


Abstract
Objectives: To examine the demographics and common presentations of pediatric coronavirus disease 2019 patients in the emergency department (ED), as well as their contact with positive COVID-19 cases, return visits, and patients’ disposition from the ED.
Methods: A retrospective chart review of confirmed cases of COVID-19 presenting to the Pediatric ED from March 2020 until June 2020 was conducted.
Results: Fifty-two patients were identified, with a higher frequency of male patients. Forty-four (85%) patients were discharged from the ED, and 8 (15%) required admission. Three patients were admitted to the pediatric intensive care unit and 2 died, resulting in a mortality rate of 3.8%. The most frequent presentations were fever (85%), cough (48%), and diarrhea (23%).
Conclusion: In our study, the second most affected system after the respiratory tract was the gastrointestinal tract, which was also the system responsible for the most return visits due to diarrhea. Coronavirus disease 2019 poses clinical and operational challenges given its variable clinical presentations.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a new pathogen that is responsible for coronavirus disease 2019 (COVID-19), which has led to a global pandemic in 2020. Since December 2019, SARS-COV-2 has been recognized as the causative pathogen of cases of severe pneumonia in the city of Wuhan in Hubei Province in China, which subsequently spread worldwide in a relatively short time. Severe acute respiratory syndrome coronavirus 2 appears to be primarily transmitted via respiratory droplets although aerosol droplets are another known route of transmission.2,3 Presently, conclusive evidence of vertical transmission of the virus from mother to fetus is lacking.4 Severe acute respiratory syndrome coronavirus 2 has been found in the stool of patients; however, the possibility of fecal-oral transmission is currently unknown. Most children with COVID-19 contract the disease because of close contact with infected patients. The incubation period ranges from 1 to 14 days, with an average of 3-7 days after exposure to the virus.6 Coronavirus disease 2019 primarily affects adults, with low numbers of pediatric patients being infected with SARS-CoV-2 worldwide. Accordingly, there have been thousands of reports for adult COVID-19, and limited reports for pediatric patients. However, this is not unique to SARS-CoV-2; indeed, the percentages of pediatric patients affected during the SARS-CoV-1 outbreaks were 6.9% and MERS-CoV were 2%.2 Based on the currently available evidence, pediatric COVID-19 accounts for 0.8%-2% of cases worldwide.2,3 On 20 January 2020, the first pediatric case of COVID-19 was reported in China, and on 19 February 2020, the first case of pediatric COVID-19 outside of China was reported in Korea. On 21 March 2020, the first pediatric case was reported in the USA, and on 24 March 2020, the first pediatric death was reported in the USA.7 Herein, we report on pediatric patients with confirmed COVID-19 presenting to pediatric emergency departments (PEDs) with various complaints, which are outlined, together with the patients’ demographics, disposition, and mortality. The aim of this study is to disseminate knowledge by adding a new piece to the current pediatric COVID-19 literature puzzle from emergency standpoint.
Methods
To locate prior related research, we searched the literature using the MEDLINE and PubMed databases, as well as articles identified from the references of the reviewed articles. We included only English language articles and excluded articles in other languages. We used the following keywords (MeSH) terms in our search:”Corona virus,”“COVID-19,”“SARS-CoV-2 in pediatric,”“Pediatric emergency.”
This was a retrospective observational study of all pediatric patients (0-14 years) who presented to PEDs with suspected COVID-19. We included children aged 0-14 years, presenting to our PED from 10 March until 20 June 2020, which was the period of lockdown in Saudi Arabia, who tested positive for COVID-19.
The study was approved by the Ethics Committee of King Abdulaziz University Hospital and was conducted according to the Declaration of Helsinki.
Our center is an academic tertiary hospital with an annual emergency consensus of 50,000 cases, 10,000 of which are pediatric, and it is one of 2 hospitals in the East Jeddah that offer free pediatric emergency services. We serve all pediatric emergency cases that are registered. From March 2020, the Ministry of Health distributed a national questionnaire that was used to initially assess the COVID-19 risk of every patient presenting to the ED (Appendix 1).
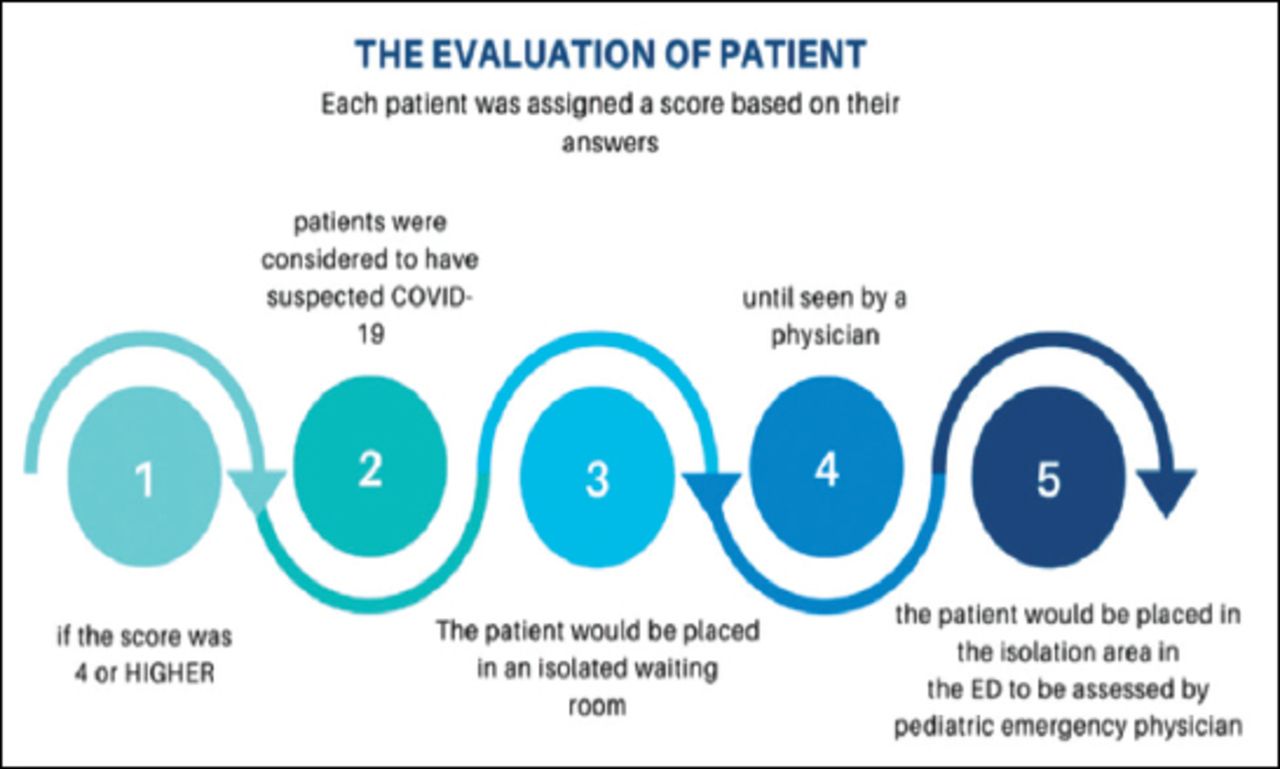
Each patient presenting to the emergency department with a COVID-19 of >4 will go through a pathway (Figure 1).

Pediatric emergency department (ED) patients process from presentation until seen by a pediatric emergency physician.
Demographic characteristics and medical data were obtained from the patients’ electronic medical records (EMRs), targeting their presenting complaints, presence of comorbid conditions, contact with a confirmed case of COVID-19, and complete blood count (CBC) results if available. All files were reviewed by a single person to retract the needed data from the EMRs.
The data was coded using Inductive coding method. For analyses of suspected infectious diseases, the coding of the following signs and symptoms were included: fever, cough, sore throat, tachypnea, vomiting and diarrhea and abdominal pain. The coding applied also on the questionnaires’ clause (exposure to contact information) choices and clinical diagnosis.
Statistical analysis
Microsoft office excel 2016 was used for statistical analyses. The descriptive statistic, frequencies and covariance tests were applied on the following data, demographic characteristics, symptoms and diagnosis.
Results
A total of 279 swabs of 267 patients were collected, and 64 swabs of 52 patients were found positive for SARS-CoV-2. There was a noticeable surge in positive samples obtainedin the last week of May and early June 2020.
All patients presented to our PED with family, and none were transferred via ambulance. The demographic results and clinical presentations of the included patients are summarized in Table 1.
Demographic features, exposure history, and signs/symptoms of the study cohort.
Forty-eight (92%) were healthy kids and 4 (8%) had chronic illnesses inform of congenital heart diseases and one had hydrocephalus with ventriculoperitoneal shunt complicated with seizure and developmental delay. Forty-four (85%) patients presented with mild disease and were discharged to home isolation. Eight patients (15%) were admitted because of moderate or severe illness. Three patients required pediatric intensive care unit (PICU) admission for respiratory failure;one patient died 36 hours after admission, secondary to the hyper inflammatory response; a second patient died 3 days after admission of multi organ failure secondary to viremia. Both deceased patients had chronic cardiac comorbidities. The third patient was discharged after spending 10 days in the PICU. Four patients were sent directly to quarantine dorms with family members who were also positive. Three patients were admitted to the hospital isolation units.Nine patients had CBC performed in the PED; 6 of whom showed normal counts, 2 showed leukopenia and lymphopenia, and one had leukocytosis.
A total of 12 patients returned to the ED within 48 hours for diarrhea (n=6; 50% patients), vomiting and abdominal pain (n=1; 8% patient), shortness of breath with normal saturation in the ED (n=2; 16% patients), decreased activity (n=1; 8% patient), and reduced intake (n=1; 8% patient); one patient (8%) returned to accompany a parent who was admitted to isolation (8%).
Five of the 12 cases with repeat visits to the ED contacted the COVID-19 team during the phone checkup, where they were asked to attend the ED for evaluation. Two of the patients returned because of worsening respiratory symptoms, one patient was admitted with their parent who was diagnosed with COVID-19 and admitted to the hospital isolation unit, and 2 patients were assessed before being sent to join their parents in the quarantine dorm.
Discussion
At the time of writing, based on the John Hopkins University Coronavirus Resource Center, there have been 7,653,993 globally confirmed cases of SARS-CoV-2, with 425,902 deaths. In Saudi Arabia, there have been 119,942 confirmed cases of SARS-CoV-2, and 893 deaths (0.7%). The ratio of pediatric patients ranges from 0.8%-5%.7,13
Saudi Arabia was one of the first countries to adopt early precaution measures to prevent the spread of the disease; this was achieved by implementing several policies and precautionary measures.
During the period of pandemic, the 2 holy mosques were closed. Partial and complete lockdown were implemented. Treatment was granted to everyone by a royal decree, including those with no privilege to specific health care sectors, such as illegal immigrants.8
The surge of positive swabs between the last week of May and early June may be explained by the decrease in social distancing because of the holiday season, during which, the government loosened the lockdown
The disease spectrum varies widely from asymptomatic cases to mildly symptomatic, moderate, and severe cases; thus, a diagnosis based on how patients first present to the PED is challenging, as symptoms can range from simple upper respiratory tract infections to pneumonia or full septic shock and hyper inflammatory responses.1 In the current study, we found that boys were more affected than girls (56% versus 44%), and the mean age was 6 years (one month - 13 years); these results were comparable to those of Lu et al9 in Chinese children with confirmed COVID-19. In our cohort, 4% of patients were asymptomatic, and all had positive contact with an adult with COVID-19, who was either one or both of the parents. Fever was the most common symptom for visiting the PED; fever was the presenting symptom in 85% of the patients in our study, and in 36%-54% of patients in studies reported in China and Italy.1,9 Thus, cough was the second most common complaint in our cohort after fever; this is not surprising, given that COVID-19 is a primary respiratory disease. In pediatric COVID-19 studies from China and Italy, cough was the second most common complaint, ranging from 44%-48.5%.1 Diarrhea was the third most common presenting complaint in our population, with 23% of children presenting to the ED complaining of diarrhea, and it was the most common cause of a return visit to the ED (50%). Sore throat, body aches, and vomiting were observed in 15%, 8%, and 8% of the patients, respectively. Furthermore, 4% presented with abdominal pain, and one patient presented with abdominal pain, fever, and vomiting with suspected appendicitis. This patient was initially examined using ultrasonography, which was inconclusive, and then followed up with computed tomography, which showed right lower quadrant lymphadenitis and terminal ileitis. Moreover, 4% of patients presented with shortness of breath or tachypnea on examination.
Despite the consensus that SARS-CoV-2 is a respiratory virus, it has important gastrointestinal manifestations (abdominal pain, vomiting, and diarrhea) as presenting complaints, which accounted for 35% of patients in our cohort. Moreover, 50% of the return visits were secondary to developing diarrhea. This was a peculiar observation in our cohort because diarrhea was not mentioned as a complaint in Qiu et al.8 Furthermore, Lu et al9 described 8.8% of his patients to have diarrhea but did not specify whether it was a presenting complaint or developed later during the disease course. In 2 other studies, diarrhea was mentioned as a complaint in 9.7%-15% of patients.10,13
Lu et al9 summarized the results of seven studies on the signs and symptoms in children with COVID-19 and found that fever presented in 33%-100% of the COVID-19 cohort population), whereas cough was found to occur in 6.7%-100% of cases.
Furthermore, a sore throat was described in 3 of the 7 studies, and it ranged from 5% to 40%.9 Headache was reported in one study, at a frequency of 9.7%;9 diarrhea was a complaint in 2 studies, ranging from 9.7%-15%; and tachypnea was reported in 2 studies, at a frequency of 10%-16.7%.10,12
These findings are similar to those of Ludvigsson et al11 on COVID-19 in the PICU, in which 83% of patients had significant pre-existing comorbidities, and there was a 4% mortality rate.
This was a novel study on COVID-19 in children, and their characteristics/outcomes from a PED point of view.
Study limitations
Compared to adult cases, the number of pediatric COVID-19 cases is small; therefore, there is a need for more pediatric emergency studies to gain greater understanding of the disease in children. This study can provide information regarding COVID-19 in children from emergency department prospective.
In summary, COVID-19 has a marked impact on the pediatric population. Although the number of infections is small compared to that in adults, it leads to PED visits with variable complaints. In our study, the second most affected system after the respiratory tract was the gastrointestinal tract, which was also the system responsible for the most return visits for diarrhea. Coronavirus disease 2019 poses clinical and operational challenges during peak periods of the pandemic given its variable clinical presentations.
Acknowledgment
I am grateful to the Saudi Society of Emergency Medicine (SASEM) and the Pediatric Emergency Section for their continuous support of emergency research across the Kingdom. I would like to thank Editage (www.editage.com) for English language editing.
Appendix 1 - Ministry of Health scoring sheet for suspected Coronavirus disease 2019 (COVID-19) patients.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 17, 2020.
- Accepted November 15, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.