


Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42844.
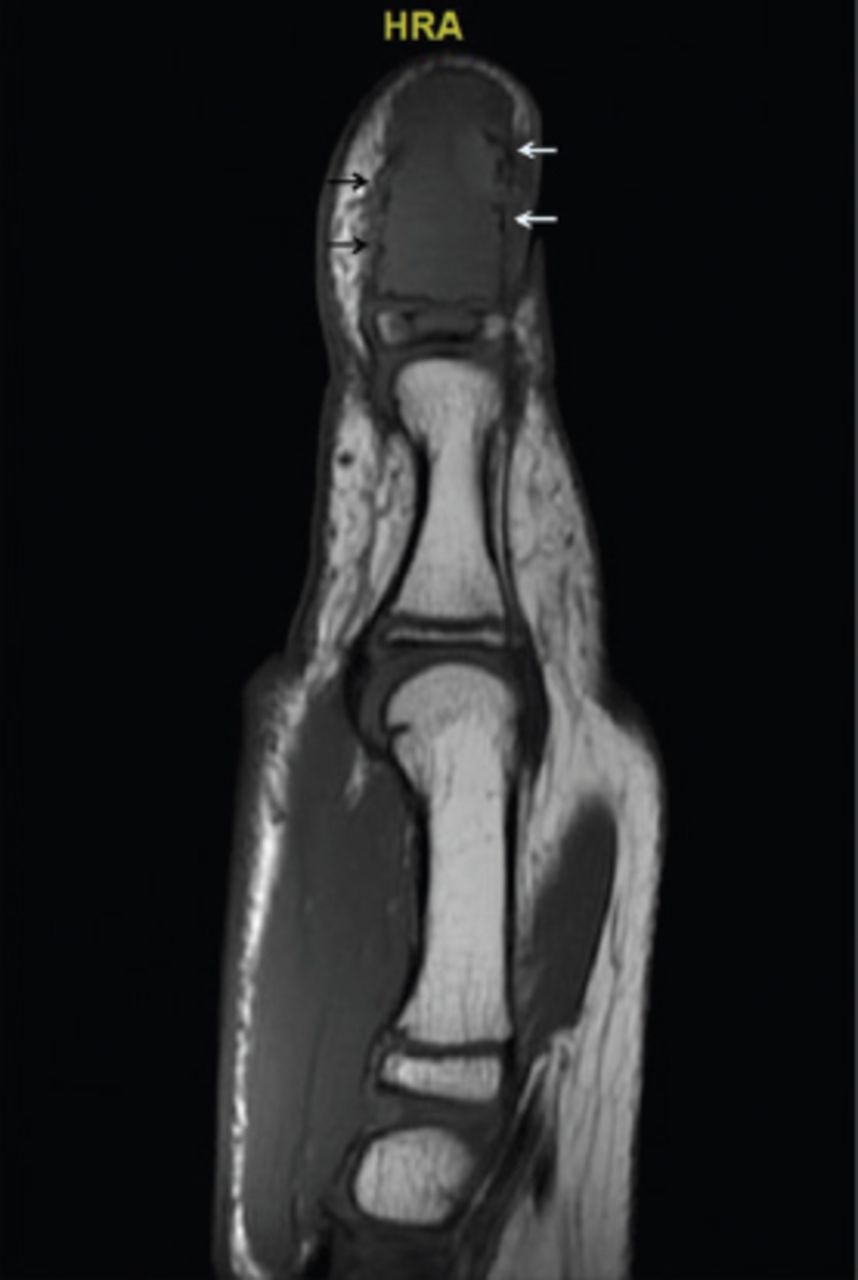
The patient was a right-handed, 12-year-old boy, who was known to have hemophilia A. He was not on regular treatment. He had a history of local swelling of the left thumb distal phalanx for 2 months with no history of trauma. Mild deformity was noticed, with limitation of the distal thumb movement. There was no laceration, discharge or tenderness. Examination of the right hand was normal. The other musculoskeletal examinations and the surgical history were unremarkable. A simple hand x-ray showed an expansible lytic bone lesion with prominent internal trabeculation (Figure 1). Magnetic resonance imaging of the present case showed a cortical break, volar bulging and a complicated hemorrhage that was associated with a fluid-fluid level and internal septations (Figure 2). Then, he was admitted for enucleation of the left thumb cystic lesion and curettage with a bone allograft. After incision and dissection, the bony cystic lesion was found to involve the whole bulb of the thumb, extending to the middle of the distal phalanx of the thumb. It extruded through the volar and dorsal cortex to the growth plate. The received curetted fragments from the bone cystic lesion appeared under microscopic examination to be blood-filled, variably sized cysts (Figure 3). These cysts had no cell lining and their walls contained bland fibrous tissue. He was followed up post-operatively for 18 months; there were no complications or recurrence (Figure 4).

X-ray of left hand pre-operatively.
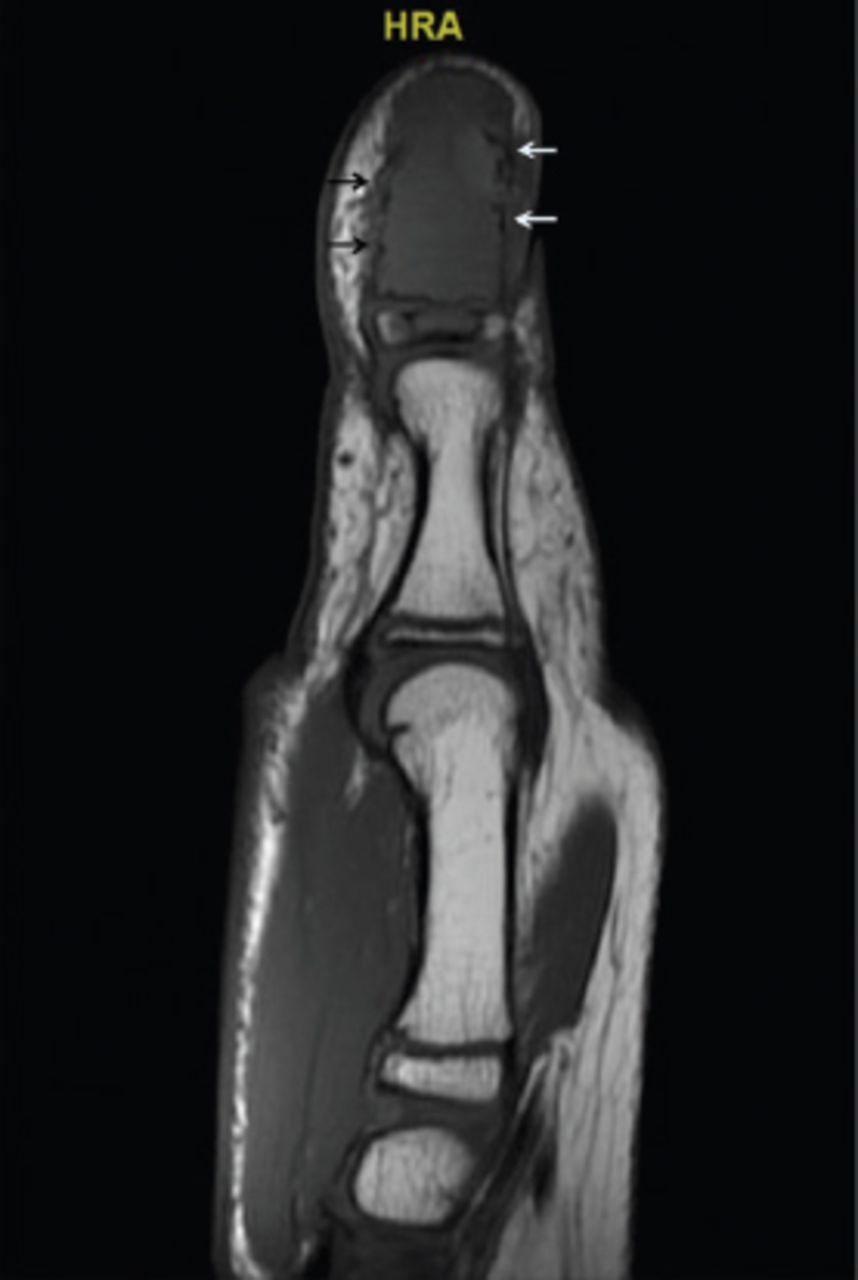
Magnetic resonance imaging of left thumb pre-operatively.

Microscopic view of a hemorrhagic cyst.

X-ray of left thumb 18 months post-operatively.
Question
What is the most likely diagnosis?
Aneurysmal bone cyst (ABC)
Pseudotumor of hemophilia (PTH)
Osteosarcoma
Giant cell tumor
Answer
2. Pseudotumor of hemophilia (PTH)
Discussion
Pseudotumor of hemophilia (PTH) is also known as a hemophilic cyst. Pseudotumor of hemophilia is a hematoma inside a fibrous capsule that expands in size after recurrent bleeding. It was first described in 1918 by Starker in the case of a 14-year-old boy with known hemophilia who presented with a right femur subperiosteal hematoma that had been thought to be an osteosarcoma. Pseudotumor of hemophilia is rare complication in hemophilic patients, occurring in 1-2%. It almost always occurs in hemophilic patients with factor VIII or IX deficiency; to date, only 3 cases have been reported in non-hemophilic patients.1 It is categorized into an osseous or soft tissue lesion based on its anatomical location. Most cases of osseous pseudotumor are seen in the femur, pelvis, tibia and bones of the hand, while soft tissue pseudotumors are mostly associated with the iliopsoas, quadriceps, triceps surae and gluteus muscles. Depending on its origin, PTH can be classified as true when it presents as interosseous bleeding or false when it presents as a muscular hematoma. Pseudotumor of hemophilia of the thumb is a very rare condition, with only one case reported in the literature.
The clinical presentation of patients with PTH varies widely depending on the anatomical location and adjacent structures that are affected by compression of the expandable hematoma. The rate of bleeding can also play a major role in whether there is a rapid or slow clinical presentation. An osseous pseudotumor can present simply as a painless cystic lesion or severely as a bone fracture and joint dysfunction.2 In contrast, soft tissue pseudotumors can lead to skin necrosis and neurovascular compromise by mass effect.3 In the current case, the presentation was a painless distal thumb swelling that become painful a few months after the first visit, which may have been due to acute internal bleeding.
Multiple modalities of imaging can be used to help in the diagnosis of PTH, with MRI being the most useful. On a plain radiograph, a lytic cystic bone lesion with a dense line representing hemosiderin pigmentation is usually seen, but these features are non-specific for PTH and can be seen with other differential diagnosis such as benign, malignant and infectious bone lesions. In the present case, a simple hand x-ray showed an expansible lytic bone lesion with prominent internal trabeculation (Figure 1). An x-ray should be followed by CT or MRI; biopsy of a pseudotumor is absolutely contraindicated.4 Both CT and MRI can show the fibrous capsule with an internal hemorrhage with a fluid–fluid level. Computed tomography is efficient at detecting bone destruction and soft tissue lesions including daughter cysts, while the number, size and extent of the lesion, neurovascular involvement and musculoskeletal deformities can all be determined accurately using MRI.1 Magnetic resonance imaging of the present case showed a cortical break, volar bulging and a complicated hemorrhage that was associated with a fluid-fluid level and internal septations (Figure 2). These findings can also be seen in ABCs.
The case histopathology report indicated the typical histopathology features of PTH, shown as a fibrous capsule with different levels of organization with bloody material inside, which can be associated with hemosiderin in the case of chronicity. In our case, ABC was a major differential diagnosis based on some of the radiological findings, although giant cells and osteoid and woven formations that are typical features of ABC were absent. Telangiectatic osteosarcoma and giant cell tumor were excluded due to the absence of malignant cells and giant cells. Molecular testing of the USP6 gene was negative, thus ruling out ABC.5
Due to the rarity and variety of PTH cases, the best management approach is not yet well established. Many approaches have been used, including surgical excision, radiation, embolization and conservation. However, surgical removal with or without a bone graft is considered by many reports as the treatment of choice for PTH. One report suggests that a center with a multidisciplinary surgical team is required for this procedure. In our case, surgical curettage and a bone graft were performed with no complications (Figure 4). The cyst was located in the distal phalanx of the left thumb, originating from the metaphysis and invading and destroying the growth plate, which necessitated the bone graft. In contrast, Issaivanan et al6 treated a case of thumb PTH by radiation and factor replacement. A conservative approach can be performed successfully with early presentation of osseous PTH. Embolization used to treat iliac bone PTH also had a favorable outcome.
In conclusion, PTH is a rare complication of hemophilia that is also seen in non-hemophilic patients. The clinical, radiological and histopathological features vary widely and require exclusion of differential diagnoses. Thus, each case of PTH should be managed individually.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.