


Abstract
Objectives: To demonstrate the efficacy of cochlear implants (CI) in post-lingual adults, including surgical and auditory outcomes based on a 25-year experience at a tertiary referral hospital.
Methods: This study was a retrospective, descriptive chart review of post-lingual adults, aged ≥18 years, implanted at King Abdullah Ear Specialist Center (KAESC), Kingdom of Saudi Arabia (KSA), between September 1994 and March 2020. The study included 176 cochlear implantations performed in 144 patients. Data retrieval included patient demographics, clinical evaluation, operative details, postoperative course, and audiological evaluation parameters. The main outcome measures were surgical procedures, including techniques and complication rates, and audiological parameters as evaluated by pure tone audiometry average (PTA), speech reception threshold (SRT), and word recognition score (WRS). Student’s t-test and Chi-square tests were used for statistical analysis and a p-value<0.05 was considered significant.
Results: Pure tone audiometry average, SRT, and WRS improved significantly after CI. Overall, major complications occurred in 3 patients. One patient underwent CI ex-planation for severe pain, and 2 had device malfunctioning. Other minor complaints were reported in 18% of the patients.
Conclusion: Cochlear implants performed, in our institute, on post-lingual adults resulted in significant improvements in auditory performance, including PTA, SRT, and WRS values with low complication rates.
Hearing loss is one of the common disabilities in adults. Unlike routine ophthalmologic examinations, screening for hearing loss among adults may not be performed regularly during primary care visits. This has resulted in lower rates of referrals for the in-depth testing of these patients. The other problem of hearing loss in post-lingual adults is poor follow-up rates and poor adherence to recommended treatment after screening. This means that the burden of hearing disabilities among adults is higher than reported.
Cochlear implants (CI) are one of the most effective measures for treating severe to profound hearing loss. The Food and Drug Administration (FDA)recommended the use of CI in adults as early as 1970s.1
A limited number of studies have examined CI in post-lingual adults with a large number of participants. Further, as the literature review also showed a lack of related reported practice in Arabic countries.
Methods
This is a retrospective chart review of all post-lingual adults who underwent implantation between September 1994 and March 2020 at King Abdullah Ear Specialist Center (KAESC), a tertiary referral center in Kingdom of Saudi Arabia (KSA). Patient lists were retrieved from the CI registry. A comprehensive chart review was prepared from the patients’ medical records to compile the data. The study was approved by the Institutional Review Board of the University Hospital (Reference Number 20/0589).
Participants aged >18 years at the time of the first implantation who had developed verbal speech according to the speech therapists were included in the study. All those participants were included who had received unilateral, bilateral simultaneous, or bilateral sequential CI or explanted after CI at our institute. Participants of both gender and all nationality were included. Patients were excluded if they refused or failed to undergo CI. Those who underwent CI at another center and were followed up at our institute were excluded because of the lack of detailed patient related records.
Both the electronic and paper-based medical records of the participants were comprehensively reviewed for data retrieval. The extracted data included patient demographics, duration of hearing loss, clinical evaluation, audiological assessment and radiological findings, operative details, and postoperative course and complications.
Evaluation of CI performance was carried out using audiological evaluation, including pure tone audiometry average (PTA), speech reception threshold (SRT), and word recognition score (WRS). These tests were performed in soundproofed booths by audiologists. Pure tone average were measured manually using the American Speech-Language-Hearing Association (ASHA) guidelines.2 Speech audiometry (SRT and WRS) was performed using the Arabic language set in accordance with the ASHA guidelines.3,4
Statistical analysis
Microsoft Excel (version 16.3; Microsoft, Seattle, WA, USA) was used for data management. The Excel file was saved on an encrypted Google Drive. Data was analyzed using the Statistical Package for Social Sciences, version 23.0 (IBM Corp., Armonk, NY, USA). Student’s t-test and Chi-square were used, and the significance level was set at 0.05, with confidence interval of 95%. The means of the raw data were used for further analysis, as appropriate.
Results
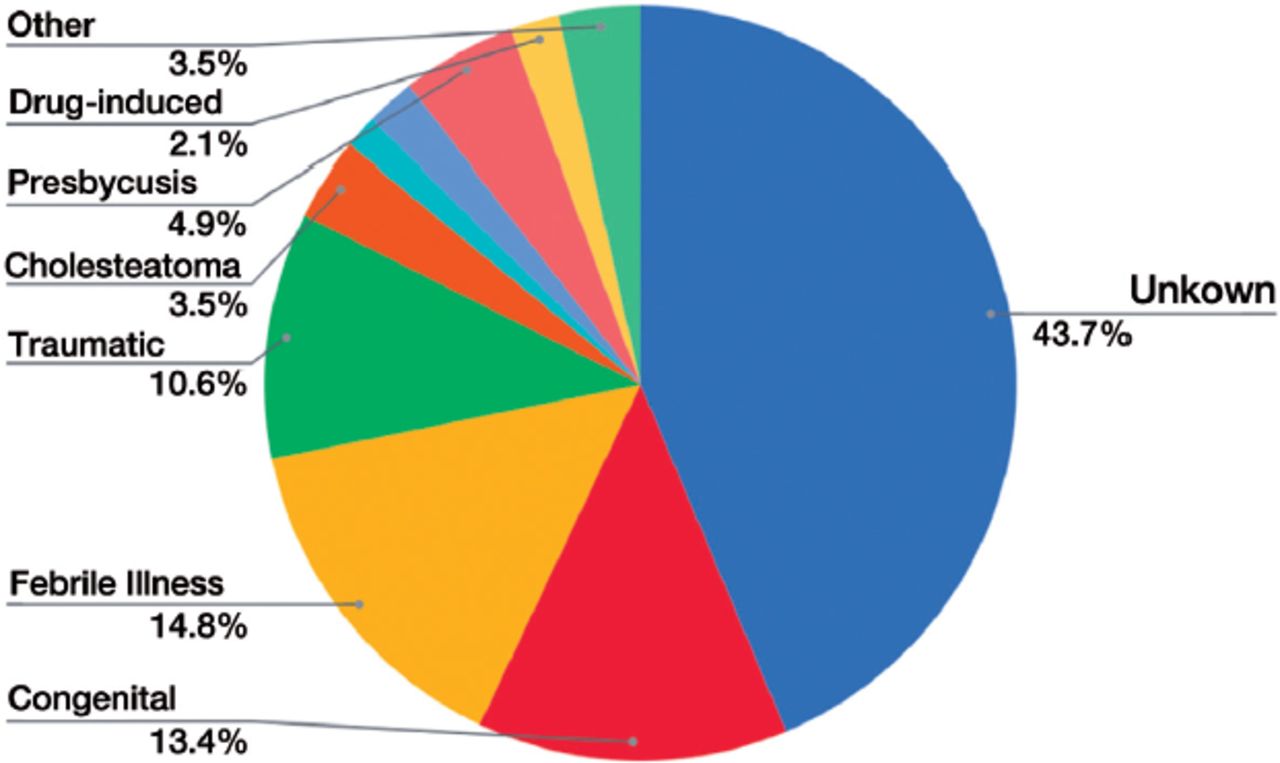
This study included 176 CIs performed in 144 patients. The male:female ratio was 1.61:1. The mean age at the time of CI was 35±15 years. The side of implantation was the left side in 80 (45%) patients and right side in 96 (54%) patients. The common causes of hearing loss were febrile illness in 21 (14.8%), congenital progressive in 19 (13%), and traumatic in 15 (10%) of patients. However, in a large percentage of patients (n=62, 43%), the cause of hearing loss was not known after evaluation. Other rare causes of hearing loss were stroke, Vogt-Koyanagi-Harada disease, Usher syndrome, mitochondrial gastrointestinal encephalopathy syndrome, Meniere’s disease, and tubotympanic chronic suppurative otitis media (Figure 1).
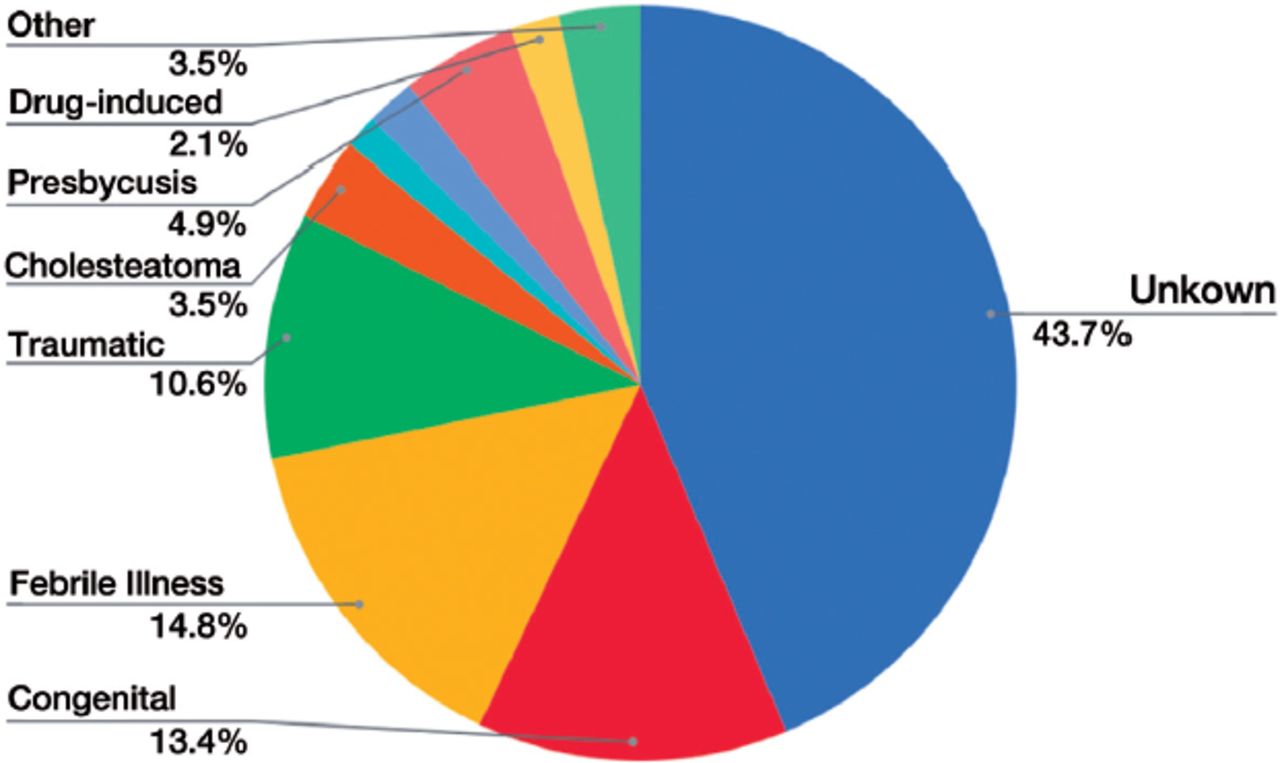
- Showing the etiologies of hearing loss in the study population.
The ototoxic agents that caused hearing loss in 3 (2.1%) of the participants were antibiotics in 2 and isotretinoin in one patient. One of the 2 patients with noise-induced hearing loss had a military occupation, and the other worked in a machinery factory. Nine percent of the patients had associated otological conditions.
The average age of hearing deprivation before CI was 15±11 years (1-56 years). More than half of the patients (n=105, 59%) used hearing aids before the CI, for a mean duration of 10.5±9.5 years (1-30 years). One-fifth (n=30, 17%) used hearing aids in the other ear after CI.
Fourteen (8%) patients had a history of otologic surgery. Four patients had contralateral CI, 2 had canal wall down, 4 had undergone tympano-ossiculoplasty, and one patient underwent congenital cerebrospinal fluid leak repair. Most of the participants had normal otomicroscopy (n=74/79, 94%). Three patients had tympanic membrane perforation, one had a dull tympanic membrane, and one had a retracted tympanic membrane. Most patients (n=93/105, 89%) had a type A tympanic membrane. Type B was found in 9% (9/105) and type C in 3% (3/105) of the patients.
Cochlear implants was performed under general anesthesia in 84% (109/129) and local anesthesia in 15% (20/129) of the participants. General anesthesia was routinely administered. Local anesthesia was chosen when the patient did not have any medical illness that rendered general anesthesia risk. A post-auricular incision was used in most patients (95%, 115/121). The periosteal flap used was a Palva flap in 57% (55/97) and a superiorly based flap in 30% (29/97) of the patients. Insertion occurred through the round window in 78.5% (95/121) of the cases, and through cochleostomy in the remaining 21.5% (26/121) cases. A smooth insertion was reported in 90% (50/55) of implants. A difficult insertion, defined as minimal resistance to implantation that did not reach the level of preventing further advancement, occurred in the remaining 5 cases. A complete insertion was achieved in 98% (92/94) of the patients, whereas partial insertion was observed in 2% (2/94).
Lateral wall was used in 53% (50/94) and peri-modiolar electrodes was used in 46% (44/94) patients. One patient was implanted bilaterally with double-array electrodes, which was chosen to increase cochlear coverage because the patient had cochlear ossification. Only one patient was a candidate for electroacoustic stimulation. Med-el, Advanced Bionic and Cochlear companies’ CI were used in 48% (n=86), 36% (n=64), and 14% (n=26) of the patients, respectively.
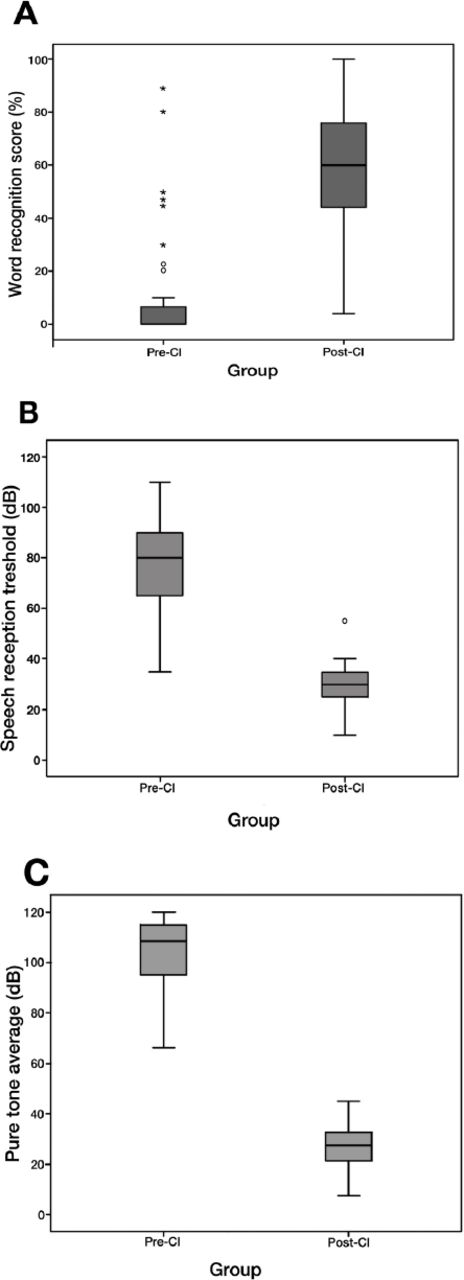
The preoperative pure tone was 102±15 dB, which improved significantly after CI to 29±10 dB (p<0.001 with a mean difference of 76.52 and 95% confidence interval: 72.14-80.98). The SRT also improved from 76±21 dB to 29±12 dB (p<0.001, with a mean difference of 48.79% and 95% confidence interval: [40.26-57.32]). The WRS increased significantly from 6.94±16.71 to 61.43±23.13 (p<0.001; mean difference 54.48; 95% confidence interval: 47.41-61.56) (Figure 2).

- Box-plot graph showing the significantly A) lower pure tone average in post-cochlear implant (CI) group, B) lower speech reception threshold in post-CI group, and C) higher word recognition score (WRS) in post-cochlear implant group.
Preoperatively, most patients (62%, 54/87) relied on lip reading for communication. Verbal communication occurred in 36% (32/87) of patients who had either hearing aids or underwent CI in the other ear or had normal hearing. One patient relied on writing for communication. Postoperatively, only 10 patients continued relying on lip reading, whereas the majority communicated verbally (86%, 63/73). There was a significant improvement in the number of patients who developed verbal communication (Chi-square: 39.56; p<0.001).
Overall, intraoperative complications occurred in 6% (11/176) of surgeries. Accidental exposure of the dura occurred in 3 patients, accidental exposure of the facial nerve in one, bleeding in 3, gusher in 2, injury to the external auditory canal in one, and intraoperative pain with local anesthesia that required conversion to general anesthesia in one patient.
Major postoperative complications occurred in 3 patients (1.7%). One of these patients underwent CI with Hifocus Mid-Scala type of electrode, who was ex-plantated due to severe pain at the site of the implant with no identifiable reason. Two other patients had an ex-plantation due to device malfunctioning. One of them was implanted with HiFocus Mid-Scalar type of electrode and the other was implanted with Nucleus CI12 contour advance type of electrode. Minor complications were reported in 18% (38/176) of cases, including self-limiting vertigo in 6% (11/176), redness and pain at the implant in 5% (8/176), facial twitching in 4% (7/176), dizziness and tinnitus in 2% (3/176), and taste disturbance in 1% (2/176) of patients (Table 1).
- Summarizing intraoperative and postoperative complications of cochlear implantation (CI) (N=176).
Cochlear implants in adults are seen in our center by audiologists and speech language pathologists, one month after device activation. Then they have monthly follow-up sessions until they reach a stable satisfactory level.
The adherence to CI was as follows: 88% (84/96) were satisfied using the implant, 2% (2/96) were using, but were not satisfied, and 10% (10/96) were not using it. The reasons for not using the implants were reported to be unsatisfactory hearing intelligibility, unpleasant sounds, and tinnitus.
Discussion
The data in this study demonstrate the outcomes of post-lingual adult CI at a single tertiary referral center. This study showed significant improvements in the PTA, SRT, and WRS values, which resulted better communication from lip-reading to verbal communication. Many studies have observed better speech recognition outcomes in post-lingual individuals and those communicating verbally during childhood.5,6 This may be due to the loss of auditory stimulation in manual communicators during early development, when auditory cortex maturation generally occurs, which is irreversible even after late CI.7
The etiology of hearing loss in a large proportion of the participants was unknown, which is consistent with a previous report.8 One of the most frequently reported etiologies among our participants was febrile illness.The feasibility of performing CIs under local anesthesia as a day surgery case has been previously studied in our institute. It was found to be safe and to decrease postoperative discomfort and complications associated with general anesthesia. Patients who underwent surgery under local anesthesia required a lower recovery time.9
This study reported a 6% rate of intraoperative complications and 20% rate of postoperative complications. The majority of postoperative complications (80%) were minor, this was comparable to those reported in previous studies.10,11 A frequent postoperative complication in the present study was self-limiting minor vertigo (11%).
Meningitis is a potentially serious post-CI complication. Notably, meningitis did not occur in any of the study populations. This could be attributed to adherence to the Centers for Disease Control (CDC) recommendations for vaccination, sterile surgical techniques, and postoperative wound care. The CDC recommendations include vaccination prophylaxis against Streptococcus Pneumoniae, which is the most common cause of meningitis in cochlear implanted patients.12 Moreover, the study population comprised all adults, whereas the incidence of meningitis is highest among children younger than 6 years, with a higher ratio of congenital cochlear anomalies.10
In this study, the number of years of hearing deprivation reached 56 years, with a mean of 15±11 years. The reason for the long gap between the onset of hearing loss and CI needs to be investigated. Nevertheless, it is speculated that the delay could be because of a defect in the referral process or a lack of knowledge and motivation in patients, or their fears and concerns regarding CI. Further investigations are warranted to determine the exact reasons for this finding. The role of a long duration of hearing deprivation is not well established. Although the effectiveness of early CI can be the same as that after long hearing deprivation, it is rational to increase the duration of life spent by the patient with the privilege of better hearing with CI.13
The chart review and auditory outcomes of this study can contribute to the preoperative counseling of CI candidates and help to draw their expectations and address their concerns.
Study limitations
The present study was limited by its retrospective design. However, it consisted of a consecutive, nonselective, and relatively large sample that provided an overview of all aspects of our institution’s experience in managing CI patients.
In conclusion, CI in our institute was found to be a safe and effective management strategy for severe to profound hearing loss in post-lingual adults. Our implanted patients showed significant improvements in auditory performance. The rate of complications in adults was low. The study population was noted to experience a delay in management, which can either be related to the patient or healthcare system and needs further investigation.
Acknowledgment
The authors thank Dr. Lama Alfawzan and Dr. Ammar Altuaibi for their contribution in data collection.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 6, 2021.
- Accepted August 11, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.