


Abstract
This review summarizes the beginning of radiotherapy, techniques of modern radiation therapy with different types, toxicities induced by radiotherapy and their management. Head and neck radiation therapy is still improving for the better management and control of the cancer and induced radiotherapy toxicities.
Head and neck cancer (HNC) represents one of the top common type with incidence of greater than half a million cases diagnosed annually. Oral, pharyngeal, and laryngeal squamous cell carcinoma (SCC) represent almost 90% of the cases. Surgical resection, radiotherapy or both have been used over the past few decades.1,2 The surveillance, epidemiology and end results data in the United States stated that radiotherapy is generally included in primary oncologic treatments.3 Radiotherapy improves clinical, form, and functional outcomes for cancer patients. Currently, almost 75% of patients with head and neck (SCC) will benefit from radiotherapy, whether primary or adjunct therapy after surgical resection. In the early stages of cancer, radiotherapy can replace the need for surgical resection.4-6 Cancer patient can be treated concomitantly with chemoradiotherapy for local advanced cancer or by surgical resection followed by adjuvant radiotherapy. Radiotherapy also used in procedure aims at organ preservation, including avoiding laryngectomy through the use of chemoradiotherapy.7-9 The aim of this review was to summarizes development of the radiation therapy for head and neck cancer with different types of induced toxicity and their managements.
Brief description of radiotherapy history
The utilization of ionized radiation in cancer treatment started in the late 19th century. The field of radiology and radiation oncology was born when the x-ray was discovered by Roentgen on November 30, 1895.10,11 After that, in 1896, Grubbe was the first person that therapeutically applied x-rays, was the first person that experienced x-ray dermatitis, was the first to utilize a sheet as a protecting material and was the first person that claimed that radiation could cure cancer patients.10,11 In the same year, Glver Lyon suggested that the radiation might have bactericidal properties. However, in 1902, after several experiments in the field, it was concluded that the radiation had no bactericidal effects, but it was used to assist the resolution of inflammation for bacterial and non-bacterial infections before the introduction of antibiotics, steroids and chemotherapeutic agents.11
Marie and Pierre Curies also discovered radium in that century, in 1898. In 1920s, Claudius Regaurd applied the concept of fractionated external beam radiotherapy through multiple weeks and was able to treat multiple cases of HNC. Then, his concept of fractionation was popular internationally.11,12
Early radiotherapy was very limited to penetrate deep biological tissues due it its low energy (100 keV). Scientists’ efforts were concentrated to increase x-ray energy to reduce dose deposition on the skin and to reach the internal cancer without skin burns. In 1913, William Coolidge produced x-rays with higher energy (200 keV), which was called orthovoltage external beam radiotherapy but was still considered low beam energy. Then, several groups after that worked to produce supervoltage x-ray beams.13,14
Compact linear accelerators were built on gantries that could rotate around the patient in the 1960s. Additionally, at that time, teletherapy units were introduced, which use cobalt-60 to produce supervoltage x-ray beams.10
Therefore, the conventional type of treatment relied on the 2-dimensional orthogonal skeletal view produced by a fluoroscopic simulator. Two or three radiation beams at different directions at the target results in large volume radiation of the tissue.15
Modern radiation technology
Currently, physical examination and multimodality imaging relay on 3-dimensional anatomic details such as computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography-computed tomography (PET CT) are important to evaluate the treatment volume and outline of tumor and normal tissues. Multimodality imaging can be combined for more details. For example, CT can combine MRI for better soft tissue details and PET-CT to add functional and metabolic details.15,16
The high dose volume will include the primary site of the cancer with the lymph node regions, which are considered the areas of gross disease or gross tumor volume (GTV). Gross tumor volume extends to involve the spread of the cancer to involve the microscopic cancer involvement, which is the clinical tumor volume (CTV1), which is enlarged by 2.5 to 10 mm to the planning target volume (PTV1) depending on the microscopic evaluation of the surgical specimens, which is the typical treatment dose that is usually 66 to 74 Gy (Gray) in 2 Gy fractions or 81.6 Gy in 1.2 Gy fractions.17
Therefore, multiple radiation beams will be directed towards the tumor from different angles and planes. Each beam is designed to follow the outline of the target with the aim to converge in order to deliver the planned dose with only fractions of radiation to the normal surrounding tissues. Therefore, the process of tumor wrapping with high radiation dose with minimum dose delivered to the normal adjacent tissues is called conformal radiation therapy.15
Numerous advanced radiotherapy techniques had been used to reduce the radiation induced toxicities such as intensity modulated radiation therapy (IMRT), which is an advent form of 3-dimensional conformal radiation therapy (3D CRT) with the ability to change the intensity of radiation across each beam, whereas 3D CRT delivers radiation to the target with a minimum dose to the adjacent tissues.18,19
Over the past 20 years, IMRT became a common technique for HNC patients due to its ability to selectively target the primary site and lymph node regions at risk by decreasing the dose to the healthy adjacent tissues, thus improving therapeutic index by decreasing the acute and chronic morbidity, improving target volume coverage with locoregional control.20-25
Intensity modulated radiation therapy permits improved dose confirmation over irregular-shaped cancer with better sparing of adjacent normal structures.26 It is employed usually for the nasopharynx and oropharynx, avoiding important structures such as brain, brain stem, optic, optic stem and parotid salivary gland.19,27,28 Lamberchet et al29 reported significantly less xerostomia related to IMRT when compared to 3D CRT after 6 months of treatment (82% versus 91%). Additionally, Rathod et al30 compared the quality of life outcomes for head and neck SCC treated with 2 different radiation therapies, IMRT and 3D CRT, and they found significantly better dry mouth, mouth opening, sticky saliva, pain, senses, swallowing, feeling ill and insomnia on the symptoms scale.
Volumetric modulated arc radiotherapy is the advanced form of IMRT, which delivers an exactly shaped 3D dose distribution with a 360-degree rotation of the gantry in a single or multi-arc treatment. Therefore, the radiotherapy machine can spin over the patient body during the course of treatment. The machine constantly reshapes and changes the intensity of the radiation beam as it rotates around the patient.31,32
Fractionation of radiotherapy
Fractionation of radiotherapy is defined as radiation dose over time that is considered one of the essential factors that controls the outcome of radiotherapy.33 For standard radiotherapy, it is generally given in 2 Gray (Gy) fractions per day, 5 days per week for a total of 60 to 70 Gy.34 In order to improve local control and reduce the toxicity effect, it can be divided in 2 approaches of fractionation: hyperfractionation and accelerated fractionation. Hyperfractionation represents small doses of radiation given to the patient 2 or 3 times per day, usually 1.10-1.25 Gy, aiming to reduce the toxicity effect on the normal cells, whereas accelerated fractionation aims to reduce cancer repopulation between the sessions by reducing the total treatment time and adding more fractions per week (10 Gy per week), resulting in improved locoregional control.5,35-37 Bourhis et al38 reviewed 15 trials in their meta-analysis study that compared conventional radiotherapy with hyperfractioned and accelerated radiotherapy for SCC patients and concluded that the patients who received altered fractionated radiotherapy had better tumor control and survival compared to conventional therapy. Additionally, Fu et al33 found that the hyper fractionation and accelerated fractionation were more efficient than conventional fractionation for locally advanced cancer. Hypofractionation of radiotherapy also has been used as palliative treatment for advanced HNC, where a small amount of fractionation is given with higher radiation doses over a shorter period of time compared with the other regimens.39
Treatment delivery verification
Image-guided radiotherapy is important before radiation delivery, especially with IMRT, where any changes in the patient’s position can affect the radiotherapy field. Therefore, through the use of an immobilization custom fitted thermoplastic mask to position the patient in the field of radiation to limit the motion of his shoulder, jaw and head, images can be taken by cone beam CT, for example, to assess the bony landmarks and compare it with the initial planning scan. The patient can be positioned in the planned radiation field as long as it is the same position for each treatment dose.40
Adaptive radiotherapy
It is usually common that the tumor and the adjacent normal tissues change after a period of radiotherapy. Three percent volume shrinkage of the tumor and lymph nodes occurs daily, with changing in the tumor size, form and location during the course of the treatment.41 Weight and muscle mass loss also leads to changes in the patient outcomes.42 The parotid gland, for example, changes its position medially into a higher radiation field.43 Thus, re-planning of the radiation dose to compensate for changes in anatomy and target volume, which is called adaptive radiotherapy, results in superior quality of life and efficacy of treatment compared to not replanning.44-46
Proton radiotherapy
Proton beam therapy was introduced in radiotherapy to be used when the cancer is close to critical anatomical structures because the beam energy can be aimed at an exact depth, with consequent dose decrease. Therefore, it is different than external photon (x-ray) radiotherapy in which it can keep the same radiation dose for the normal adjacent tissues when the radiation dose is escalating to the tumor area. Additionally, it can deliver a reduced dose to the surrounding structure with the same radiation dose delivered to the tumor.47-49
Cellular and cancer response to radiation
When high-voltage x-ray penetrates the tissues, it ionizes the oxygen and produces free oxygen radicals and cancer death.50 Therefore, this high-voltage x-ray can damage the genetic material of the cells (DNA), which blocks division and proliferation.
The presence of oxygen increases the response to radiotherapy
Cancer cells are usually hypoxic and relatively resist radiation therapy. The use of radiation sensitizers may improve the response to radiation.35
The chemotherapeutic agent cisplatin (cis-diaminedichloroplatinum, CDDP) can act as a radiosensitizer. Cisplatin is commonly used with concurrent radiotherapy for locoregional control and laryngeal preservation.51 Bonner et al52 reported a significantly better 5 years overall survival for patients with locoregional advanced SCC of head and neck with chemoradiotherapy compared with radiation alone.
Radiation toxicity
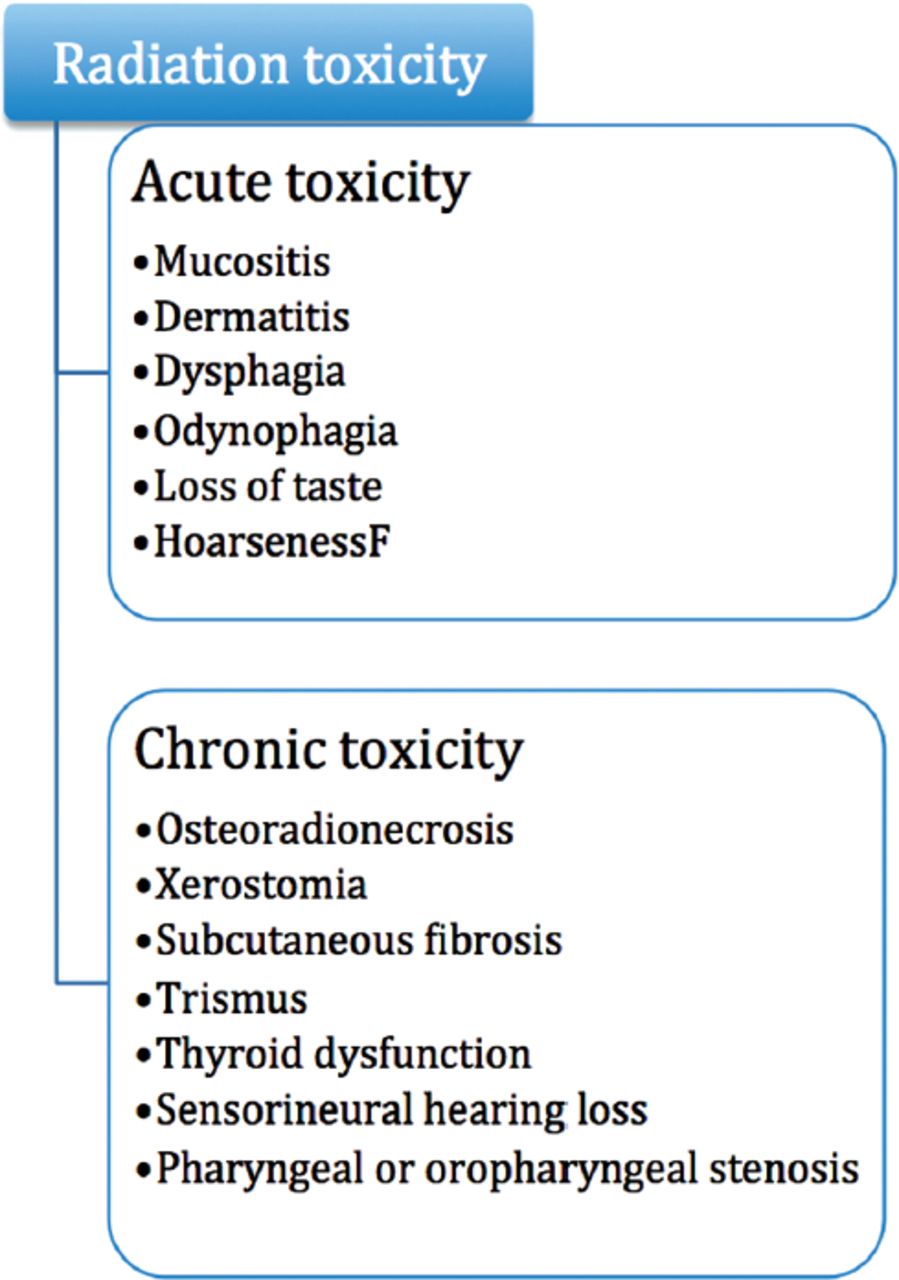
In addition to the anti-tumor effect of radiotherapy, it can cause injury to the normal tissues positioned in the area of radiation. Toxicity after radiotherapy is defined as adverse events or complications that occur after radiation, which can be any changes in the normal tissues with temporary or permanent nature. It can be considered as acute toxicity when it occurs within 90 days of treatment or late toxicity when it happens after 90 days of radiation53-55 (Figure 1). Toxicity is found to be more severe when radiotherapy is combined with chemotherapy. Cooper et al56 reported that the incidence of acute toxicity of grade 3 or more was 77% in patients who received chemoradiotherapy while only 34% in patients who received radiotherapy alone.

- Examples of head and neck radiation toxicity.
Post-radiation complications vary from skin rashes to osteoradionecrosis
The common acute toxicities include mucositis, dermatitis, dysphagia and odynophagia, hoarseness and loss of taste caused by laryngeal edema, whereas the late toxicities include osteoradionecrosis, xerostomia, subcutaneous fibrosis, thyroid dysfunction, trismus, sensorineural hearing loss, myelitis, and pharyngeal or oropharyngeal stenosis.57,58 Usually, tissues with rapid turnover rates show acute reactions, whereas tissue with slower turnover has late reactions that may take months or years.58
Mucositis, which is defined as inflammation of the oral and oropharyngeal mucosa, is one of the first acute toxicities that affect the patient. It appears within the first 2-3 weeks of treatment as erythema of the oral mucosa that proceeds to ulceration and pseudomembranes, and it usually affects the non-keratinized oral mucosa more than the keratinized ones.59,60
Mucositis may result in local discomfort with difficulty in eating and drinking that may cause nutritional problems to the patient leading to weight loss that may necessitate the use of a gastrostomy tube, whereas with severe mucositis, radiotherapy needs to stop and the patient may need hospital admission, which prolongs the time of treatment.53,61-63 During radiation therapy, some mouthwashes can be prescribed to the patient to help relieve some of the oropharyngeal symptoms. For example, Akabutu’s mouthwash that is produced by Dr. John Akabutu while he works at the University of Alberta Hospital and the Cross Cancer Institute, contains viscous lidocaine, nystatin suspension, hydrocortisone, glycerin and normal saline.64 However, the epithelial surface usually healed in 20-40 days after the completion of the radiotherapy depending on the severity of the lesion.65
Over 90% of HNC patients who received radiotherapy suffer from xerostomia, oral discomfort, difficulty in mastication, speech and swallowing, loss of taste and worsening of periodontal hygiene.54,62,66 Additionally, over 50% of them produce dental caries and oral mucositis with an increased risk of trismus, skin fibrosis, fungal infection, periodontitis, odynophagia and osteoradionecrosis.67 To help prevent xerostomia, numerous strategies have been used, such as surgical transfer of salivary glands, a radiotherapy method that spares the salivary glands, a radioprotectant such as amifostine, and intraglandular botulinum therapy.68 In 2001, Seikaly et al69 introduced a novel technique of transferring the submandibular salivary gland surgically to the submental space before the radiotherapy. During radiotherapy, usually, the submental region shielded and received scattered radiation, which is considered just 5% of the total radiation dose.70 The submandibular salivary gland can produce 200 to 300 mL of saliva per day, so by Seikaly et al69 and Jha’s70 method of submandibular salivary gland transfer, it can preserve the gland function after radiation treatment with the proper shielding.71 This method can be applied for patients with primary tumors of the oropharynx, hypopharynx, larynx and skin as they do not have lymphatic involvement of level I nodes.69 Sood et al72 in 2014 reviewed studies of 12 institutes that used Seikaly et al69 and Jha’s70 methods to prevent radiation induced xerostomia, and they found that in 177 patients, salivary gland transfer prevented xerostomia in 82% of them. Additionally, after approximately a year of radiotherapy, the stimulated salivary flow returned to 88% and un-stimulated to 76% of pre-surgical value. A strict high-fluoride regimen should be followed after radiation therapy to help prevent dental caries, especially with a hyposalivation environment.73,74 Attempts can be carried out to restore the salivary flow of patients through the use of muscarinic cholinergic agonists to stimulate salivary flow. Saliva replacement can be used if stimulation fails. Sialagogues, such as salivary replacement rinses, carmellose and mucin sprays, polyacrylic acid, carboxymethylcellulose, and sugarless gum, can improve symptoms.68,75-78
Limited mouth opening (trismus) can also occur if the temporomandibular joint or masticatory muscles or both were included in the area of radiation, which results in muscle fibrosis and scarring with fibrosis of the ligaments around the joint, which may interfere with patient’s nutrition, speech and dental care.79,80 Less than 35 mm is considered as the functional cut-off point of trismus.81 It is considered as a late toxicity event that happens after radiotherapy and can be a life-long problem. Some therapeutic interventions seem to improve trismus such as pentoxifylline, botulinum toxin and through exercises with the Therabite Jaw Motion Rehabilitation device.82,83
Osteoradionecrosis is a serious and late toxicity event that occurs after radiation therapy when the irradiated tissue breaks down and fails to repair after the injury, so the irradiated bone is exposed and undergoes necrosis. The risk increases with a radiation dose above 60 Gy, with the prevalence rate between 5% and 15% in the patients who received radiotherapy, which occurred between 22 and 47 months after radiation. In the head and neck region, usually, the mandibular bone is more susceptible to osteoradionecrosis.53,73,84-86
The risk of osteoradionecrosis increases after oral surgery procedures after radiotherapy, which emphasizes the need for pre-radiation dental management to reduce the need for teeth extraction after radiotherapy.73 Prophylaxis extraction of the teeth with unfavorable conditions within the area of planned irradiation was recommended.87 Several studies suggested a minimum of 2 weeks waiting time between teeth extraction and initiation of radiotherapy.84,88
Osteoradionecrosis induces fibrosis and thrombosis, bone marrow damage, necrosis of lacunar osteocytes, and loss of bone and soft tissue healing.89,90 Its treatment usually includes surgical resection and vascular graft reconstruction when it involves pathological fractures or threatening of fractures. Hyperbaric oxygen therapy may help prevent the incidence of osteoradionecrosis before any surgical procedure to the irradiated area.53
Hyperbaric oxygen therapy (HBO)
Hyperbaric oxygen therapy is utilized for patients who suffer from severe carbon monoxide poisoning, arterial embolism, and decompression sickness. Additionally, it can be used to limit chronic radiation injuries.78,86,91
One hundred percent oxygen can be delivered to the patients in a hyperbaric chamber according to specific protocols. Hyperbaric oxygen therapy dose can be delivered over several days before and after the surgical procedure for irradiated patients. The standard Marx 30/10 HBO protocol is used, where 30 times of HBO treatment are delivered to the patient at 2.4 atmosphere for 90 minutes before surgical procedure, followed by 10 times of HBO treatment after the surgical procedure with the same time and atmosphere setting.78,92
Taher et al91 in 2015 assessed the efficacy of (HBO) in the management of chronic radiation-induced tissue injuries. They found a high response rate in osteoradionecrosis prophylaxis because of radiation induced dental disease. Additionally, they noticed improvement in necrosis of the head and neck tissues, mandibular osteoradionecrosis and xerostomia. In 2012, Hampson et al93 evaluated the outcomes of 411 patients over 8 years that showed complete healing after teeth extraction; the used of HBO protocol was 20/10 for 166 patients and 30/10 for 43 patients before and after the extraction. Hyperbaric oxygen therapy could also be used as an adjuvant treatment to the surgical treatment for osteoradionecrosis to fasten the healing of the osseous and soft tissues.94
The patients demonstrate some complications after HBO, which are related to increased oxygen and pressure levels. Barotrauma of the middle ear, sinus, lung and teeth may occur, which result from failure to balance pressure between the atmosphere and the air-filled space in the patient body resulting in a “squeeze.” Increased oxygen levels may result in transient myopic change and pulmonary oxygen toxicity, which resolve after several days. Additionally, with patients, lower seizure thresholds may suffer from generalized tonic-clonic seizure in rare conditions.78
In conclusion, over the past decade, improvements in head and neck management through radiotherapy have been added. Modern radiotherapy techniques resulted in the improvement of cancer control. Several types of management of toxicity-induced radiotherapy were implemented to improve the patients’ quality of life. The field of radiotherapy is still growing to control tumors and improve radiation-induced toxicity.
Acknowledgment
The author acknowledges the American Journal Experts company for the professional editing of the manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.
- 22.
- 23.
- 24.
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.
- 77.
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵




{kind=link}