocytosis of barium by alveolar macrophages.3 Barium can cause silent fibrosis in the form of thickening of interlobar septae, sub-pleural cysts, and centrilobar micronodules.3 Aspiration of gastric acid can also cause lung injury as a result of neutrophil sequestration and edema.7
Co-incident aspiration of gastric contents is more likely to cause complications than aspiration of barium.1 Indeed aspiration of barium is usually asymptomatic and intervention is rarely required. Thus, the use of a bronchoalveolar lavage to remove barium is controversial. It may be useful if large amounts of barium have been aspirated. But aspirating small to moderate amounts of barium via bronchoalveolar lavage could disseminate the barium to unaffected areas.3
Barium aspiration is a rare complication of oral contrast agent usage. The radiological appearance is often unusual and alarming. As demonstrated here, a lateral chest x-ray may provide better visualization of the aspirated barium. Reviewing previous investigations can help to avoid unnecessary expensive and invasive investigations such as CT of the chest. Oral contrast agents should be avoided in patients with a high risk of aspiration. Alternative modalities should be considered if investigation of the gastrointestinal tract is required.
Acknowledgment.
The authors gratefully acknowledge Prof. Hamdan Al-jahdali for his support.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.