


Abstract
Objectives: To investigate the ethmoid infundibulum (EI) and maxillary sinus natural ostium (MSNO) dimensions in normal sinuses of the Asian population; identified variation between sides, gender, and age groups; and to assess the effects of such variation on the measurements.
Methods: We assessed EI dimension and MSNO diameter in computed tomography (CT) scans of the normal paranasal sinus of 100 patients who underwent trans-sphenoid endoscopic surgery. We compared demographic data and multiple anatomical variations.
Results: The gap difference in EI length between the right and left sides significantly differed from 0 (0.47±1.38 mm). We found wider EI in people aged ≥60 years (2.44±0.59 mm), compared to people aged <60 years (2.25±0.31 mm). Ethmoid infundibulum length was greater among individuals with Haller cells (8.84±1.56 mm) than in individuals without them (7.92±1.47 mm). Furthermore, MSNO diameter was greater with accessory ostium (3.48±0.77 mm versus 3.02±0.72 mm, presence versus accessory ostium absence).
Conclusion: Multiple factors may affect EI and MSNO dimensions. Ethmoid infundibulum length differed between both sides. Ethmoid infundibulum width differed between individuals aged ≥60 years and individuals aged <60 years. Haller cells and accessory ostium presence were associated with significant differences in those measurements.
The ethmoid infundibulum (EI) is a component of the ostiomeatal complex (OMC). This area is important in the drainage of anterior nasal sinuses, (namely, frontal, maxillary, and anterior ethmoid sinuses).1-3 The anterior border of the EI is the uncinate process (UP) and posterior border of the EI is the bulla ethmoidalis. The maxillary sinus natural ostium (MSNO) opens into this space; obstruction of drainage in this area can lead to sinusitis.2
Ethmoid infundibulum dimensions (namely, width and length) have been studied in several sinus diseases such as acute sinusitis and retention cysts.4-9 Shin et al,4 measured EI dimensions in the contralateral side of the maxillary fungal ball; they found that a narrow and long EI was associated with various diseases. Alkaire et al,6 reported that recurrent acute rhinosinusitis is associated with a narrow EI. The EI width measurement method is consistently defined as the line between the UP and bulla ethmoidalis. Pruna,9 describes EI length measurement as the UP length. Previous studies indicate substantial interest in understanding EI dimensions.4-8
The MSNO has been studied in sinus diseases such as fungal balls and odontogenic sinusitis.10,11 El-Anawar et al,12 reported no statistically significant difference in MSNO diameter between sides in healthy people. This diameter is defined as the length of a line drawn between the UP attachment to the medial maxillary wall and the bony part of the orbit floor or anterior ethmoid air cells (namely, Haller cells [HCs]).12,13
Understanding the anatomies of EI and MSNO can facilitate research and treatment of sinusitis. Nevertheless, few studies have assessed the anatomical factors that affect the dimensions of those areas in normal populations. For instance, the effects of HCs on EI and MSNO, differences in dimensions between sides in a single individual, or the impact of gender on these dimensions have not been widely investigated.4,14,15 Furthermore, those measurements are frequently used in publications related to sinus diseases and procedures (namely, balloon sinusotomy).16 Our study investigated the EI and MSNO dimensions in normal sinuses of the Asian population; identified variation between sides, gender, and age groups; and assessed the effects of such variation on the measurements.
Methods
This retrospective cross-sectional study was approved by the Institutional Review Board of the College of Medicine, St. Mary’s Hospital, Catholic University of Korea, Seoul, (approval no. KC20RISI0758). Images of 100 patients (200 sides) who underwent surgery from July 2014 to March 2019 using a trans-sphenoidal approach were analyzed based on computed tomography (CT) scans of paranasal sinuses. Patients were included had a normal sinus appearance; patients were excluded if they had sinus opacifications (partial or complete), previous surgeries, trauma, or another sinus pathology. All paranasal CT scan protocols entailed acquiring axial images 0.6 mm thick, then reconstructing coronal images 1 mm thick. In these thin CT scans, the EI and MSNO were usually visible, depending on the presence or absence of disease-related opacification. Ethmoid infundibulum dimensions and MSNO diameter were measured from coronal CT scans (Figure 1).4,12 Measurements were performed using the measurement tool in the picture archiving and communicating system (Marotech, Seoul, Korea); the mean value of 2 measurements was recorded for both EI and MSNO. One author (with 7 years of experience) reviewed the presence of anatomical variations including deviated nasal septum (DNS), concha bullosa (CB), HCs, and maxillary accessory ostium (AO). Deviated nasal septum (DNS) was defined as a deviation to one side of >10 degrees in a vertical line from the crista galli to the nasal floor (Figure 1).4
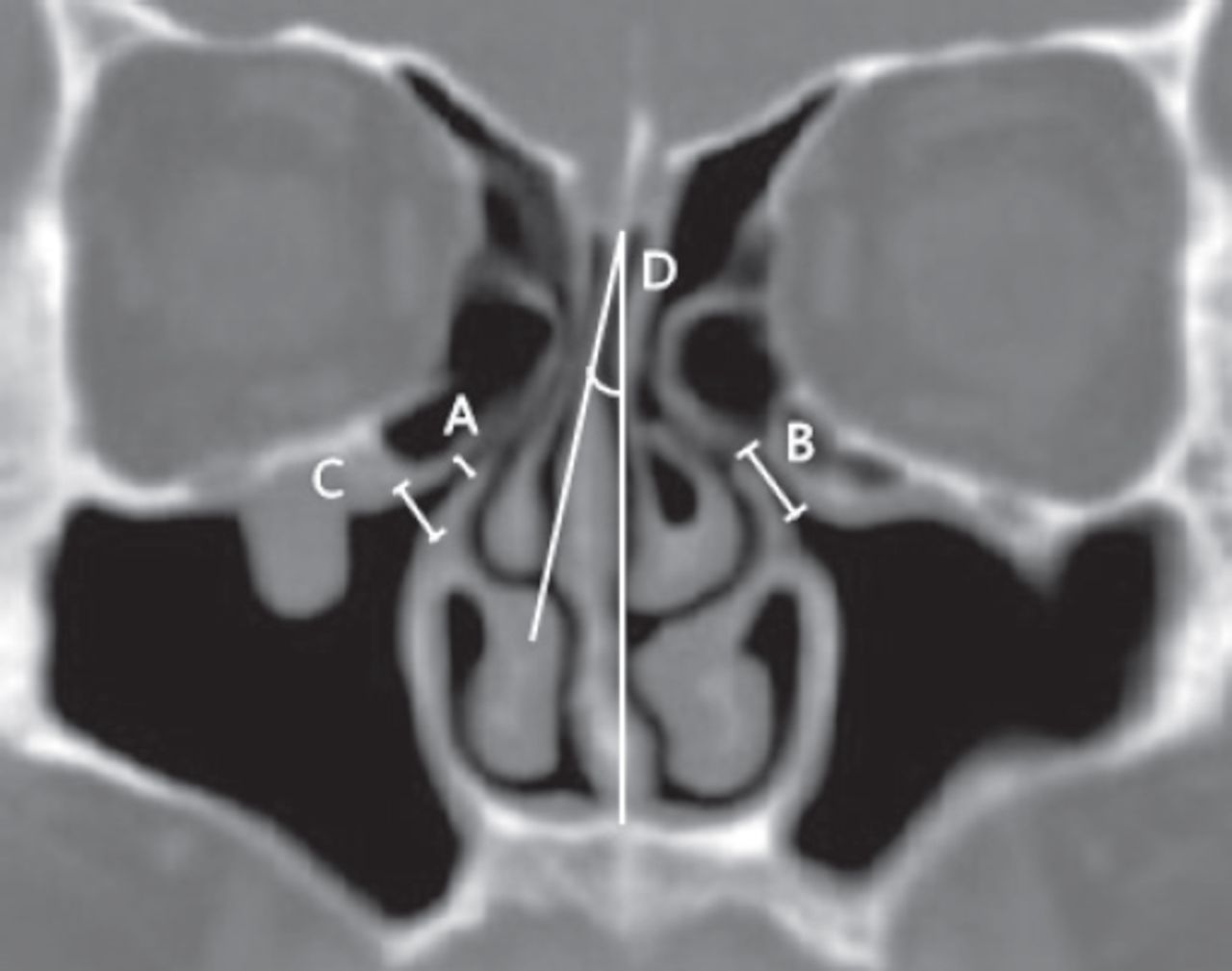
- Methods of measuring ethmoid infundibulum dimensions, maxillary sinus natural ostium diameter, and deviated nasal septum. A) Ethmoid infundibulum width was defined as the line between uncinate process and bullae ethmoidalis. B) Ethmoid infundibulum length was defined as the uncinate process length from its free edge to the attachment above the inferior turbinate on coronal CT. C) Maxillary sinus natural ostium diameter was defined as the length of a line drawn between the uncinate process attachment and the bony part of the orbit floor or anterior ethmoid air cells. (D) Deviated nasal septum was defined as a deviation of >10 degrees from a vertical line from the crista galli to the nasal floor.
Statistical analyses
All EI and MSNO measurements were recorded in millimeters and are shown as means±standard deviations (SDs). One-sample student’s t-tests were used to compare gaps between right and left side measurements, relative to a mean value of 0 (namely, no difference between sides). Student’s t-test was also used to compare EI dimensions and MSNO diameter between gender and age groups. Similarly, the mean values of those measurements were compared according to the presence or absence of multiple anatomical variations. Finally, Pearson correlation analyses were conducted to check the correlation between EI dimensions and MSNO diameter. A p-value <0.05 was considered significant. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) for Windows, version 24.0 (IBM Crop., Armonk, NY, USA).
Results
The mean EI length of 200 sides was 8.11±1.53 mm (range: 5.01-13.97 mm) and the mean EI width was 2.33±0.56 mm (range: 1.21-5.91 mm). The mean MSNO diameter was 3.12±0.75 mm (range: 1.5-5.85 mm). Table 1 shows the respective means of the right and left sides, as well as the gap between the 2 sides. The gap between EI length measurements on both sides was statistically significant (0.47±1.38 mm, p<0.01).
- Comparisons of ethmoid infundibulum and natural ostium dimensions between left and right sides.
Table 2 shows the EI dimensions and MSNO diameter on both sides between gender and age groups (individuals aged ≥60 years and individuals aged <60 years, according to the World Health Organization recommendations regarding age analyses).18 There were no significant differences between gender in any of the 3 measurements. When comparing measurements between age groups, the mean sum of EI width on both sides was significantly greater among individuals aged ≥60 years (2.44±0.59 mm) versus individuals aged <60 years (2.25±0.31 mm; p=0.038). However, this sum remained significant only on one side when means were stratified according to side (left versus right; Table 2). The EI width was weakly positively correlated with MSNO diameter (r=0.271, p<0.01). Thus, greater EI width is associated with greater MSNO width. Other dimensions were not significantly correlated with each other.
- Comparisons of ethmoid infundibulum and natural ostium dimensions according to gender and age.
Table 3 shows a comparison of EI dimensions and MSNO diameter according to the presence or absence of anatomical variation. Haller cells were present in 41 of 200 sides (20.5%); HC presence was associated with significantly greater EI length, compared to HC absence (8.84±1.56 mm versus 7.92±1.47 mm, p<0.01). Furthermore, AO was present in 40 of 200 sides (20%); AO presence was significantly associated with greater MSNO diameter (3.48±0.77 mm versus 3.02±0.72 mm, AO presence versus AO absence; p<0.01).
- Comparisons of ethmoid infundibulum and natural ostium dimensions according to the presence and absence of multiple anatomical factors.
Discussion
Developments in CT imaging and endoscopic sinus surgery have led to increasing interest in sinus anatomy. Several reports have described radiological anatomical variation in the OMC in various sinus pathologies.4-8 However, sinus disease could modify those dimensions through either soft tissue destruction or the presence of OMC opacification, thus interfering with measurement of those dimensions. Our study mainly describes variation in the EI and MSNO dimensions in normal sinuses, rather than diseased sinuses.
Comparison of EI and MSNO dimensions between sides, gender, and age groups
Our results indicated symmetry between right and left sides regarding EI width and MSNO diameter; however, EI length significantly differed between sides (Table 1). We also found a significant difference in EI width between individuals aged ≥60 years and individuals aged <60 years. However, this difference was only evident on the right side when the measurement was stratified according to side. Furthermore, there were no differences in measurements between gender (Table 2).
Similarly, El-Anawar et al,12 found no significant difference in mean MSNO diameters when comparing right and left sides. Shin et al,4 found no differences in EI width in normal controls between right and left sides (p=0.742). Although their study population was similar to ours, they reported that EI length did not significantly differ between sides in normal individuals (p=0.406). In their study, they measured maximal length only, while we measured the mean of 2 readings because the EI occasionally appeared in multiple images. There is no definitive method for EI length measurement.4,7,9 Therefore, further studies are needed to confirm the symmetry of EI length in a single individual because measuring the normal side as a reference is common in patients with unilateral disease.4
Although the difference was not statistically significant, all measurements were greater among individuals aged ≥60 years than among individuals aged <60 years. This could be due to aging, which is associated with atrophic changes in the mucosa over time. In terms of gender comparison, several studies described findings similar to ours. For example, Sakuma et al,13 found no differences in MSNO between men and women. Furthermore, one study found no differences in EI length between men and women.18 Although differences between gender have been observed in terms of maxillary sinus dimensions, EI and MSNO measurements are similar between gender.
Comparison of EI and MSNO dimensions according to anatomical variation
We found that HC presence was associated with greater EI length (p<0.05). However, HC presence and absence were not associated with any differences in EI width or MSNO diameter. Furthermore, the presence of AO in the maxillary sinus was associated with greater MSNO diameter in our study. However, we did not observe any significant differences in EI and MSNO dimensions according to DNS and CB statuses (Table 3).
Some anatomical variation in the OMC area could obstruct the paranasal drainage sinuses (namely, HCs, paradoxical middle turbinate, and CB). However, the effects of such variation on the sizes of EI and MSNO are not well-studied in normal populations. In contrast to our result, Akay et al,18 reported no significant differences in EI length according to HC presence or absence (p=0.114). Haller cells are commonly presumed to cause sinusitis because they contribute to EI and MSNO narrowing. However, our data and the findings of a previous study suggest that HCs do not directly reduce those dimensions.6 Shin et al,4 reported a substantial difference in EI width, according to CB presence or absence. They did not find a significant difference in EI length according to CB presence. Previous investigations have indicated that AO is caused by recurrent sinusitis and obstructed sinus drainage.19 By contrast, our data showed that AO was associated with greater MSNO diameter.
Study limitations
Measurements were taken from radiological images and thus may differ from normal endoscopic (or cadaveric) measurements. Accurate measurements are difficult with reconstructed coronal CT, because only one cut may be available through EI and MSNO areas. Various methods have been used to measure those dimensions in previous studies. There is a need for other studies to unify those measurements using CT scans. Such radiological measurements should also be compared to cadaveric or endoscopic measurements in normal populations.
In conclusion, we found that multiple factors affect measurements of EI dimensions and MSNO diameter, including side (left versus right) and age. Haller cells and AO presence were associated with significant differences in EI length and MSNO diameter, respectively. Measurements have also differed according to study methods and populations. Further studies are needed to define those dimensions and methods of measurement, as well as anatomical factors affecting these frequently reported dimensions.
Acknowledgment
The authors gratefully acknowledge Textcheck (http://www.textcheck.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 7, 2021.
- Accepted July 3, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.