


Abstract
Objectives: To evaluate risk factors associated with 31-day unplanned readmission(s) for pulmonary tuberculosis (TB) in China.
Methods: This retrospective study enrolled patients (age, >14 years) with pulmonary TB who experienced 31-day unplanned readmissions to a specialized hospital for TB between January 2018 and December 2019. For each confirmed readmission, 2 control subjects were randomly selected from among patients with pulmonary TB but did not experience an unplanned readmission within 31 days.
Results: A total of 402 pulmonary TB patients (5.9%) experienced unplanned readmission within 31 days after discharge. In univariate analysis, readmission was associated with gender, age, insurance coverage, residing in a rural area, active smoking, chronic obstructive pulmonary disease (COPD), drug-induced hepatitis, and leaving hospital against medical advice. The final logistic regression model revealed that higher risks for unplanned readmissions were associated with male gender (odds ratio [OR] 1.44, [95% confidence interval (CI) : 1.06-1.95]), age >65 years (OR 2.94, 95%CI: 2.03-4.27), rural residence (OR 8.86, 95%CI: 6.61-11.87), active smoking (OR 2.15, 95% CI 1.37-3.40), COPD (OR 2.77, 95%CI: 1.59-4.81), and leaving hospital against physician advice (OR 4.11, 95%CI: 1.43-11.83). The median time to 31-day unplanned readmission was 24 days. Major reasons for unplanned readmission included fever, exacerbation of dyspnea, and hemoptysis.
Conclusion: Unplanned readmission for pulmonary TB within 31 days of discharge was higher among older males residing in rural areas, active smokers, and those leaving hospital against medical advice.
Tuberculosis (TB) is one of the most important infectious diseases in the world, and caused by Mycobacterium TB. In accordance with World Health Organization (WHO) report in 2020, the incidence of TB was approximately 10 million (range, 8.9-11.0 million), with 1.4 million deaths worldwide.1 In 2020, the incidence rate of TB was estimated to be 58 per 100,000 population in China.2 Although the prevalence of TB has decreased through 2 decades of effort and short-course strategy programs (such as, directly observed treatment, short course [DOTS]), China still ranks second in terms of the largest burden of TB in the world, which is also associated with enormous economic implications.3
Unplanned re-hospitalization within 31 days of discharge refers to a situation in which a patient is readmitted to hospital for the same or related disease within 31 days after initial discharge,and is considered to be a “sentinel event” reflecting poor-quality hospital care.4 Moreover, unplanned readmission(s) after hospitalization also impose a burden on patients and health care resources due to high costs.5 In 2004, hospital readmissions in the United States cost the medicare system approximately $17.5 billion, accounting for approximately one-fifth of the country’s total hospital costs.6 A cross-sectional study reported a hospital readmission rate of 5.9%, which varied among hospitals, ranging from 9.8% to 17.0% in France.7 The readmission rates continue to rise, causing widespread concern across countries. The United States and China announced in 2007 and 2011, respectively, that early unplanned readmission should be used as an important indicator for evaluating medical quality.8,9
Considering the additional costs that unplanned readmission impose to the health system, correlational research may improve our clinical decision-making on unplanned hospitalization. A systematic study in 2020, chronic obstructive pulmonary disease (COPD)-related readmission rates have differences in 30 countries, risk factors and the local healthcare environment should be interventions.10 According to a 3-year study carried out in Iran, a common cause of early readmission were drug-induced hepatitis, dyspnea.11 In addition, comorbidities and socioeconomic factors were also considered to be associated with readmission.12,13 So far, readmissions for major disease and surgical diagnoses have been studied, but the risk factors for early unplanned readmission among patients with pulmonary TB without research. Thus, this study aimed to investigate risk factors associated with 31-day unplanned readmission of patients previously discharged with pulmonary TB in China.
Methods
The present investigation was a retrospective analysis of adult (age >14 years) patients with confirmed pulmonary TB admitted to Changsha Central Hospital, Hunan, China between January 2018 and December 2019. Patient diagnoses were coded according to the WHO’s International Classification of Diseases (10th Revision), and matched to cases according to the principal diagnosis. Readmission data were collected from the electronic medical record monitoring database, and were verified to confirm whether they documented unplanned readmission(s) within 31 days of admission for TB. The unplanned readmission group included patients who were readmitted for TB related diseases within 31 days after discharge. In contrast, patients lack of readmission information; HIV positive patients; scheduled for readmission; readmitted for a non-TB-related condition were excluded. For each confirmed readmission, 2 control subjects were randomly selected from among patients with pulmonary TB who did not experience unplanned readmission within 31 days. Demographic information and clinical characteristics of the patients, including gender, age, TB type, medical comorbidities, and so on, were obtained from the hospital’s electronic record systems.
Direct sputum smear method was used for sputum smear (Ziehl-Neelson), then was smeared and observed with a microscope. The operation is strictly in accordance with the “Manual of Standardized Operation and Quality Assurance for Sputum Smear Microscopy” (Olympus CX31, Japan) biological microscope was used for the instrument, and anti-acid staining is Zhuhai BASO Company (China). Detection standard for positive sputum smear microscopy: if the number of acid-fast bacilli in 100 visual fields is 3-9, it indicates a positive result for TB bacilli.
PubMed database was used for identification and retrieval the article. This study was approved by the Medical Ethics Committee, Changsha Central Hospital and in accordance with the Helsinki Declaration.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, N.Y., USA). Univariate analysis (a simple binary logistic regression) was used to identify the potential factors associated with readmission (patients unplanned readmitted ≤31 days and no unplanned readmission ≤31 days). Variables whose value of p<0.05 were included in the multiple analysis (binary logistic regression model [multiple]) to adjust for possible biases. Variables were selected with the enter method, and the goodness of fit was evaluated by the Hosmer-Lemeshow test. Odds ratios (OR) and their respective 95% confidence intervals (95% CI) were estimated. Reference categories were assigned OR=1. Statistical significance was based on 2-tailed p<0.05.
Results
Between January 2018 and December 2019, 6806 patients with pulmonary TB were admitted to the Changsha Central Hospital, Changsha, China of which 402 (5.9%) were unplanned readmissions after discharge. Accordingly, a total of 804 controls were randomly selected from among patients who had not experienced unplanned readmission. As such, 1206 patients (unplanned readmission ≤31 days [n=402], non-unplanned readmission ≤31 days [n=804]) were fit into the study. The mean (± standard deviation [SD]) age was 48.20 ± 18.98 years; 786 were male and 420 were female.
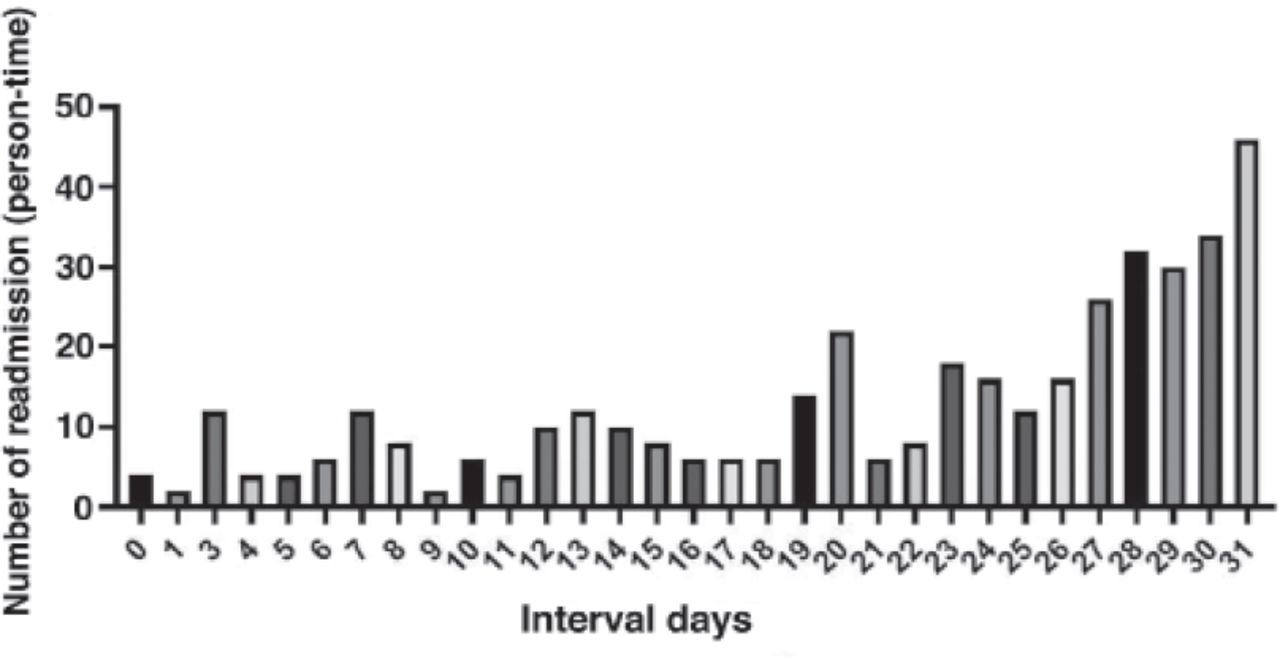
The median time to 31-day re-hospitalization was 24 days, with a range of 0-31 days. Four patients were readmitted on the day of discharge, comprising of 1.0% of the total readmission rate, 104 (25.9%) were readmitted to hospital within 1 to 15 days after discharge, and 298 (74.1%) were readmitted 16 to 31 days after initial discharge (Figure 1).
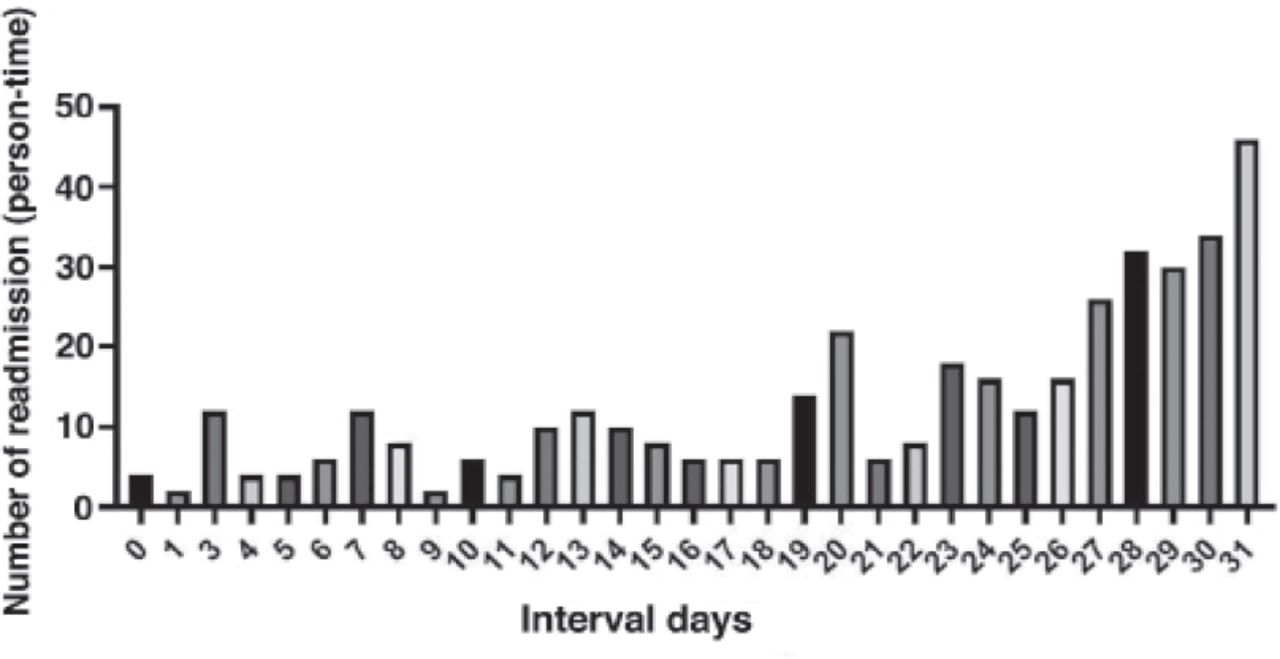
- Discharge-readmission days distribution chart.
Univariate analyses revealed that patients who experienced unplanned readmission differed significantly from non-readmitted patients in terms of gender, age, insurance coverage, rural versus urban residency, active smoking, COPD, drug- induced hepatitis, and leaving hospital against medical advice (Table 1).
- Unplanned readmission≤31 days risk factors for pulmonary tuberculosis patients.
Multivariate analysis included all significant variables from univariate analysis (p<0.05). In the final model showed that male gender, age >65 years, rural residence, active smoking, COPD, and leaving hospital against medical advice retained significance (Table 1).
Discussion
The unplanned readmission rate for a 2-year period in this study was 5.91%, which as lower than the rates reported by Silva and Qayed.14,15 The median time to 31-day unplanned readmission was 24 days, and >70% of patients were readmitted between 16 and 31 days after discharge.
Unplanned readmission for pulmonary TB was higher in males, which is usually the case with TB infection. The readmission rate according to gender was higher in some studies, but only one study reported a direct relationship.16 Based on univariate and multivariate regression analyses, our study also confirmed that males were readmitted more often. Regarding the place of residence, patients residing in rural areas experienced higher readmission rates than those in urban areas, which is different from the results reported in a study from Brazil.14 This difference may have several explanations. First, the prevalence of TB is higher in rural versus urban areas of China,17 and those residing in rural areas are more affected by poor socioeconomic conditions. These patients often delay their medical treatment after falling ill, which leads to them becoming a new source of infection and infecting other susceptible groups.18 Furthermore, poverty leads to low protein intake, which negatively affects the body’s immune system. Poverty is also associated with lower education levels, which indirectly reduces an individual’s ability to prevent TB.19-21 Therefore, TB health education in the future should remain focused on rural areas.
Unplanned readmission of TB patients was associated with age > 65 years, similar to the findings reported by Anaam.16 But, this results differ from another study, in which age was not confirmed as a risk factor for hospital readmission among TB patients.11 The association between readmission and age can be explained by decreased immunity, comorbidity, and concomitant diseases. Studies investigating hospital readmission among TB patients report different risk factors; however, all depend on comorbidity.11,22 Results of our study demonstrated that COPD is one of the risk factors for increased unplanned readmission. A study by Bhatt et al,23 documented in middle-aged and older patients with COPD have a higher risk for re-hospitalization. A follow-up study reported that COPD patients with a history of pulmonary TB were hospitalized more often and experienced lower long-term survival rates compared to those without a history of TB.24 Chronic obstructive pulmonary disease is not only a important risk factor for TB, but is also one of the important causes of Mycobacterium TB drug resistance.25 Additionally, the readmission rate of smoking population was significantly higher than that of non-smoking population, and tobacco has an impact on both TB/COPD morbidity and mortality.26,27 Various studies have verified that smoking is a risk factor for TB and COPD. However, results of our study do no brief for the formulation that smoking causes additional mortality risk in those with pulmonary TB,28 but do suggest that smoking is a risk factor for unplanned readmission.
The unplanned readmission rate for patients who leave the hospital against physician/medical advice was also higher. These patients were discharged from the hospital at their own request due to financial or personal reasons without completing treatment or meeting discharge indications. Existing studies have indicated that treatment failure is, in large part, attributable to antimicrobial-resistant pulmonary TB.29 A nested case-control study documented that properly managing patients who experience their first TB infection by encouraging strict adherence to medication do not fail treatment, and can be rescued from relapse.30 To reduce the rate of patients leaving hospital without medical advice, we need to make joint efforts at the national and hospital levels, such as strengthening the medical system, reducing the proportion of patients paying out-of-pocket expenses, and improving the treatment capability of hospitals treating severely ill patients. According to the Chinese hospital monitoring system readmission reporting requirements, we subcategorized the time interval into 3 groups (according to time of first discharge and interval of readmission). In the first group (readmission on the same day), we evaluated patients who were readmitted on the day of discharged patients within the same days, in which sudden relapse occurred on the day of discharge, including dizziness, vomiting, and pneumothorax. Treatment refusal and treatment failure were the main causes of late readmission (such as, 16 to 31 days after discharge). Exacerbation of dyspnea and fever is a common objective reason for both early and late readmission, followed by drug side-effects and hemoptysis.
The present study had several strengths. Our hospital is a specialized tuberculosis hospital with a relatively stable patient source, so a large sample size can be obtained in this study. The readmission of COPD and asthma has been studied by some scholars,31,32,33 but only a few studies have looked at readmission rates for TB, and there is a lack of research on unplanned readmission in patients with pulmonary TB. This study analyzed the influencing factors of unplanned readmission of TB patients, which could help to identify and intervene the high-risk groups of unplanned readmission. Meanwhile, this study also provides a theoretical basis for subsequent prospective studies of unplanned readmission to TB.
Study limitations
First, was it is a single-center, retrospective design, which may have hindered some analyses. We advise that early unplanned readmission is an critical parameter to monitor in TB programs, and prospective studies should be initiated in the future. Second, this survey is a single-center study. The HIV infection rate in this province is relatively low, and TB patients will be transferred to the provincial infectious disease hospital immediately once they are diagnosed with AIDS, so the readmission information of such patients cannot be collected. Third, although a few behaviors and socioeconomic characteristics of patients were collected, this retrospective study was unable to obtain more information relevant to patient readmission, such as socioeconomic status, body mass index, pharmacological intake, and education.
In conclusion, the unplanned readmission rate of pulmonary TB in our study was lower compared to similar studies. The most common reasons for unplanned readmission to our hospital included fever, exacerbation of dyspnea, and drug side effects. We conclude that the unplanned readmission within 31 days of pulmonary TB was higher in older males residing in rural areas, and among active smokers, and those leaving the hospital against medical advice. The existence of these factors reminds the medical staff to attach great importance to the newly hospitalized patients with these factors. Some of these factors can be changed by intervention, indicating that continuous health management and regular treatment can be achieved for patients with chronic comorbidities, smoking cessation, strengthen health education in rural areas, and reducing the ratio of out-of-pocket patient expenses, may help decrease unplanned readmission rates within 31 days for pulmonary TB.
Acknowledgment
The authors gratefully Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 19, 2021.
- Accepted July 28, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.