


Abstract
Objectives: To define the importance of biochemical and virological thresholds for the prediction of significant liver diseases.
Methods: A total of 215 young and male HBeAg-positive cases followed up in a tertiary training and research hospital in Turkey between 2008 and 2017 enrolled in the retrospective diagnostic accuracy study.
Results: Fibrosis scores varied between 0-4, F1 (n=81, 37.6%) and F2 (n=82, 38.1%) were the most frequent fibrosis stages. Of the patients, 58.6% (126/215) had a significant histopathological abnormality (SHA). The ratio of SHA was higher for ALT >90 U/L (n=68/95; 71.6%) and HBV-DNA between 2,000,000-200,000,000 IU/mL (n=47/73; 64.4%). Thresholds for the higher odds ratio (OR) for SHA were >90 U/L for alanine aminotransferase (ALT) and >2,000,000 IU/mL for HBV-DNA. Based on receiver operating characteristic analysis, 90.5 U/L of ALT and 22,607,500 IU/mL of HBV-DNA were levels with the optimum sensitivity and specificity for the prediction of SHA.
Conclusion: Hepatitis B virus-DNA levels between 106 and 108 IU/mL and ALT levels of 2~3 x ULN might be considered to be good indicators for discriminating chronic hepatitis phase from chronic infection in hepatitis B e-antigen-positive chronic hepatitis. However, we think that the current biochemical, serological and molecular markers are inadequate for differentiating chronic hepatitis phase than chronic infection, and non-invasive test and/or liver histopathology should be carried out in selected cases.
Hepatitis B virus (HBV) infection still remains an important cause of liver cirrhosis and hepatocellular carcinoma (HCC) despite the vaccination policies and improvement in treatment modalities. Approximately 240 million people are diagnosed with chronic hepatitis B (CHB) infection worldwide.1 Countries are classified as low (<2%), intermediate (2-7%), and high endemic (≥8%).2 Turkey is one of the intermediate endemic countries with a Hepatitis B surface antigen (HBsAg) positivity prevalence of 4.57%, and it is estimated to be 3.3 million HBV carriers.3 Considering the prevalence rate in Turkey, mother-to-child transmission is still the most important cause of transmission of HBV, and so we still have high numbers of young patients with CHB. Chronic hepatitis B is defined as having HBsAg positivity for at least 6 months. Chronic hepatitis B infection has various clinical manifestations, which can be categorized according to hepatitis B e-antigen (HBeAg) status, hepatitis B viral load, and serum alanine aminotransferase level (ALT).2,4 One of the latest developments in HBV infection is about its classification; it is newly classified into 5 phases: HBeAg-positive chronic infection (formerly immune tolerant phase), HBeAg-positive chronic hepatitis (formerly immune clearance phase), HBeAg-negative chronic infection (formerly inactive carrier phase), HBeAg-negative chronic hepatitis (formerly immune reactivation phase), and HBsAg-negative phases.1 There are some cases in gray zones, which means that HBeAg status, viral load, and transaminase level do not fall into the same phase.2 And also, there are still some contradictive points about threshold values of HBV-DNA and upper limit of normal (ULN) for ALT between guidelines of international societies for estimating liver damage on HBeAg-positive patients.1,2,4,5 We have one of the largest numbers of liver histopathology results in young hepatitis cases in literature; these patients are all naive, healthy except for having HBV infection, have no comorbidities and all the cases underwent liver biopsies due to the regulation of military service in Turkey. One of the main difficulties in the management of patients with HBV is to determine the severity of liver disease, and the severity of the disease is mainly correlated with the phase of infection.
The aim of present study is to compare ALT and HBV-DNA levels with liver fibrosis and necroinflammatory scores. Our study results may contribute to the efforts for determining precise ALT and HBV-DNA thresholds for estimating liver damage among young patients with HBeAg-positive positive chronic hepatitis or chronic infection.
Methods
This retrospective diagnostic accuracy study was conducted in a tertiary training and research hospital. The study was approved by the Institutional Ethics Committee on May 2017 (HNEAH-KAEK 2017/KK/71). The retrospective study data were gathered by the clinicians who were in charge of following up the patients during the study period. The study includes the period between January 2008 and January 2017.
Study design and population
Because we are a military hospital, vast majority of our cases were the candidates for military service, and a few of them were ordinary patients who were followed up for hepatitis B. Turkey has a mandatory military service, and hepatitis B patients with the findings of chronic hepatitis in liver histopathology have the right to exempt from military service. We do liver biopsies according to the health regulations of Turkish Armed Forces with the consent of patients with HBV. And also, liver biopsy and histopathologic results are still mandatory for prescribing hepatitis B treatments according to Reimbursement Regulations of Turkish, Ministry of Health. Only the patients with necroinflammation grade ≥6 and/or fibrosis stage ≥2 in liver histopathology can be prescribed with oral antivirals. In the study, we considered necroinflammation grade ≥6 and/or fibrosis stage ≥2 as a significant histopathological abnormality (SHA). Liver biopsies to those who need treatment were carried out.
We first checked up the patients who were referred to our hospital from the recruitment offices or other hospitals with the history of hepatitis B for HBsAg, anti HBc-IgG/M, HBeAg, anti-HBe, HBV-DNA, anti-HCV, anti-HIV, complete blood count, liver transaminases, albumin, prothrombin time, alpha-fetoprotein, and some other additional tests if necessary. If the patient had HBsAg, HBeAg, and HBV-DNA positivity and ALT level over 40 U/L, we required to repeat the tests every 3 months for a period of at least 6 months. At the end of the follow up period, we performed liver biopsies to the ones who were still HBsAg and HBeAg positive, and had positive HBV-DNA and ALT levels consistently higher than 40 U/L. And also, there were few cases that we performed liver biopsies with high HBV-DNA levels and a fluctuating course of ALT over 30 U/L.
None of the patients had a history of liver biopsy or any treatment for hepatitis B. Patients who had history of HBV treatment with interferon or antiviral drugs, other chronic liver diseases or drug use and who had symptoms of cirrhosis or who are co-infected with other hepatitis viruses and human immunodeficiency virus (HIV) were excluded from the study.
All of the cases who fulfill the criteria above were included in the study. As a result, 215 young and male cases who were mostly the candidates of military service we included. Cases were divided into 2 groups whether they have SHA or not. Then, groups were analyzed in terms of the ALT and HBV-DNA levels.
Liver biopsy and histopathology
Patients with the history of chronical HBV infection underwent liver biopsy via Menghini’s aspiration method with 16G biopsy needles or via subcostal real-time ultrasound-guided trucut-style. A qualified biopsy specimen was minimum 1.5-cm-long and displayed more than 4 portal tracts. Histopathologic assessment of liver biopsies was based on the Knodell histologic activity index (HAI) for necroinflammation and Ishak’s scoring system for fibrosis stage. Not all the pathological assessments were carried out by the same pathologist but they were all trained in the same pathology department and they are still working in the same pathology laboratory.
Laboratory tests
Serum biochemistry tests including ALT and AST were determined by commercial kits. Hepatitis B virus serological markers were detected using chemiluminescence microparticle immunoassay (Abbot, Architect System, Germany). Hepatitis B virus-DNA was quantitatively determined by HBV QNP 2.0 real time polymerase chain reaction (PCR) assay (Iontek, Turkey) with a lowest detection limit of 10 IU/mL (80 copies/mL) and limit of quantification between 2x109 and 2x101 IU/mL.
Statistical analysis
Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 15. The baseline characteristics were presented as means and standard deviations for continuous variables and as frequencies and percentages for categorical ones. Comparisons of continuous variables were performed by independent samples Student’s t test and Mann-Whitney U test according to those distributions. Categorical variables are compared by using Chi-squared test and Fisher’s exact test. The receiver operation characteristic (ROC) analysis was used to determine optimal threshold levels for serum ALT and HBV-DNA observed in study population. Diagnostic performance was analyzed by VassarStats; web-based application (Website for Statistical Computation, www.vassarstats.net). G*Power 3.1.9.2 was used for performing post-hoc power analysis. The study has 90% power to detect minimum 20% of difference for significant liver histology within patients categorized according to their serum HBV-DNA and ALT levels.
Results
A total of 215 HBeAg-positive cases were included in the study. All of the patients were male and young; average age was 22.91 years. The mean ALT levels of all patients was 83.05 U/L, AST was 42.14 U/L, AST/ALT ratio was 0.57 and Log10 HBV-DNA was 7.14 IU/mL. There was no difference in mean age and AST/ALT ratio among non-SHA (p=0.155) and SHA groups (p=0.146) (Table 1). Patients with SHA had higher values of mean ALT (p<0.001), mean AST (p<0.001) and mean log10 HBV-DNA (p=0.036) than the patients with non-SHA.
Comparison of age, clinical, and virological data between 2 groups according to the status of liver disease.
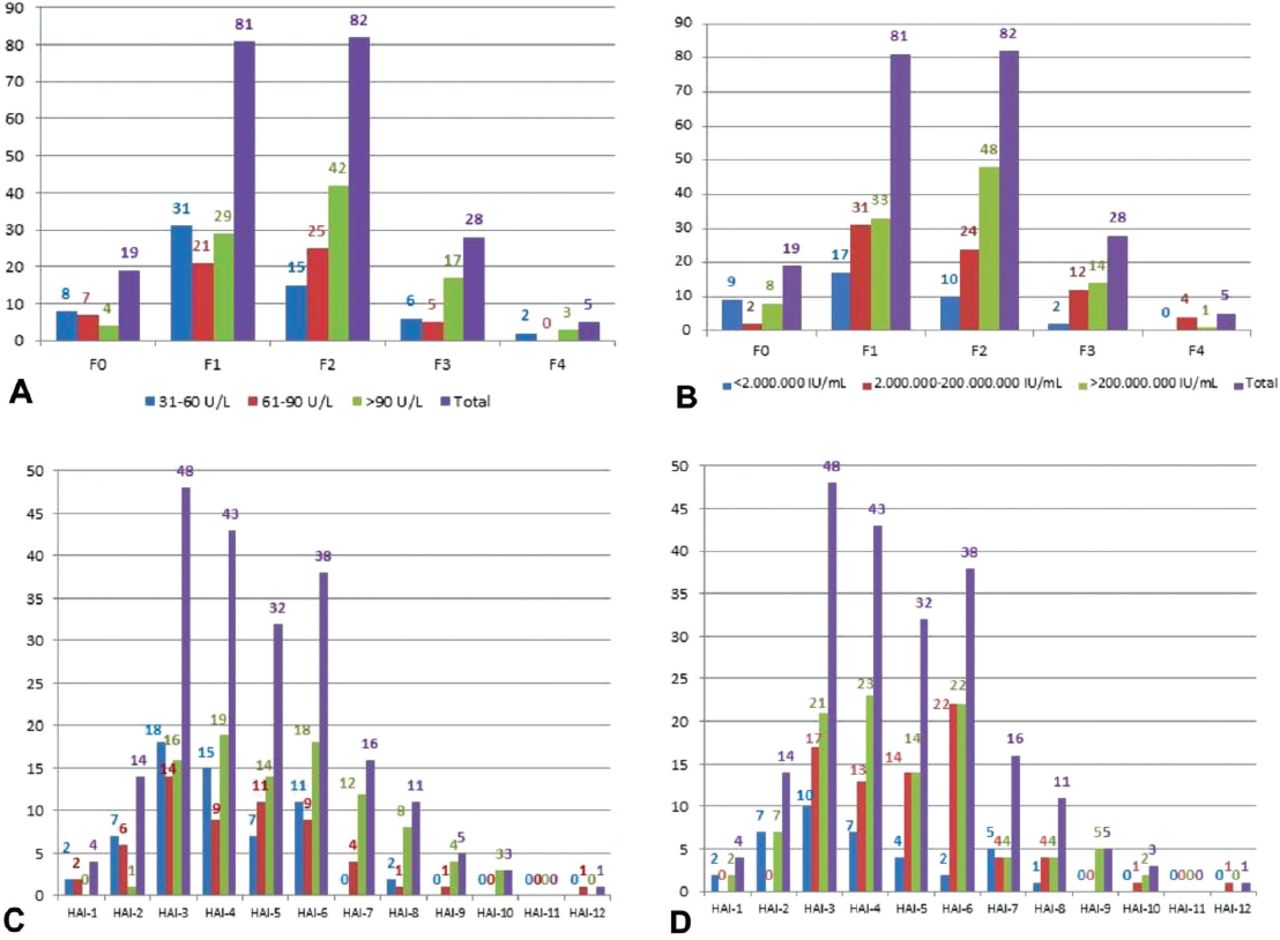
Fibrosis scores of all cases varied between 0 and 4, F1 (37.6%) and F2 (38.1%) were the most frequent fibrosis stages. Fibrosis score=1 was the most frequent fibrosis stage (50%) in cases with ALT 31-60 U/L. Fibrosis score=2 was the most frequent fibrosis stage in cases with ALT 61-90 U/L and >90 U/L (43.1% and 44.2%, respectively) (Figure 1A).

Distribution of the 215 cases according to alanine aminotransferase (ALT), HBV DNA levels and fibrosis, histologic activity index (HAI) stages. Graphs according to A) ALT levels and fibrosis stages, B) HBV DNA levels and fibrosis stages, C) ALT levels and necroinflammatory grade, and D) HBV DNA levels and necro inflammatory grade.
In cases with HBV-DNA <2,000,000 IU/mL and 2,000,000 - 200,000,000 IU/mL, F1 was the most frequent fibrosis stage (44.7% and 42.4%, respectively). Fibrosis score=2 was the most frequent fibrosis stage (46.1%) in cases with HBV-DNA >200,000,000 IU/mL (Figure 1B).
Necroinflammatory grades of all cases varied between 1 and 12. Histologic activity index scores of
3, 4, 5, 6 were the most frequent scores (22.3%, 20%, 14.8% and 17.6%, respectively).
HAI-3 was the most frequent necroinflammatory score in cases with ALT 30 - 60 U/L (29%) and 61- 90 U/L (24.1%). HAI-4 was the most frequent score (20%) in cases with ALT >90 U/L (Figure 1C).
In cases with HBV-DNA <2,000,000 IU/mL, HAI-3 was the most frequent score (26.3%). HAI-6 was the most frequent score (30.1%) in cases with HBV-DNA 2,000,000 - 200,000,000 IU/mL, and HAI-4 was the most frequent score (22.1%) in cases with HBV-DNA >200,000,000 IU/mL (Figure 1D).
Cases were divided into 2 groups according to liver histological status; described as SHA (HAI: ≥6 and/or F: ≥2). Of all cases, 53.5% (115/215) had F: ≥2 score, 34.4% (n=74/215) had HAI: ≥6 score, 29.3% (n=63/215) had both HAI: ≥6 and F: ≥2 score, and consequently, 58.6% (n=126/215) had SHA. The ratio of SHA was higher in ALT group. The distribution of SHA in the combined group analysis is presented Table 2.
Distribution of cases with SHA according to ALT and HBV DNA levels [n / (%)].
According to the risk estimation analysis for SHA, the odds ratio (OR) was higher in patients with ALT than ALT, it was statistically significant for both. The OR was higher in patients with HBV-DNA than HBV-DNA. In combination group analysis, the OR was highest among the patients with ALT and HBV-DNA (Table 3).
Risk estimation for SHA according to ALT and HBV DNA threshold levels by fisher’s exact test
In diagnostic performance analysis, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+) and negative likelihood ratio (LR-) were calculated (Table 4). The diagnostic performance analysis of ALT with HBV-DNA threshold level combinations was also performed (Table 4).
The diagnostic performance of alanine aminotransferase (ALT) and HBV DNA threshold levels to predict significant histological abnormality (SHA).
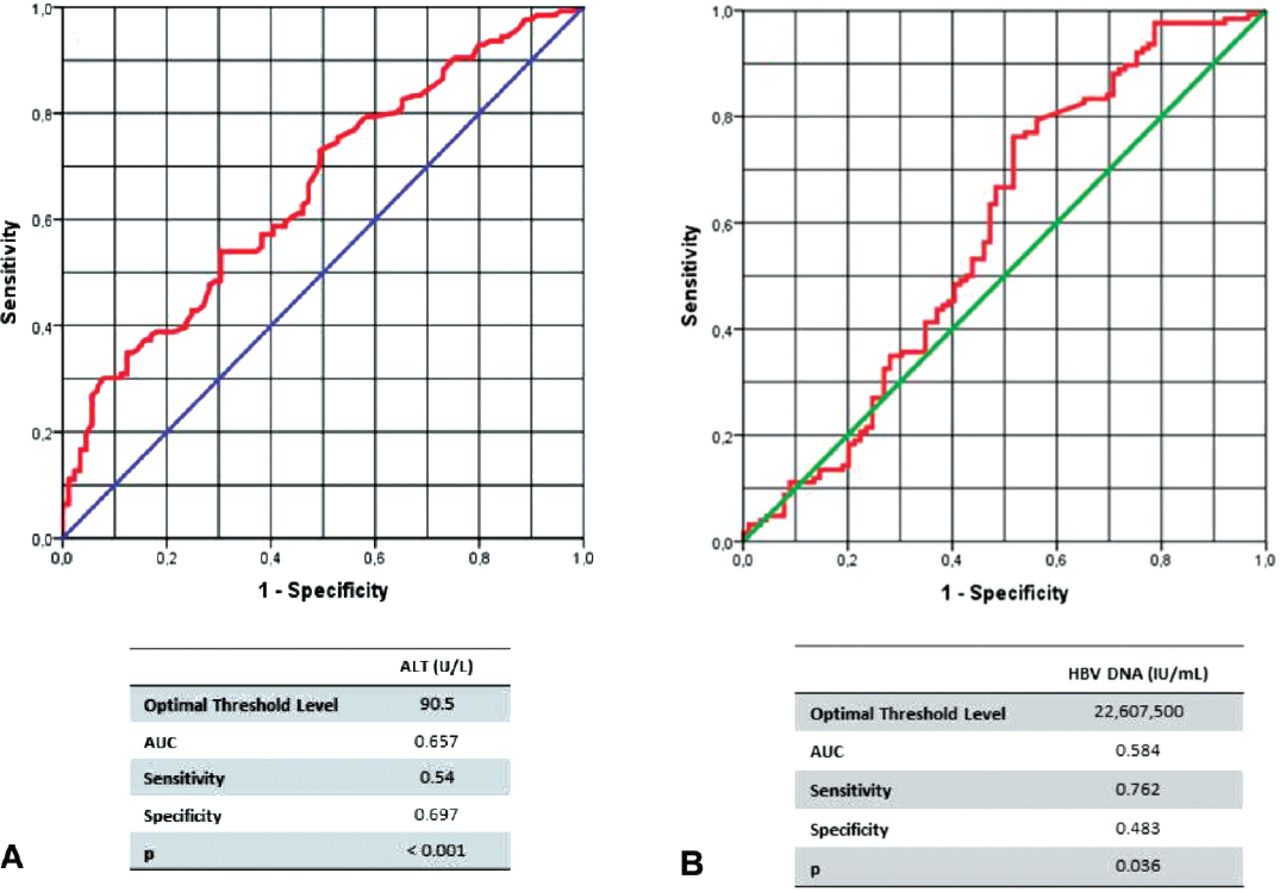
Based on the receiver operating characteristics (ROC) curve analysis of serum ALT and HBV-DNA levels, threshold levels with the optimum sensitivity and specificity for the prediction of SHA were determined. The optimum ALT threshold level was 90.5 U/L. The optimum serum HBV-DNA threshold level was 22,607,500 IU/mL (Figures 2A & 2B).

Area under the receiver operating characteristic curve of A) alanine aminotransferase (ALT) and B) HBV DNA for predicting significant histological abnormality (SHA). AUC - area under the curve
Discussion
There are 2 contradictive issues in HBeAg-positive phase; first, there is no consensus on the discrimination of HBeAg-positive infection and hepatitis phases, and the second, the debates on treatment indications for HBeAg-positive cases with normal or minimally elevated ALT have not come to a conclusion yet. Although there are some differences in terminology, monitoring and treatment criteria among the recent guidelines for the management of HBV are published by the World Health Organization (WHO), The American Association for the Study of Liver Diseases (AASLD) and The Asian Pacific Association for the Study of the Liver (APASL) in 2015, The European Association for the Study of the Liver (EASL) in 2017, the treatment indications to start treatment are mostly the same in HBeAg-positive and HBeAg-negative CHB; mainly based on serum HBV DNA, ALT levels and the severity of the liver diseases.1,2,4,5 According to these guidelines, ALT threshold level is controversial. It is argued to decrease the ALT threshold levels as 19-25 U/L for females and 30-33 U/L for males in the WHO and AASLD guidelines, and the latest AASLD guideline support the ALT threshold levels as 25 U/L for females and 35 U/L for males in the management procedure of chronic HBV. On the contrary, APASL and EASL accept that there are no available data to support the need for lowering the traditional thresholds for the ULN of ALT values.6 And also in literature, ALT levels between 25 and 40 U/L is considered as high normal, in which histopathological changes is more likely to occur.7
In HBeAg-positive infection phase, studies have shown that the risk of fibrosis progression is very low and patients receiving treatment have a lower HBeAg seroconversion rate.8 Lai et al7 showed that 12% (n=3/25) young immunotolerant patients had significant fibrosis. Andreani et al9 revealed that 50% (n=20/40) of immunotolerant patients had mild, the rest had no fibrosis, and the median age of loss of tolerance in those 12 patients was 30.7 years, 3 of them developed chronic hepatitis while six developed inactive diseases.9 According to the results in these studies, treatment is recommended only in patients who have advanced liver fibrosis. It is also known that approximately 8-20% of untreated HBV infected cases develop cirrhosis within 5 years, and the risk of developing HCC is significantly higher in patients with prolonged high viremia.10
Traditionally, liver biopsy is considered to be the gold standard method to estimate the severity of the liver disease.11 However, there are not strict recommendations anymore for liver biopsy in international guidelines due to the improvements in non-invasive markers of liver fibrosis. In developing countries like Turkey, non-invasive tests like fibroscan are too expensive and still lack of availability countrywide. In 2017, Turkish practical guidelines about diagnosis, management and treatment of HBV infection, treatment is recommended for HBeAg positive patients older than 30-years-old with normal ALT and high HBV-DNA levels.12 However, there is not a clear-cut recommendation to perform liver biopsy before 30-years-old. The main reason for performing biopsy for our cases on ≤30-years-old was the health care regulations for military service in Turkey, and 97.2% of our cases who had liver biopsy were younger than 30 years of age.
Even though they are identified under the name of same disease as chronic hepatitis B infection; there are some differences between HBeAg-positive and negative cases in terms of management, monitoring and treatment recommendations meaning that they are two different diseases of the same infection. Higher risk of HCC was reported in HBeAg-positive cases related to higher HBV-DNA levels and more prolonged hepatitis in these cases, and patients remaining HBeAg-positive over 30 years old have a significantly higher life-time risk of HCC than HBeAg-negative cases, 87% versus 12%, respectively.13 According to EASL 2017 guideline, one of the main differences in the treatment indications between HBeAg-positive and negative phase is that patients older than 30 years with high viremic HBeAg-positive chronic HBV infection may be treated regardless of the severity of liver histological lesions, although they have persistently normal ALT levels.4 Also Vlachogiannakos et al10 suggest that HBeAg-positive cases with HBV-DNA over 20,000 IU/mL and age over 30 years should be treated regardless of ALT and liver histology. In middle income countries like Turkey, treatment of both HBeAg positive and negative cases has the most health-gain and is cost-effective.14 However, the most important issue about the treatment indications is the reimbursement arrangements of countries; and these arrangement policies are usually not correlated with the current literature and guideline recommendations.15 In a study made in 5 different European countries including our country (Turkey, Germany, France, Poland and Romania) showed that up to 39% of patients who fulfils the treatment criteria according to EASL guideline did not have treatment for CHB.13 In present work, though we had very young patients with mean age of 22.9, the risk of having treatment indication (necroinflammation grade ≥6 and/or fibrosis stage ≥2) was almost threefold higher in cases with HBV-DNA >2,000,000 IU/mL. Of all cases, 58.6% had SHA; they fulfilled the treatment criteria both according to EASL and reimbursement arrangements of Turkey. Even in the subgroup with HBV-DNA <2,000,000 IU/mL and ALT between 30-60 U/L, one fourth of the cases had SHA. Moreover, 91% of all cases in this study had fibrosis scores between 1 and 4; all these findings may suggest the need for treatment in earlier decades in HBeAg-positive high viremic cases.
In literature, there are few studies in HBeAg-positive cases aiming on correlation or relationship between HBV-DNA and liver fibrosis and/or necroinflammation; studies are mostly in HBeAg-negative cases.6,16-19 Hepatitis B virus-DNA threshold level for the treatment indication of CHB due to the reimbursement arrangements of Turkey is 2,000 IU/mL; same level for both HBeAg-positive and negative CHB cases.13 However the HBV-DNA threshold level for indicating significant histopathological damage is unclear in HBeAg-positive phase. Unlike HBeAg-negative cases, 2,000 IU/mL of HBV-DNA threshold level is inadequate in HBeAg-positive cases, because only a few amounts of HBeAg-positive cases have HBV-DNA level below 2000 IU/mL. According to the results of our study, only 6% of the cases had HBV-DNA below 2,000 IU/mL, and moreover only 17.7% of them had HBV-DNA below 2,000,000 IU/mL. In all current guidelines, it is given for HBV-DNA that the levels are very highly elevated in HBeAg-positive infection but it is less in HBeAg-positive hepatitis; however, there is not a clear-cut threshold and consensus on the threshold HBV-DNA level for differentiation of two phases. Our results revealed that higher HBV-DNA levels (>200,000,000 IU/mL) indicate HBeAg-positive infection rather than hepatitis. According to the study of Xie et al20 the optimal level of serum HBV-DNA to evaluate low risk of significant fibrosis was ≥6.7 log 10IU/ml (~0.5 x107 IU/mL), and patients with HBV-DNA levels <4.7log 10IU/ml (~0.5 x105 IU/mL) all had significant fibrosis.20 In our study, the optimum threshold HBV-DNA level to predict SHA was 2.2 x107 IU/mL, which was similar with EASL 2017 guideline; according to this guideline, 107 IU/mL is given as the HBV-DNA threshold level for discriminating chronic hepatitis than infection.4 So, application of the HBV-DNA threshold level (107 IU/mL) for HBeAg-positive cases defined in EASL 2017 guideline appears to be more practicable.
While treatment on patients with persistently normal ALT levels (PNALT) is not indicated, EASL 2017 guideline approaches the treatment recommendation in HBeAg-positive cases over 30 years old more aggressively, regardless ALT levels.4 Zeng et al21 conducted a study to show the significance of liver biopsy in CHB; they first identified the hepatitis phase of patients by the serological (HBeAg, HBV-DNA and ALT) profile only, and then serological plus histological profile. According to the study results, they revealed that the diagnostic accuracy of the serological profile for only immune-tolerant phase was low, and half of the cases (n=56/112) diagnosed as immune-tolerant by serological profile was confirmed as immune-tolerant by serological plus histological profile, thus 50% of immune-tolerant patients identified by serological profile may not have been given antiviral treatment if they were not performed liver biopsy. Xie et al20 revealed that patients with ALT 1-2×ULN and >2×ULN had similar significant fibrosis rates (48.4% versus 51.8%). Additionally in the case series of Kumar et al22 ≥2 fibrosis rates in cases with PNALT was 3-fold higher in HBeAg-positive cases; 39.7% (n=29/73) versus 13.8% (n=8/58) in HBeAg-positive and negative cases, respectively. According to the results of these studies, having normal ALT level may not be sensitive enough for discriminating HBeAg-positive chronic infection than hepatitis, and the significance of ALT is lower in HBeAg-positive phase than HBeAg negative, or at least we should determine new ALT threshold for HBeAg-positive phase unlike to HBeAg-negative phase. According to the liver stiffness measurement results of 453 HBeAg-positive cases by Wong et al,23 the risk of advanced fibrosis increases in patients with an ALT level greater than 0.5 x ULN; ULN was 58 IU/L in the study. Seto et al24 revealed in their study including 211 HBeAg-positive naïve cases that 22.5% (n=9/40) cases with normal ALT levels had SHA (necroinflammation grading ≥7 or fibrosis score ≥3), but most of these cases had high normal ALT levels. There was a significant difference in fibrosis scores among cases within normal ALT levels using Prati criteria (30 U/L for men, 19 U/L for women) and cases within normal ALT levels but exceeding the Prati criteria. The results of their study also showed no significant differences in fibrosis staging among ALT 1-2 x ULN and x2 ULN in all HBeAg-positive cases.24 Apart from these studies, we do not have persistently normal alanine aminotransferase (PNALT) cases in our study. But in our focus group, we revealed that SHA rates increase concordantly among the ALT groups even in young age (30-60, 60-90 and >90 U/L) with the highest rate in >90 U/L. Over 40% of cases in the lowest ALT group had SHA, which was not a low rate for this young-aged group. And also, the risk of SHA was about 2.6 times higher in the group with ALT over 60 U/L, approximately same as in the ALT group over 90 U/L. Considering the sensitivity, specificity, PPV, NPV as a whole in diagnostic performance analysis, we considered 60 U/L ALT as the optimum threshold value for prediction of SHA, because sensitivity value of 60 U/L were markedly higher than 90 U/L, although there was a slight difference in PPV. Also, 2,000,000 IU/mL was considered as the optimum threshold with higher sensitivity and PPV. In further analysis, 60 U/L ALT with 2,000,000 IU/mL HBV-DNA together showed better performance for prediction of SHA with higher sensitivity, PPV and also with acceptable specificity and NPV.
This study is focused on naive, male and young population; these characteristics of population in the study may promote the importance of the results indicating the importance of ALT levels and viral load on liver histology in young male population. On the other hand, these characteristics may also be considered as the limitation of the study, and more attention should be paid to adapting study data to the general population.
In conclusions, HBeAg-positive and negative phases have totally different and distinctive dynamics that need different management. The results of our study revealed that HBV-DNA level between 106 and 108 IU/mL and ALT level of 2~3 x ULN might be considered to be good indicators for discriminating chronic hepatitis phase from chronic infection in HBeAg-positive chronic hepatitis. However, we think that the current biochemical, serological and molecular markers are inadequate for differentiating chronic hepatitis phase than chronic infection, and non-invasive test and/or liver histopathology should be done in selected cases.
Given that our study was performed over a highly selected population, the results cannot be generalized to all patients, and there is a need for further studies in generalized populations.
Acknowledgment
All authors would like to thank Ersin Tural for the statistical analysis.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 22, 2018.
- Accepted January 10, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.