


Abstract
Objectives: To assess phosphate binders’ usage, knowledge regarding their utilization, and adherence among hemodialysis patients in Qassim, Saudi Arabia.
Methods: A prospective cross-sectional study conducted at 4 dialysis centers in Qassim, Saudi Arabia with inclusion of 237 patients’ undergoing hemodialysis between November 2018 to January 2019. The study involved interviewing the patients, reviewing their medical records for biomarkers used to assess kidney function, and assessing the patients’ knowledge-based regarding dietary phosphate control, as well as adherence to phosphate binders’ usage.
Results: Out of 237 included patients, male to female ratio was 54:46. The prevalence of prescribing non-calcium phosphate binders was 82.7% whereas prescribing calcium phosphate binders was 73.8%. A total of 63% of patients showed a medium level of adherence to phosphate binders. Although adherence level was not poor, therapeutic efficacy was affected by other factors such as administration time adherence positively correlated with the serum phosphate level (p=0.00).
Conclusion: Phosphate binders usage is frequent among hemodialysis patients in Qassim centers. Circulating phosphate level was affected by the extent of patients’ knowledge of dietary control and adherence to the usage of phosphate binders. Thus, we recommend enhancing patient education in reference to high- and low- phosphate-rich diet to take wise dietary decisions, lower pill burden, and improve adherence toward the control of hyperphosphatemia
Chronic kidney diseases (CKD) represent a burden on the Saudi Health Care system; overall, CKD has shown an increasing prevalence.1-3 According to the Saudi Center of Organ Transplantation 2016 report, the number of patients dependent on dialysis in Saudi Arabia is rising annually and estimated to exceed 20,000 patients by the end of 2020.4 The knowledge of the pathogenesis and treatment of CKD mineral-bone disorders (CKD-MBD) had grown considerably. The diagnosis, prognosis, and management of these disorders are now formally systematized according to specific Kidney Disease: Improving Global Outcomes (KDIGO) guidelines.5
Observational studies have revealed that patients with significantly higher serum phosphorus, calcium, and parathyroid hormone (PTH) levels have a higher mortality risk than those with lower levels.6,7 In Gulf Cooperation Council Countries (GCC) participation in the international dialysis outcomes and practice patterns study (2012-2015), showed that serum level were not different from the other international readings described by the other countries involved by the study, but it was noticed that results for PTH level were higher than other participants. Thus, the control of serum phosphorus is considered a critical factor in improving the clinical outcomes in CKD-MBD, including survival.8,9 Moreover, hyperphosphatemia represents a significant cause of morbidity and mortality in hemodialysis patients, as phosphate is not effectively removed by dialysis, the patients are required to follow a protein-restricted diet to decrease phosphate consumption.10 Oral phosphate binders are required by the majority of patients on hemodialysis, which are agents used to control serum phosphate levels through different action mechanisms, but the net result is to prevent gastrointestinal phosphate absorption.11 Highly efficient aluminum-containing agents have been used but are associated with the risk of aluminum toxicity, which suggests doses monitoring, and hence, are no longer widely used. Further, calcium-based salts are also used, and they have the advantage of being cost-effective. In the past, they had been utilized as first-line therapy agents for the control of phosphate absorption, but due to its association with hypercalcemia and vascular calcification, they have been related poor prognosis with no difference in all-cause mortality rates, compared to other agents. Therefore, considering the widespread use of these salts has been an issue of concern.12,13 Sevelamer hydrochloride (calcium and aluminum free) is indicated to control serum phosphorus in patients with end-stage renal disease (ESRD), and it is useful when administered concurrently with vitamin D to reduce the potential occurrence of hypercalcemia and to minimize the progression of coronary artery calcification. Thus, it is not advisable to manage it as single-drug therapy. This was observed after treatment of hemodialysis patients with sevelamer for 6-12 months, in comparison with patients treated using calcium carbonate or lanthanum carbonate, another nonaluminum, and calcium-free phosphate binder. The study found that the degree of the reduction in hyperphosphatemia appeared to depend more on patient acceptance and tolerance than on differences in phosphate-binding capacity.14
Unfortunately, all phosphate binders are associated with poor patient adherence, and the reasons differ depending on each patient. Nonetheless, the common reasons include patients’ lack of understanding of their condition and treatment, cost of treatment, and the possibility that physicians might prescribe higher doses to improve reduced efficacy, with a consequence poor patients’ adherence, attributable to a high level of pill burden.15 Studies assessing phosphate binder usage, especially in the Qassim region in Saudi Arabia, is limiting. Meanwhile, the number of hemodialysis patients is continually increasing. Accordingly, we aimed to assess phosphate binder usage among the Qassim ESRD patients undergoing kidney hemodialysis and to evaluate the factors affecting the therapeutic efficacy of phosphate.
Methods
A prospective cross-sectional study was conducted among hemodialysis patients attending 4 dialysis centers across the major cities in the Qassim region for 3 months from November 2018 to January 2019. With an assistance from the Biostatistics Department, the dialysis inclusion patient’s entry was calculated to be 237 using Raosoft®, Inc. software at a 5% margin of accepted error and a 95% confidence interval. Ethical approval was obtained from Qassim Research Ethics Committee. The study was conducted following the ethical principles outlined in the Declaration of Helsinki. Written informed consent was provided by all participants.
Inclusion criteria were as follows: only ESRD patients receiving regular hemodialysis 3 times per week for at least 3 months who were stable, oriented, and age more than 18 years, and those who did not meet the inclusion criteria were excluded.
A simple, convenient sampling method was followed. Patients were guided through a face-to-face interview to complete a structured data sheet adopted from the literature. The questions were tested and revised by a specialist and internal consistency was assessed using Cronbach’s alpha (0.8). The question was translated into Arabic and then translated to English. The first set of questions was to determine the general characteristics of participating patients. Patients were divided into phosphate binder users and non-users depending on whether the use of phosphate binders or not was included in their treatment regimen. Patients were classified according to the dependence on the number of correct answers to the questions concerning rich phosphate dietary content. A patient score of 11-7 was designated as having a good knowledge level, while a patient scored 7-4 was designated moderate knowledge level, and 0-4 had a poor knowledge level.
Moreover, adherence to phosphate chelating therapy was assessed indirectly by patients’ responses regarding questions on commitment to dose and time of administration of the drug. After that, the record of each patient was checked and reviewed the serum phosphate levels. According to the serum phosphate means, patients were categorized into 3 groups of high, medium, and low levels of adherence. Moreover, means of PTH, hemoglobin (Hb), and serum albumin level were calculated and recorded. The last set of questions was assessing the factors that might affect the efficacy of phosphate binders, including the time of administration in regard to meal and number of tablets administered per day.
Statistical analysis
Descriptive statistics were applied using coefficients of the summarized data set. Relative frequencies and percentages were used to summarize categorical variables. Cross tabulation and nonparametric correlations to determine associations between groups (Spearman’s test), as our data did not follow the typical normal distribution. Statistical Package for Social Sciences, version 21 (IBM Corporation, Armonk, NY, USA) was carried out for all statistical analyses.
Results
Of the 237 interviewed patients, were male (54%, n=128), while female represents 46% (n=109). The mean age was 52.15 (SD=15.004) years, with a mode of 60 years. The majority of the patients were married (66.7%, n=158). Most of the patients’ educational level was high school or less (54.4%, n=129), followed by illiterates (28.7%, n=68). Hypertension and diabetes mellitus (42.6%, n=101) were the most common comorbid conditions reported by the patients (30%, n=721 and (3.8%, n=9), respectively (Table 1). The prevalence of prescribing non-calcium- versus calcium phosphate binders among the included patients was 82.7% versus 73.8%. Of those on non-calcium phosphate binders, 76% were on calcium therapy.
Demographic data of study participants (N=237).
Out of the interviewed patients, 78.5% (n=214) had serum phosphate levels within the normal range. Regarding the knowledge of dietary control and phosphate binders usage, 58.6% (n=139) of patients scored poor knowledge level, whereas 24.5% (n=58) had moderate knowledge, and only 16.9% (n=40) showed good knowledge. We found that 80% (n=112) of patients, displayed normal phosphate levels, reported as having poor knowledge on dietary phosphate control and phosphate binders’ usage among the participants, and 55% (n=20) patients showed low serum albumin level followed free phosphate meal. Regarding patients’ Hb levels, most of the study participants recorded a ranged from >11.1-12 mg\dL.
Out of the 237, 64% (n=152) showed high levels of parathyroid hormone that exceeds 300 pg/mL. Of these levels, 28.3% were more than 800 pg/mL lower. We found than 28.3% (n=67) was reported lower than 300pg/mL and 4.8% of these showed less than 100pg/ml.
Majority of patients (89%, n=211) gave the wrong answer in response to the question regarding phosphate binders effect on the absorption of other drugs when co-administered at the same time, and 32% (n=76) of patients had no knowledge that phosphate binders should be administered separately from other medications. Further, 64% (n=152) of patients taking phosphate binders tablets with meals had a normal range of serum phosphate levels in their records.
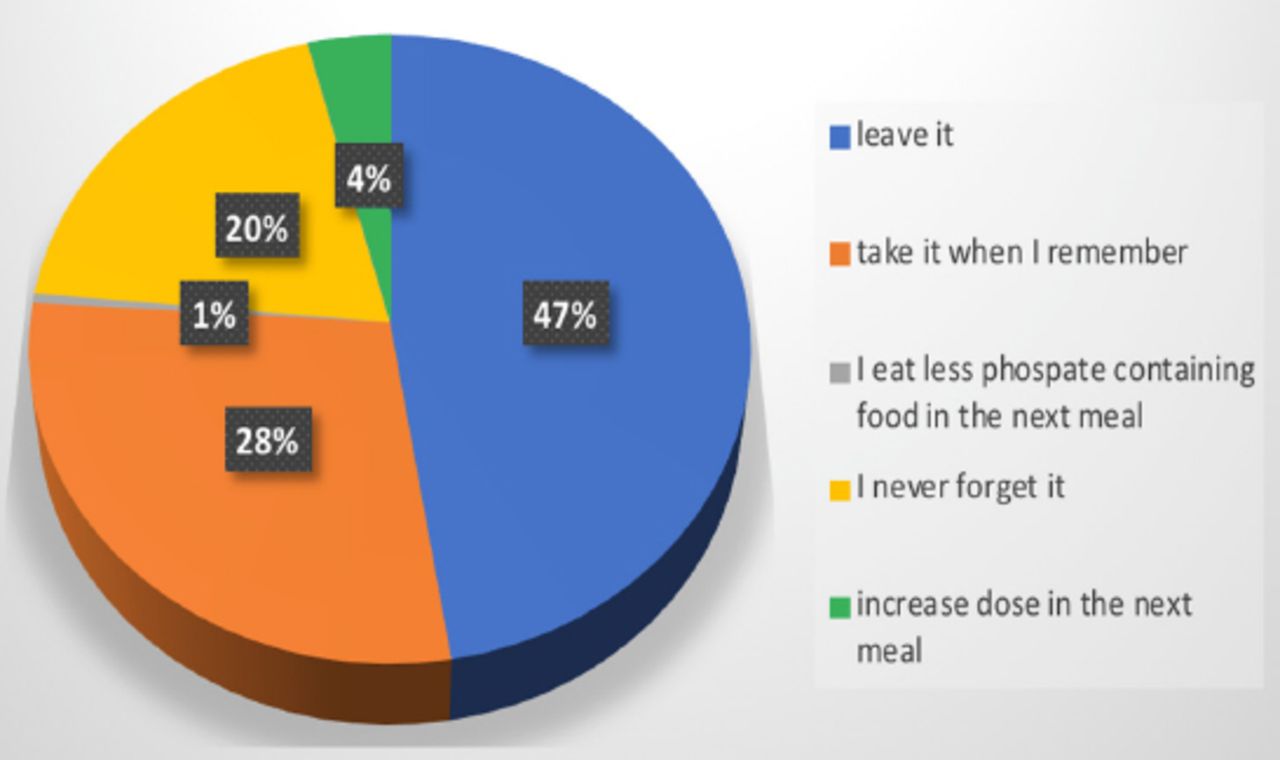
Out of the total participants, 55 of those responded as having medium adherence to phosphate binder usage, 23% had very high PTH level (>800 pg/ml), while 13% with a high level of adherence also had elevated serum PTH levels (501-800 pg/ml). Nearly 64% (n=152) of patients were taking phosphate binders tablets with food and had phosphate levels recorded within the normal range. Only 7% (n=17) of those who took >6 tablets per day had a medium level of adherence. The participants’ attitudes toward a missed dose of phosphate binders showed that 47% (n=111) ignored it and took no action (Figure 1).

Participants’ attitudes when missing a dose of phosphate binder.
A Spearman’s non-parametric test was applied for the correlation between the phosphate binders and other variables. It revealed a positive significant correlation with the serum phosphate (p=0.00) knowledge of dietary control (p=0.001). There was a strong, positive correlation between phosphate serum level and the number of phosphate binder tablets administered, which was statistically significant (p=0.003). A statistically significant negative correlation was observed between phosphate serum level and the use of phosphate binders, which was significant (p=0.000). Further, a negative correlation existed between serum PTH level and the use of phosphate binders (p=0.023).
Discussion
The K/DOQI and KDIGO guidelines suggested phosphate binder’s usage for the treatment of complicated CKD to maintain normal serum phosphate levels. It also recommended that calcium-based binders should be dose-stopped in case of hypercalcemia, arterial calcification, progressive bone disease, or fall in serum PTH concentrations that are less than 2 times the upper reference laboratory range.5
Patients’ demographic and clinical characteristics profoundly affect their knowledge and adherence to phosphate hemodialysis medications. Out of the total patients included in the study, more than half (54%) has a median age of 52.15 years. The median age of patients enrolled in our study was lower than what was reported by some countries stated in the Dialysis Outcomes and Practice Patterns Study (DOPPS) of the GCC such as Kuwait and UAE, quite similar to median age reported in Saudi Arabia.16 This study, young age group might justify the good adherence as it decreased the chances for the presence of polypharmacy among patients. Polypharmacy has been identified as a geriatric-related syndrome.17 However, this study found that hypertension and diabetes mellitus (42.6%, n=101) were the most common comorbid reported by the participants and its high level is consistent with what was reported in GCC DOPPS. They reported that 41% of hemodialysis patients in the GCC were diabetics and 29% were hypertensive.18 The association of ESRD with other diseases acts as additional non-adherence leading factors were due to polypharmacy. One of the limitations of the study was we did not assess the number of administered drugs associated with treatment non-adherence.17
The majority of our participants were males (54%, n=128) and married (66.7%) compared to the GCC DOPP study finding (2012-2015) which showed 71% of married patients were from Saudi Arabia and male predominance.16 The social status of being married can add additional support to the participants enhancing their commitment to therapy through social support and follow up. We found that most patients had low level of education (illiterate, high school, or less), as reported by Lim et al.19 This was expected, as illiteracy or low level of educational development has been linked with chronic renal failure.20 We found a high percentage of prescribing phosphate binders among our participants for non-calcium phosphate binders (82.7%) and for calcium based binders (73.8%). This result was in the same range of what had been reported in GCC (81%).9 More than two-thirds of non-calcium phosphate binder users (76%) are co-administrating with calcium binder. Calcium phosphate binders were considered as the first option to treat hypocalcemia accompanying hyperphosphatemia, adding a non-calcium containing phosphate binder is the choice to control the adverse effect of progression of vascular calcification in hemodialysis patients who are only taking calcium carbonate prescribed in higher doses.21,22
The level of knowledge reported by our study was similar to what has been reported previously.19 The possible reasons for patients’ superficial knowledge on phosphate dietary control and phosphate binders include patients’ difficulty in understanding the complexity of the role of minerals and electrolytes, and their interactions in the body. Additionally, the availability of media information regarding phosphate binders is lacking. Thus, patients’ limited understanding likely benefits in lowering serum phosphate level is attributable to a combination of inadequate educational programs, pharmacist counseling, as well as meager media advertisement or conveying a message on the matter. All of which are likely to affect patient’s knowledge toward the use of phosphate binders. However, we noticed that 80% (n=112) of patients, displayed normal phosphate levels, reported as having poor knowledge on dietary phosphate control, and phosphate binders’. We can point that such kind of adherence reflects patients commitment to treatment with phosphate binders, which was not built on knowledge base on phosphate dietary control and factors affecting phosphate binders efficacy.
Restriction of proteins to control phosphate levels might harbor negative prognostic consequences on a patient’s nutritional state and the consequence of the development of complications. We found that most of the patients were following a restricted phosphate diet, thus they had developed low albumin levels and hemoglobin levels not exceeding 11 mg/dl, in agreement with what was stated in the literature.23,24
We envisioned that adherence to phosphate binder is a challenge for many ESRD patients, and might correlate with different factors. We evaluated patients’ adherence through assessment of serum phosphate levels, which showed that most of the study participants had a moderate level of adherence.
In 4 centers involved with our study, 38% of the subjects were adherent to the prescribed phosphate binder therapy, and serum phosphate level was above 5.5 mg/dl in 39% of the participants with a significant direct relationship between serum phosphorus levels and pill burden from phosphate binders consistent with previous studies reported adherence pill burden, and patients’ life quality (QOL) relative to hemodialysis Please rephrase and clarigy.25-28
Moreover, there is a considerable variability among studies that explain different methodologies used to measure adherence (such as self-reports, the serum phosphorus level, pill counts, and others) and various definitions of adherence.25-28
Concerning the laboratory variables, we noticed that PTH level was very high in patients with moderate and good adherence. Patients below the upper limit (300 pg/ml) were 23.8% (n=67); this upper limit was reported by 71% of the centers enrolled in the DOPPS involving GCC.9
Our sample showed a high level of parathyroid hormone (64% [n=152]) consistent with the DOPPS study, which reported high median parathyroid level in Saudi Arabia (523 pg/ml) compared to the GCC average (452 pg/ml) this results are considered higher than results in Japan and Europe. Out of patients below upper limit, 4.8% (n=13) of patients showed levels of parathyroid hormone that considered as low bone turnover and required further assessment and treatment.29
Patients with higher phosphorus levels seemed to be more adherent if investigations of serum phosphorus level and adherence were carried out at the same time. Higher PTH levels were also linked with non-adherence, which, most likely, indicate secondary hyperparathyroidism as a complication of persistent higher measurements of phosphorus in these patients.25,26 These findings support the need for new individualized scales for phosphate binders, including factors that might affect therapeutic efficacy. Moreover, a more intensive dietary education concerning phosphorus intake in this population would be highly desirable.
The most common reasons for non-adherence among hemodialysis patients were found to be suffering from side effects, forgetfulness, high cost, and challenging, complicated regimens.30 In this study, factors affecting patients’ adherence included the time of administration. We found that the majority of patients who were taking phosphate binder tablets with food had a normal range of phosphate levels. Ghimire et al30 found that the prevalence of medication nonadherence varied from 12.5% to 98.6%. Medication-related factors such as the number of daily tablets, total pill burden, number of phosphate binders administered, which shows that increasing bill burden decreases the level of adherence, and complexity of medication regimen were also associated with poor adherence.30 However, we noticed that a small number of patients with high bill burden and a medium level of adherence, emphasizing that bill burden might affect patients’ level of adherence to their prescribed medications.31
A qualitative study was conducted in Australia regarding factors related to medication adherence in ESRD, and it was reported that economic restrictions had contributed to medication non-adherence. Also, low socio-economic status has been ominously associated with medication non-adherence among renal failure patients. In developing countries, most of renal failure patients have inadequate access to health insurance, and hence, medical care for ESRD patients becomes expensive. Subsequently, this affects adherence to the treatment regimen.32
In this study, we did not evaluate the implication of patient’s financial status relative to adherence since the government of Saudi Arabia covers the cost of treatment and ensure the availability of medications.
Study limitations
First, this study had a drawback in the cross-sectional design, being unable to detect the causal relationship between variables and the short duration of the study might affect results assessment. Second, the patient’s group was not a full representation of all patients on hemodialysis in the region, as they were recruited from the centers in Qassim only.
We evaluated the relationship between clinical markers, including phosphorus, calcium, PTH, hemoglobin and albumin, and the level of patients’ adherence, but we were unable to assess the relationship between the level of vitamin D and adherence, which would have been useful. In addition, we did not considered the effect of missing dialysis doses and it was not assessed in our study what might affect the result.33
Our current study, however, has many strengths that could be highlighted. First, the study was undertaken across 4 dialysis centers, and the representative sample size was recruited. Second, our study had the advantage of obtaining 2 measures of adherence (a clinical measure of serum phosphate and self-reported adherence scale), which was influential in measuring and establishing a strong correlation between variables and reassuring that the measurement of adherence was reliable.
In conclusion, phosphate binders’ usage is frequent among hemodialysis patients at Qassim centers. Although the adherence level was not poor, therapeutic efficacy was affected by other factors such as administration time. Also, we noticed that the patients elevated serum phosphate level was affected by the level of dietary control.
Furthermore, our recommendations that should aid in controlling hyperphosphatemia are as follows: First, improving patients’ knowledge to abstain from the phosphate-rich diet by establishing patients’ educational and counseling centers in the hospitals equipped with suitable related materials, media involvement, online educational links, and audio-visual aids for teaching hemodialysis patients how to adhere to the prescribed regimen, are likely to support adherence, and in turn, lower pill burden. Second, through education and counseling, patients at the beginning of pre-dialysis would get the support needed to identify existing coping strategies interventions provided to improve such health-related issues. Third, developing specific and powerful tools for adherence assessment might apply to patients’ populations undergoing hemodialysis. Finally, it would be beneficial to investigate a patient’s preference regarding prescribed drugs to enable the achievement of adequate adherence to treatment.
Acknowledgment
The authors gratefully acknowledge Enago (www.enago.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 8, 2020.
- Accepted August 29, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.