


Abstract
Objectives: To determine the prevalence of vasculopathic diabetic foot and the associated factors in a Saudi tertiary center.
Methods: This retrospective chart review included adult patients (≥18 years) diagnosed with diabetic foot between May 2015 and July 2019 in King Saud University Medical City, Riyadh, Kingdom of Saudi Arabia. Based on clinical presentation and laboratory results, the patients were categorized into 2 groups namely, “vascular induced diabetic foot group” and “non-vascular induced diabetic foot group”.
Results: A total of 404 diabetic patients were enrolled in the study. The mean age of the patients was 62.03±12.30 years; 61.9% were males. Most of the diabetic foot cases had a non-vascular etiology (n=327, 80.9%), while 77 cases (19.1%) were due to vasculopathy. Patient in the vascular group had a significantly higher incidence of coronary artery disease (32.5% versus 14.4%; p<0.001), and a higher incidence of peripheral artery disease (PAD) in the unaffected limb (22.1% versus 2.1%; p<0.001).
Conclusion: Most cases of diabetic foot were due to non-vascular causes. Old age, history of coronary artery disease, or PAD in the unaffected limb were factors that were significantly associated with diabetic foot due to arterial disease.
Diabetic foot is a chronic serious complication of diabetes mellitus (DM). It has a worldwide prevalence of 6.3% and accounts for hospitalization in 4-10% of diabetic patients.1-4 Diabetic foot imposes a great challenge on the affected individuals, affecting both the mental and the physical health well-being.5 In addition, it also imposes a huge financial burden on both the individual and the national levels, with the largest contributors of cost being attributed to both hospital admissions and surgical procedures in managing patients with diabetic foot.6,7 Diabetic foot is the result of complex interplay between different components. These components include: disturbed metabolic and immune states, the presence of co-existing peripheral neuropathy and peripheral arterial disease (PAD).8-9 Peripheral arterial disease accounts for up to 50% of diabetic foot ulcers and acts as an independent risk factor for the development of these ulcers.10 The higher prevalence of PAD in diabetic patients is noted, with up to 11% of diabetic patients being affected when compared to 4% of non diabetics.10 In the Kingdom of Saudi Arabia (KSA), vasculopathy complications were found in 33.1% of patients presented with diabetic foot.9 At a prevalence rate of 2.41%, PAD accounts for the third most prevalent vasculopathy complication among these Saudi patients following coronary artery disease (23.6%) and cerebral vascular disease (10.2%). Moreover, PAD was more prevalent in diabetic foot cases complicated with foot ulcers with prevalence rate of 30% and amputations with 54%.9 On the other hand, the non-vascular risk factors also contribute to the development of diabetic foot. Most importantly, the presence of co-existing peripheral neuropathy. The combination of sensory and motor neuropathy will lead to both reduction in sensation and abnormal foot loading which will eventually lead to increased susceptibility to trauma and infections and thus, resulting in further increased risk of diabetic foot complications in addition to underestimation of the severity of the patient’s condition.11 It is important to mention that diabetic foot outcomes are mostly affected by the presence of PAD. However in most cases, it is difficult to allocate the exact underlying cause of a resultant complication as more than 60% of diabetic foot patients have a co-existing diabetic neuropathy. Thus, a combination of PAD and neuropathy is reported to be a leading cause of non-traumatic foot amputations.10,11 The impact of non traumatic lower extremity amputation is huge; with data showing that one year mortality rate following a major lower limb amputation to be 33-65% within 4 years. As for the patients who underwent minor lower extremity amputation, mortality rates at 1 was 18% and 4 years 45%.12 In the United Kingdom, over half of all lower limb amputations are carried out in diabetic patients, so prevention of such complications is mandatory.10 In the present study, the prevalence of vasculopathic diabetic foot and the associated factors in a Saudi tertiary center were determined.
Methods
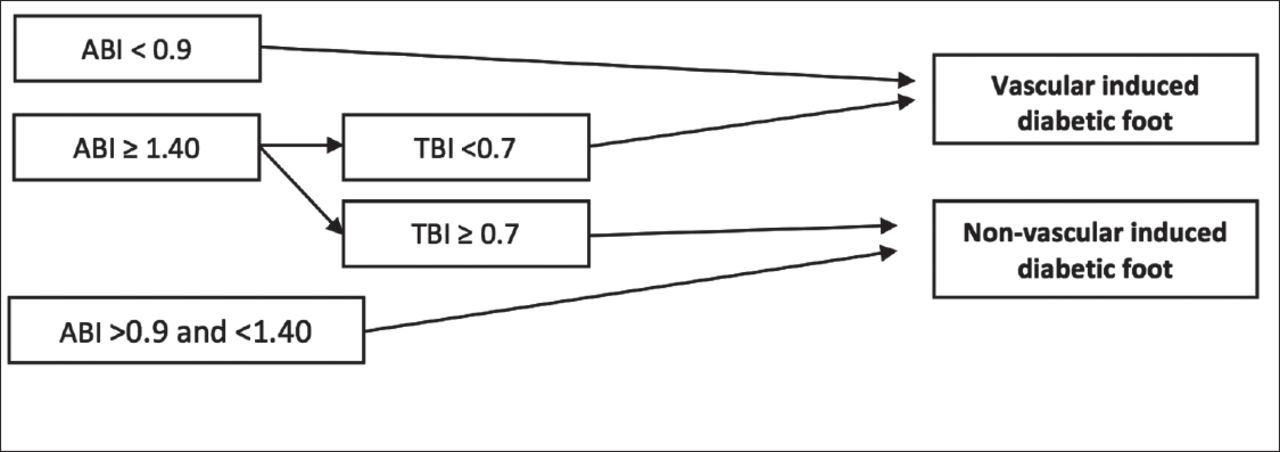
This is a retrospective chart review and was performed on collected data pertaining to diabetic foot patients, that were maintained in the database of King Saud University Medical City, Riyadh, Kingdom of Saudi Arabia (KSA). This study included all adult patients (≥18 years) who presented to the emergency room (ER) with diabetic foot and were admitted to the in-patient service or followed up in the outpatient clinic at King Saud University Medical City, Riyadh, KSA, during the period between May 2015 and July 2019. A list of all patients diagnosed of diabetic foot, cellulitis in diabetes, and gas gangrene was retrieved from the database. The list included 595 patients of which 191 patients were excluded from the study due to incomplete documentation or refusal of further examination and investigation. This study was approved by the Institutional Review Board Committee of King Saud University. The confidentiality of the patients was ensured by assigning each patient a number code for the purpose of reference and statistical analysis; the codes were only accessible to the authors. Patient demographics and risk factors for diabetic foot were collected and included age, gender, route of admission, duration of diabetes, blood sugar level, type of diabetes medications the patient was on, other complications associated with diabetes, history of previous foot ulcers, and history of foot deformity. Random blood sugar level of the patient was measured upon arrival. Based on the clinical presentation and laboratory results, the patients were categorized into 2 groups namely, “vascular induced diabetic foot group” and “non-vascular induced diabetic foot group. An ankle-brachial index (ABI) p>0.9 and p<1.40 was considered normal; p-values ≥1.40 implied the presence of calcified incompressible vessels. Vasculopathy was diagnosed in the affected limbs when there was an absence of pulse with low ABI (p<0.9) or a low toe brachial index (p<0.7) (Figure 1).13

Illustration of peripheral artery disease diagnosis using non-invasive diagnostic methods. ABI: ankle-brachial index, TBI: toe-brachial index
Ankle-brachial index and toe-brachial index (TBI) techniques
a) Appropriate blood pressure cuff size for both the ankle and the arm was selected. b) Patient was put in a quiet room on decubitus position with the arm and ankle at the same level as the heart, for a minimum of 10 minutes before measurements. c) Cuffs were set comfortably in place, adjusted to the arms at the same level above the cubital fossa and directed toward the brachial artery on each side. d) Ultrasound gel was put in the antecubital fossa and the handheld doppler was placed on the gel. e) Cuffs were deflated until doppler no longer detects signals. f) Systolic blood pressure (SBP) in the upper limbs was recorded and annotated, the arm with the highest blood pressure was selected in order to confront its result with the lower limb. g) Cuffs were placed immediately proximal to the malleoli or on the big toes (in TPI measurement), then the ultrasound gel and doppler were placed on the dorsalis pedis and the posterior tibial arteries pulses. h) Cuffs were deflated until doppler no longer detects signals. ix) Systolic blood pressure in the lower limb was recorded. i) Calculation of ABI based on data obtained by using the formula: highest pressure in foot/highest pressure in arms. g) When the results of upper limbs and lower limbs were identical, the right limbs were chosen. All examinations were performed by experienced technicians who did not participate in the study and were reviewed by vascular surgeons.
All patients were advised a basic standard of care. In case of dissent from patients, they were asked to sign a form indicating their discharge against medical advice under their responsibility.
Statistical analysis
Descriptive statistics was performed using the Statistical Package for Social Sciences (SPSS) statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). The frequencies and percentages of all nominal variables and the mean and the range for all measurable variables were calculated. Student’s t-test was performed for comparisons between the vascular induced diabetic foot and non-vascular induced diabetic foot groups for all measurable variables, while the chi-square test was used for all nominal variables. A p-value<0.05 was considered significant.
Results
A total of 404 diabetic patients were enrolled in this study of which 11 patients had diabetic foot in both the limbs. Therefore, a total of 415 limbs with diabetic foot were included in this study. The demographic characteristics of the patients are shown in Table 1. The mean age of the patients was 62.03±12.30 years and 61.9% of them were males. A majority of the patients (76.7%) presented through the ER of the hospital. More than half (56.7%) of them were diagnosed with DM of an unknown duration. Among those with DM of a known duration, 17.3% had the disease for more than 20 years. Twenty-four (5.9%) patients had a history of foot deformity and 22.3% had a history of diabetic foot. More than one-third (36.9%) of the patients were free from other microvascular and macrovascular diabetic complications. However, nephropathy accounted for the most frequent complication in 95 patients (23.5%). Insulin was used as the anti-diabetes medication in 196 (48.5%) patients. The mean blood glucose level was 13.00±6.23 mmol/L (normal blood glucose level is <11.1 mmol/L) and the mean glycosylated hemoglobin (HbA1c) level was 9.81±2.28% (normal HbA1C level is <5.7%; prediabetes level is 5.7-6.4%).14
Patients demographics.
As shown in Table 2, a majority of the cases of diabetic foot were of a non-vascular cause (n=327, 80.9%), whereas only 77 cases (19.1%) were of a vascular cause, of them 28 limbs (6.75%) were having calcified incompressible vessels (p≥1.40). The patients with diabetic foot of a vascular etiology were significantly older than those of a non-vascular etiology (65.17±10.68 years versus 61.29±12.56; p=0.013). Moreover, other diabetic complications such as history of coronary artery disease and PAD of the non-affected limb were more frequent in the group with a vascular etiology (32.5% versus 14.4%; p<0.001) compared to those with DM of a non-vascular cause (22.1% versus 2.1%; p<0.001). However, there were no significant differences between those with diabetic foot in either groups in terms of gender (p=0.866), route of presentation (p=0.275), duration of diabetes (p=0.197), history of foot deformity (p=0.066), history of diabetic foot (p=0.140), blood glucose level (p=0.097), and HbA1c (p=0.701) or in terms of other diabetic complications such as retinopathy (p=0.804), neuropathy (p=0.136), nephropathy (p=0.144), or stroke (p=0.066).
Factors distribution between vascular and non-vascular caused diabetic foot ulcer.
Table 3 is indicative of the significantly higher number of limbs managed by wound care (cleaning the wound with saline, dressing, debridement in the clinic, and application of antibiotic ointment) in patients in the non-vascular group compared to those in the vascular group (50% versus 17.7%; p<0.001). Nevertheless, amputations were significantly more frequent in the group with a vascular cause compared to that with a non-vascular etiology and included toe amputation (32.9% versus 13.3%; p<0.001), below knee amputation (20.3% versus 12.4%; p<0.001), and above knee amputation (8.9% versus 2.5%; p<0.001). Two limbs among patients in the vascular group and 8 limbs among those in the non-vascular group were not managed in the hospital due to shortage of beds; 2 limbs from the non-vascular group were managed by incision and drainage of the big toe and intravenous antibiotics.
Management of diabetic foot ulcer.
Discussion
Diabetic foot and the related complications ranging from ulcer formation to amputation is affecting the lives of diabetic patients. An estimated lifetime risk of having a diabetic foot ulcers in these patients is 25%. Of these foot ulcerations, 20% will lead to lower limb amputation.15 These ulcers can be classified as: purely ischemic, purely neuropathic or mixed neuroischemic ulcers. It is to be noted that purely ischemic ulcers are seen in only 10% of these diabetic patients.16 Diabetics are more likely to suffer from atherosclorotic vesseles, which affect the blood supply and tissue perfusion of any given area and hence in the periphery, can result in ulcer formation. It has been reported that PAD contributes to 50% of all ulcers seen in diabetics whether in the form of a pure ischemic or combined neuroischemic ulcers.17 In a population-based study in KSA, PAD contributed to 30% of diabetic foot ulceration (DFU).10 In our study, it was found that only 19.1% of our patients were found to have vascular induced diabetic foot (all types of diabetic foot complications; DFU, gangrene and amputation), which is considered low when compared with what was found in the other studies that were carried out in the Westren countries.16-18 In addition, in a study that was carried out in Jeddah, KSA, it was found that 15.4% of patients who presented with DFU had mixed peripheral arterial disease and peripheral neuropathy and none of the rest of patients presented solely with peripheral arterial disease.19 This is in contrast with what was found in the West with peripheral arterial disease being reported in up to 50% of cases.17 These differences in the prevalence might be explained by differences in populations’ characteristics and methods of evaluation.20 As shown previously in the results, we divided our sample according to the presence and absence of vascular induced cause for diabetic foot and then we studied the different possible contributing factors for development of diabetic foot among the 2 groups. Patients with vascular induced diabetic foot were significantly older than the non vascular group (mean age of 65.17 years versus 61.29 years; p=0.013). This might be explained by the fact that the older the patient is and the longer the duration of having diabetes is, the more likely they will develop PAD although in our study, diabetes duration was insignificantly correlated in both groups, and this might be due to lack of knowing the duration of diabetes in 56.7% of our patients.21 It was also found that coronary arterial disease and PAD (found in the other non-affected lower limb of the patient) were significantly more prevalent in the vascular group compared to the non vascular. This might be explained by the fact that patients who presented with PAD are more likely to have more generalized and severe athersclerotic disease when compared to the non vascular group.21 Putting the fact of more prevalent of neuropathy in our community is and the fact that diabetic patients with neuropathy might have difficulty in describing pain in the earlier course of PAD and thus as a result may present with ulcerations and gangrene as the first signs of PAD, strike the importance of performing an objective vascular assessment for all the diabetic patients who present with DFU as ischemia has a major impact on the outcomes of DFU and on the limb as a whole.17,19,22 In our study, a total of 140 patients underwent amputation (34.83%) which is a little bit higher when compared to an amputation rate of 29.7% from a previous study that was carried out in Jeddah, KSA.19 However, the amputation rate was similar to a study that was carried out in Australia with amputation rate of 34.1% and in Nigeria with amputation rate of 35.4%.23,24 These similarities in the amputation rates might be explained by the similarities of the patients’ characteristics and the guidelines that were followed by the treating physicians in these different regions; however, differences in amputation rates might be seen with other studies in different populations.25 These differences in the amputation rates can be explained by the differences in patient characteristics, the quality of care, the degree of certainty of a given diagnosis, and the physicians’ agreement on the treatment plan based on the geographical region.25 Furthermore, due to social and cultural beliefs, many patients tend to seek help from traditional healers which results in a delayed presentation and an increased risk of extensive infections. We found that different types of amputation were significantly more frequent among the vascular group compared to the non-vascular group, which is consistent with what is found in the literature.26,27 This is due to the adverse effects of PAD on the rate of ulcer healing; impairing the delivery of oxygen, nutrients, and antibiotics to the infected area therefore, it is to be recognized that early detection of PAD is required to determine the need for vascular interventions as these interventions seem to increase the probability of ulcer healing.17,22,27 The complexity of underlying causes of diabetic foot in general and the subsequent complications especially amputation necessitates a multidisciplinary approach, which includes: nurses, orthopedic surgeons, plastic surgeons, vascular surgeons, and nutritionists.28 In addition, to provide the cardinal features for the treatment of the diabetic foot, which include: wound care, debridement, adequate vascular supply, metabolic control, improvement of nutritional status and appropriate antibiotic.16 Coordination between vascular surgeons, reconstructive plastic surgeons and orthopedic surgeons is important to decide about the need of vascular interventions, the best time for definitive wound closure and providing the appropriate way to prevent recurrence of ulcers after treatment by providing the biomechanical support to the limb.29 This would put an excessive pressure on the health system and economy, due to the large number of diabetic patients in KSA, which means a comprehensive but attainable treatment algorithm is needed to get successful results.30,31
Study limitations
Our study findings are limited by the retrospective study design. Therefore, we did not have complete data for all patients who visited our facility which resulted in the relatively small number of patients in our study. The single-center experience may be a strength in our study. The techniques used in measuring the ABI and TBI were standardized and performed by the same personnel to minimize the interobserver variations.
In conclusion, the present study aimed to determine the prevalence of, and factors associated with diabetic foot of a vascular etiology in patients presenting to a tertiary center in KSA with diabetic foot. In contrast to the western world, minority (19.1%) of the patients were diagnosed to have a vascular induced diabetic foot. Most of the diabetic foot cases were not caused by PAD. Due to the systemic nature of diabetes and the chronicity of the disease, old age, history of coronary artery disease, and PAD in the other unaffected limb were the only factors that were significantly associated with vasculopathic diabetic foot. Other factors like control of diabetes, stroke, and microvascular complications in diabetes were factors that were not significantly associated with diabetic foot of a vascular cause.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 6, 2020.
- Accepted December 14, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.