


Abstract
Objectives: To compare the effectiveness of Maitland versus Mulligan mobilization techniques on pain, functional disability, and psychological status in patients with neck pain.
Methods: Forty-four patients with nonspecific neck pain were randomly assigned to the Maitland group (n=22 patients received Maitland therapy [central or unilateral postero-anterior pressure] for 2 sessions/week for 3 weeks) and Mulligan group (n=22 patients received Mulligan sustained natural apophyseal glides for 2 sessions/week for 3 weeks). This study was conducted at the Rehabilitation Clinic, King Abdulaziz Hospital, Jeddah, Kingdom of Saudi Arabia between December 2016 to May 2017. The outcome measures were the numeric pain rating scale score, neck disability index score, beck depression inventory score, State-trait anxiety inventory score, fear avoidance beliefs questionnaire, and pain catastrophic scale results. The independent t-test, Shapiro-Wilk test, and paired t-test were used in data analysis.
Results: There were significant improvements in mean values of the numeric pain rating scale, neck disability index, beck depression inventory, state-trait anxiety inventory scores, and pain catastrophic scale results after the interventions in both groups (p<0.05, all except fear avoidance beliefs results in mulligan group p>0.05), and there were no significant differences in mean values between the groups (p>0.05).
Conclusion: In patients with nonspecific neck pain, Maitland and Mulligan mobilization techniques have positive effects on neck pain, functional disability, and selected psychological features with no significant difference between them.
Neck pain is one of the most common musculoskeletal painful disorders. Approximately 70% of individuals have neck pain at some time in their lives.1 It is the fourth cause of functional disability after back pain, depression, and arthralgia.2 Neck pain is usually complex and encompasses several factors related to ergonomic, individual, behavioral, and psychosocial aspects.3 The pathology of neck pain may fluctuate between remission and exacerbation.4 The common associated affections and symptoms of neck pain are pain, functional disability, and psychological features, namely anxiety, depression, pain catastrophizing, and fear avoidance, which are considered as predictive of poor outcomes in patients with neck pain.5,6 From the biopsychosocial view, pain and functional disability are considered as a multidimensional, dynamic interaction among physiological, psychological, and social factors that reciprocally affect each other and result in chronic and complex pain.6 The psychosocial factors have a dominant and significant role in shaping the trajectory of chronic pain conditions and pain perception mechanisms.7 It was suggested that high levels of psychological distress and diminished cognition are usually associated with decreased benefits from different kinds of pain alleviating therapeutic interventions.7 The pain transition process from acute to chronic persistent pain, depression, inactivity, and disability was explained by the fear avoidance model. Avoidance is the behavioral response to fear about pain that influences treatment outcomes.7 Exercise and manual therapy (MT) are the most widely and effectively used physical therapy treatments for neck pain.4,6,9,10 Manual therapy is usually used to reduce pain, improve cervical kinesthesia, and improve joint mobility.11 Manual therapy activates the sympathetic nervous system and has extended analgesic effects beyond the specific body segment receiving the treatment.12 Maitland and Mulligan mobilization techniques are commonly used types of MT in clinical practice.11 A better outcome is expected after a mobilization intervention under high anxiety levels, whereas a better prognosis is expected after manipulation and sustained natural apophyseal glides (SNAGs) under low anxiety levels.11
It was proven that somatization, depression, and fear are associated with perceived recovery, pain, and function among patients with neck and back pain.13 There is a strong association between low fear avoidance beliefs and low pain self-efficacy with positive changes in pain and functional disability.14 A patient’s high expectation of the treatment outcome had a positive impact on treatment success.15 Limited studies have investigated the relationship between psychological factors and treatment outcomes for subacute and chronic neck pain.6,13-16 Few studies found a positive effect of exercises on psychological factors among patients with neck pain.17 However, the effects of MT on pain, functional disability, and psychological aspects still needed to be investigated.6
Therefore, the objective of this study was to compare the effectiveness of Maitland with Mulligan mobilization techniques on neck pain, functional disability, and psychological variables (depression, anxiety, pain catastrophizing, and fear avoidance) in patients with subacute and chronic nonspecific neck pain.
Methods
All procedures were approved by the Ethics Research Committee of the Institutional Review Board of Imam Abdualrahman Bin Faisal University, Saudi Arabia (IRB-2016-03-143). The study was conducted in accordance with the Declaration of Helsinki at the Rehabilitation Clinic, King Abdulaziz Hospital, Jeddah, Kingdom of Saudi Arabia between December 2016 to May 2017. All participants were informed that the collected data would be submitted for publication, and a consent form was signed before study participation (Clinical Trials Registration: ClinicalTrials.gov with ID: NCT03089021).
Forty-four male and female patients with subacute and chronic nonspecific neck pain were recruited from the Rehabilitative Clinic, King Abdulaziz Hospital and East Jeddah General Hospital in Jeddah, Saudi Arabia.
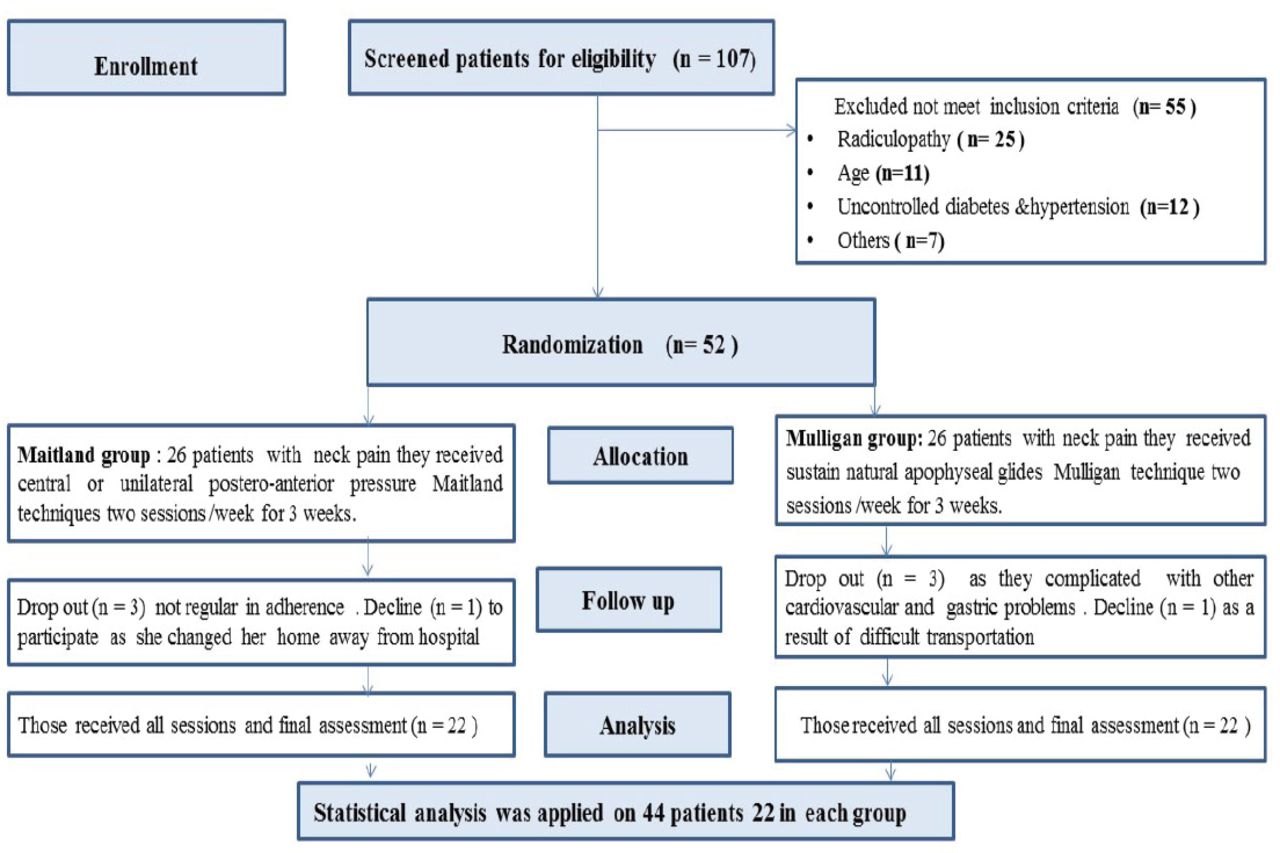
Randomization was carried out using GraphPad software before patients’ recruitment. The treating and assistant therapists (assessors) who collected the outcome measures were blinded to the treatment groups (GraphPad Software, Inc., San Diego, CA). Twenty-two patients were allocated to the Maitland group, and the other 22 patients were allocated to the Mulligan group (Figure 1).
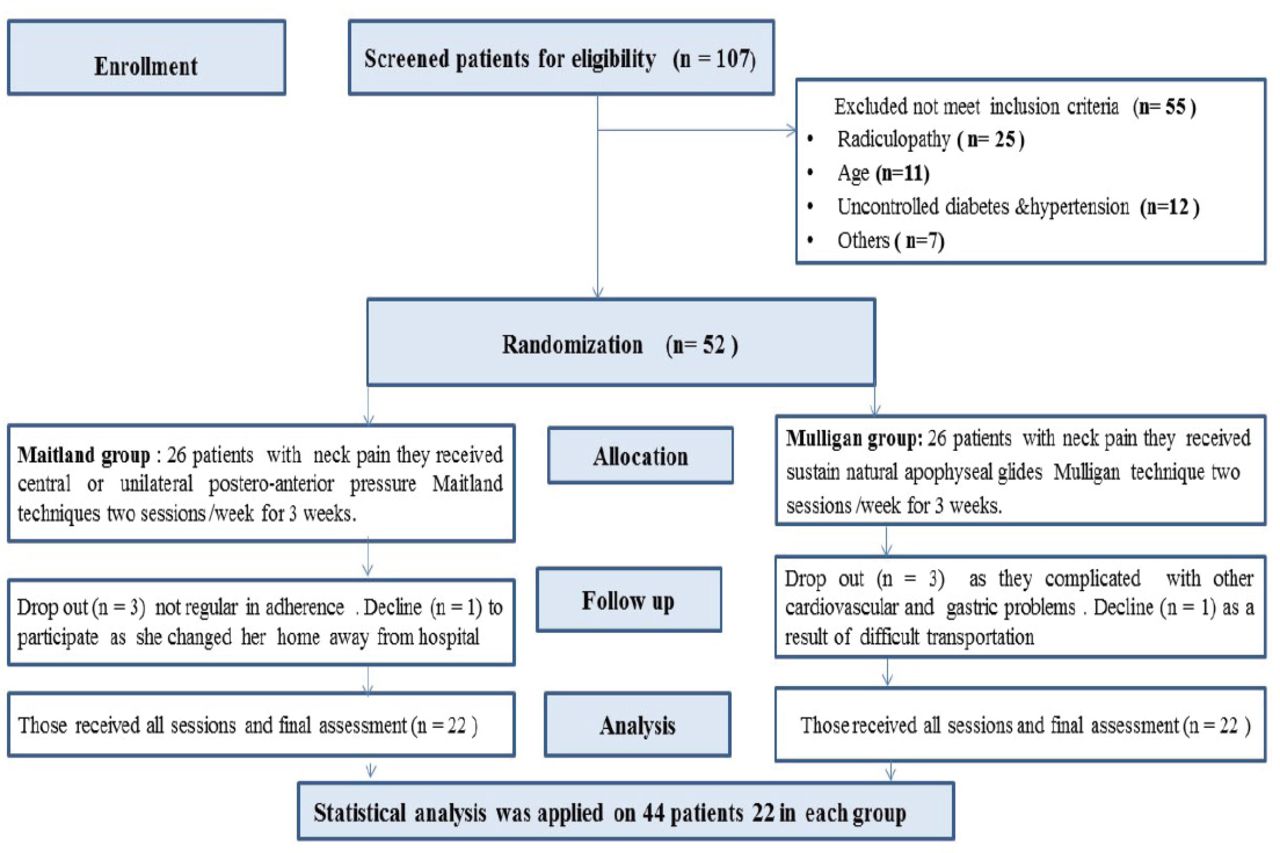
Flow chart of patients with subacute and chronic nonspecific neck pain.
The sample size was calculated using an online tool that uses the pain mean (µ1 = 1.48, µ2 = 1.70) and standard deviation (0.25) reported in a previous study.6 The significant value was 0.05 with a power of 0.80.
Patients with neck pain for more than one week without radicular symptoms that extended to the posterior aspect of the neck from the superior nuchal line to the first thoracic vertebra were included in this study.10
Patients who were contraindicated to mobilization, namely pregnant women and patients who had whiplash injury, tumor, fracture, metabolic diseases, rheumatoid arthritis, osteoporosis, and hypertension (with resting blood pressure >140/90 mm Hg), cervical radiculopathy, fibromyalgia pain syndrome, previous neck surgery, neck pain associated with vertigo caused by vertebrobasilar artery insufficiency or chronic headache, psychiatric disorders; and those who received physical therapy treatment in the previous 3 months were excluded.1,10
Assessment procedure
Each patient was evaluated by an assessor using the following criteria. A standardized musculoskeletal examination of the cervical spine was performed to determine the target vertebral level and painful segments that matched each patient’s problem in order to identify the proper site of intervention.
Pain intensity
This was measured by the numeric pain rating scale (NPRS). Each patient was asked to mark a point on the line from 0 to 10 in relation to his/her level of pain.18
Neck disability
This was evaluated by the neck disability index (NDI), a valid and reliable self-report questionnaire consisting of 10 sections.19 Four sections relate to subjective symptoms, and the remaining 6 sections relate to activities of daily living. Each section is scored from 0 to 5 points, giving a maximum score of 50. The total score of the NDI ranges from 0 to 50 points. A higher score indicates a higher disability level.20
The presence and severity of anxiety
This was evaluated by the state-trait anxiety inventory (STAI-Y), a self-report questionnaire that includes 2 scales. The first scale is the state anxiety scale (Y1 form) that requires the patient to answer questions about his/her feelings on that day. It contains 20 items scored from 1 (not at all) to 4 (very much). The second scale is the trait anxiety scale (Y2 form) that requires the patient to answer questions that express his/her propensity for anxiety. It contains 20 items scored from 1 (almost never) to 4 (almost always). The total score for each form ranges from 20 to 80. Higher scores indicate a higher anxiety level.21,22
Depression
This was measured by the Beck Depression Inventory (BDI), which is a self-report questionnaire containing 21 items. Each item has 4 self-evaluation statements that must be answered in consideration of the last 2 weeks. It is scored from 0 to 3, and the total score ranges from 0 to 63. Scores are grouped as follows: 0 to 10 (normal), 11 to 16 (mild mood disturbance), 17 to 20 (borderline clinical depression), 21 to 30 (moderate depression), 31 to 40 (severe depression), and over 40 (extreme depression).23
Fear avoidance
This was evaluated by the fear avoidance beliefs questionnaire (FABQ), which is a self-report questionnaire that contains 16 items. The first 5 questions relate to fear avoidance of physical activities (FABQ-PA). The remaining 11 questions relate to fear avoidance of work (FABQ-W). The score for each question ranges from 0 (strong disagreement) to 6 (strong agreement). The total score for FABQ-PA ranges from 0 to 30 and that for FABQ-W ranges from 0 to 66. Higher scores represent higher levels of fear avoidance.15
Pain catastrophizing
This was evaluated with the pain catastrophizing scale (PCS). It consists of 13 items and assesses 3 aspects of catastrophizing: rumination (4 questions, numbers 8-11), helplessness (6 questions, numbers 1-5 and 12), and magnification (3 questions, numbers 6, 7, and 13). Each question is scored from 0 (not at all) to 4 (all the times). The total score can be obtained by score summation of the 13 items, and it ranges from 0 to 52 with high scores indicating high pain catastrophizing.18,24
Treatment procedure
Six treatment sessions were applied to each patient, 2 sessions/week for 3 weeks. All patients were treated by a therapist. The hypomobile and painful spinous process or facet joint that matched the patients’ chief complaint was treated with MT according to the patient group.
Maitland group
Each patient laid in the prone position with his/her forehead comfortably resting on her/his hands. The therapist stood at the side of the patient’s head and placed the 2 tips of her thumb pad on the posterior surface of the articular process that should be mobilized. Passive spinal segmental mobilization in the form of low velocity, small, or large amplitude oscillatory movements was applied to the target cervical vertebrae in each patient.25 The applied technique was central posterior-anterior oscillatory pressure on the spinous process of the target segment (Figure 2A) or unilateral posterior-anterior oscillatory pressure on the facet joint of the target segment.25 Oscillatory pressure was applied for 2 minutes and repeated 3 times with 1 minute of rest in between each mobilization. The grade of mobilization and pressure site were chosen in accordance with the examination findings and patient’s response to mobilization.6,10
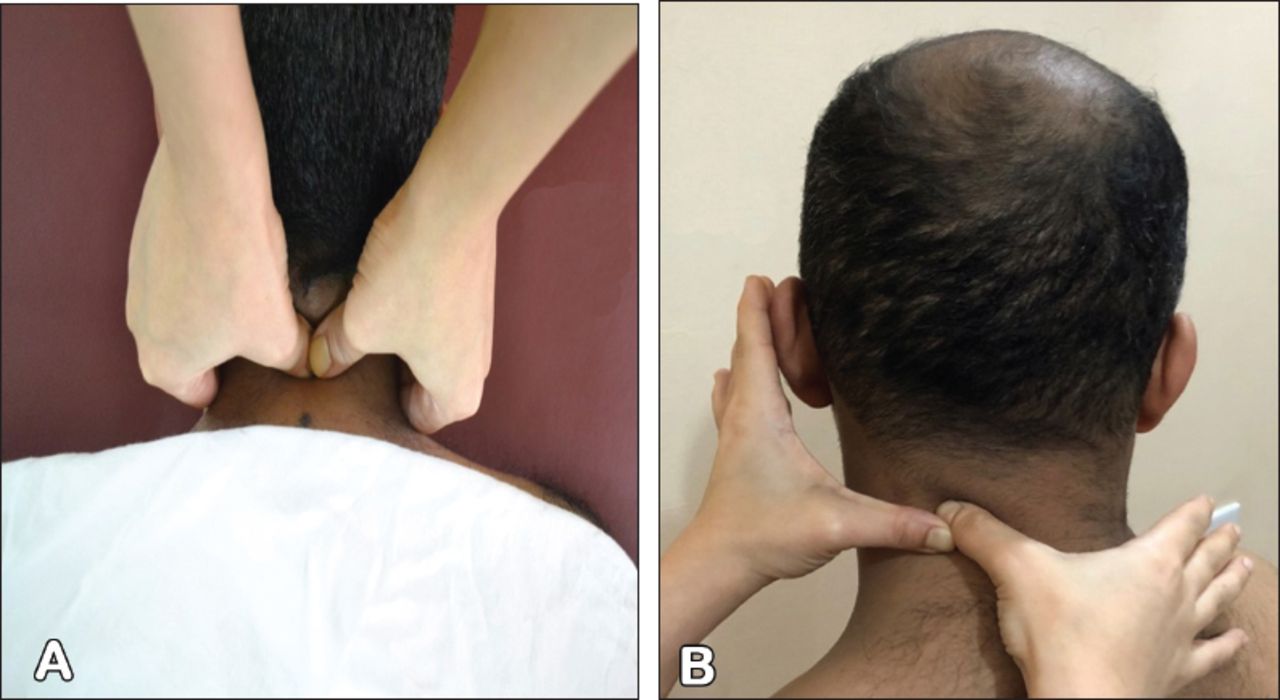
A) Maitland technique of central posterior-anterior oscillatory pressure on spinous process of cervical 3. B) Mulligan technique of sustained natural apophyseal glides (SNAGs) mobilization technique with right rotation on the left cervical 3/4.
Mulligan group
Each patient sat in a comfortable sitting position on a chair, and the therapist stood behind her/him to perform the SNAGs technique. The medial border of the distal phalanx of the therapist’s thumb was placed on the patient’s spinous process or on the facet joint of the superior vertebra of the target segment for treatment. A gliding force was applied toward the patient’s eye by the therapist’s other thumb, while the therapist’s other fingers rested on the lateral side of the patient’s neck (Figure 2B). The therapist maintained this gliding force. Each patient moved his/her head slowly toward the painful and restricted side (flexion, extension, rotation, and lateral flexion), and more pressure was applied by the patient at the end of active movement. The therapist’s hands followed the patient’s head movement to ensure mobilization with movement. The Mulligan mobilization was repeated 10 times for 3 sets.26
Statistical analysis
The collected data were analyzed using SPSS, version 20 (IBM Corp., Armonk, NY, USA). The independent t-test was used to compare baseline demographic data between the groups. The Shapiro-Wilk test was applied to all variables to test the normality distribution of the data. Parametric analysis was conducted to analyze normally distributed variables. The paired t-test was used to compare the effects before and after the interventions within each group, and the independent t-test was used to compare the effects of interventions between the groups. Statistical significance was set at a p-value <0.05 with a confidence interval at 95%.
Results
Statistical analysis was applied to 44 patients (41 women and 3 men; age range, 25-45 years). Among those, 10 patients had subacute neck pain, and 34 had chronic nonspecific neck pain.
There were no statistically significant differences in mean values of age and body mass index between the Maitland and Mulligan groups (p=0.875 and p=0.497). The percentage of used medications decreased after the interventions, from 9.1% to 2.3% in the Maitland and from 20.5% to 0% in the Mulligan groups. Detailed demographic data are presented in (Table 1).
Demographic data of patients in the Maitland and Mulligan groups.
The percentages of patients adherence and number of sessions of the treatment interventions were 97.31% (129 sessions) in the Maitland and 98.48% (130 sessions) in the Mulligan groups, and there was no significant difference between the groups (p=0.644), (Table 1).
Comparison of neck pain, functional disability, and depression within and between the groups. The mean values of the pain rating and catastrophizing scales, NDI, and BDI reduced significantly after the interventions in the both Maitland and Mulligan groups (Table 2) with no significant differences between the groups (Table 4).
The mean values of neck pain, functional disability, and depression pre and post the Maitland and Mulligan interventions.
Comparison of the selected psychological variables within and between the groups. The STAI-Y reduced significantly after the interventions in both groups while FABQ-PA, and FABQ-W reduced only in Maitland group (Table 3) with no significant differences between the groups (Table 4).
The mean values of anxiety and fear avoidance pre and post the Maitland and Mulligan interventions.
Comparison of the measured variables post the Maitland and Mulligan interventions.
Discussion
Previous studies confirmed that psychosocial status has a dominant and tangible role in the development of pain and adjustment during the long-term process that is accompanied by pain.7,13,15 The current study results revealed significant reductions in neck pain and functional disability after the application of either Maitland or Mulligan mobilization techniques. These findings are in agreement with those of previous studies of patients with nonspecific and chronic neck pain.1,9,27,28
Ali et al27 found that the addition of Maitland mobilization to both isometric neck exercises and shortwave diathermy effectively improved neck pain and functional disability compared with cervical traction. Tachii et al1 proved that the short-term application of SNAGs in addition to a hot pack and neck isometric exercises also improved neck pain and functional disability. When comparing Maitland and Mulligan mobilization techniques, there were significant reductions in neck pain and functional disability after 30 days of the interventions.9 Several authors confirmed that MT has analgesic effects on pain.1,6,10-16 The underlying mechanisms of pain reductions after MT may be due to the influence of analgesic mediations and sympatho-excitatory effects through the activation of large-diameter, low-threshold mechanoreceptors, which in turn results in inhibition at the spinal cord level, according to the gate control theory of pain. Activation of the dorsal periaqueductal grey matter is used to control the motivational states through the release of serotonin and nor-adrenaline from the descending neurons.12 At the same time, reductions in neck pain have positive impacts on functional activity and reductions of the neck functional disability index.20
In contrast with the current study’s findings, some authors found that SNAGs of MT did not induce any benefit in neck pain and the functional disability index.28 Those authors followed a multi-modal management strategy, and found that SNAGs of MT in addition to isometric training induced more improvement in pain and physical activity than using only SNAGs for 6 weeks in patients with nonspecific neck pain. The current study used only SNAGs for 2 sessions/week for 3 weeks without any additional treatment. Urrehman et al28 used SNAGs in a comparative group for 6 weeks for 4 times/week, which was longer than the duration of SNAGs was applied in the current study.
There is controversy in the literature regarding which technique of manual mobilization is better for relieving neck pain and reducing functional disability.10,29,30 There were no significant differences in mean values of pain and functional disability between both mobilization techniques. A previous study found similar effects with non-long-term differences in pain and functional disability among 3 manual techniques in patients with chronic neck pain.10 In contrast with the current results, one study found that the application of Maitland thoracic mobilization and endurance training has no extra benefits compared to endurance exercises in reducing the neck disability index.31 A possible explanation for this difference is that the authors used mobilization for the thoracic spine not the cervical region as in the current study. In contrast, Lopez et al6 concluded that high velocity, low amplitude postero-anterior mobilization reduces pain during rest more than SNAGs in patients with neck pain. One session was applied in their study,6 whereas 2 sessions/week were applied for 3 weeks in our study. Some recent studies support the superiorty of Mulligan (SNAGs) mobilization over other techniques for neck pain relief.9,29,30 Gautam et al9 demonstrated that Mulligan mobilization is more effective for improving neck pain and functional disability than Maitland mobilization. The authors applied Mulligan mobilization in addition to active and isometric exercises whereas in the current study, manual techniques were applied without any additional exercises. In addition, Hussain et al29 proved that the Mulligan technique was more effective than the Maitland technique in pain improvement and disability in patients with nonspecific neck pain. Their results may be different from ours because they applied Mulligan natural apophyseal glides, whereas the current study applied Mulligan SNAGs. In the current study, the Maitland technique was used on the basis of patients’ examination findings and their response to mobilization. Thus, all grades of mobilization (I, II, III, and IV) were included in the current study, but only grades I and II were included in Hussain et al’s study.29 Hussain et al29also used both ultrasonic and short-wave diathermy with MT, whereas the current study used only MT. Furthermore Tanveer et al30 reported that SNAGs mobilization was more effective in pain reduction than Maitland mobilization for nonspecific neck pain. The authors applied SNAGs and Maitland mobilization for 3 sessions/week for 3 weeks, whereas in the current study, mobilization techniques were applied only for 2 times/week for 3 weeks. In addition, our study had older participants (age range, 25 - 45 years) than Tanveer et al,’s study (age range, 20-39 years).30
According to the current study results, there was a significant improvement in the selected psychological variables (trait anxiety, depressive symptoms, and pain catastrophizing) after the interventions in both groups. Results of the FABQ-PA and FABQ-W significant improved after only Maitland mobilization. Many studies are in agreement with the selected psychological variables as important predictors of a successful outcome after physical therapy intervention in patients with neck pain.13,15 Furthermore, the interaction between psychological variables and physical therapy treatment outcomes is proven in the literature.6,14,17,32 Many authors supported that active therapy in the form of different types of exercises has positive effects on the psychological status of patients with neck pain.14,17 Edwards et al8 reported that high levels of distress, catastrophizing, and low levels of self-efficacy for managing pain may produce attentional and information-processing biases that lead individuals to respond selectively and intensely to pain-related stimuli (namely, they ruminate more about their pain sensations). There is a strong association between pain, functional disability, and fear avoidance as a recognized example of the psychological status of patients with neck pain.13 In other words, when pain and functional disability decrease, the psychological stresses will decrease and vice versa.17
Unfortunately, few studies have examined the direct effect of MT on psychological factors. Only one study previously compared manipulation, posteroanterior mobilization, and SNAGs during one session in patients with neck pain.6 The authors found that among the psychological factors, only patients with trait anxiety responded to the applied manual techniques. High-anxiety patients responded to the mobilization and SNAGs, but the others with low anxiety responded to the manipulation effects. In the current study, MT was applied for 6 sessions, which is considered long and repeated applications of MT in comparison to only 1 session in the previous study.6
Study limitations
A small number of male subjects participated in the study, no control group was included, and the long-term effects of MT were not evaluated.
In conclusion, patients with nonspecific neck pain, the Maitland and Mulligan mobilization techniques have positive effects on neck pain, functional disability, and selected psychological variables with no significant differences between them.
Further studies are required to assess short-term and long-term effects of different physical interventions on psychological variables in patients with neck pain.
Acknowledgment
I gratefully acknowledge the patients who participated in this research study; research assistants, Mahmoud Elsayed Shanab and Belal Elsayed Shanb; and staff of the Department of Physical Therapy, College of Applied Medical Sciences, Imam Abdulrahman Bin Faisal University.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 6, 2020.
- Accepted November 23, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.