


Abstract
Objectives: To find the association between environmental and occupational exposures and chronic rhinosinusitis (CRS) development.
Methods: The Preferred Reporting Items Of Systematic Reviews Guidelines were used when a systematic literature review was conducted to find all published cases of CRS by searching PubMed database and Google Scholar. Published articles between 1989 and 2021 that reported chronic and occupational rhinosinusitis were included. However, articles that reported allergic rhinitis or upper airway diseases and non-English articles were excluded from this study.
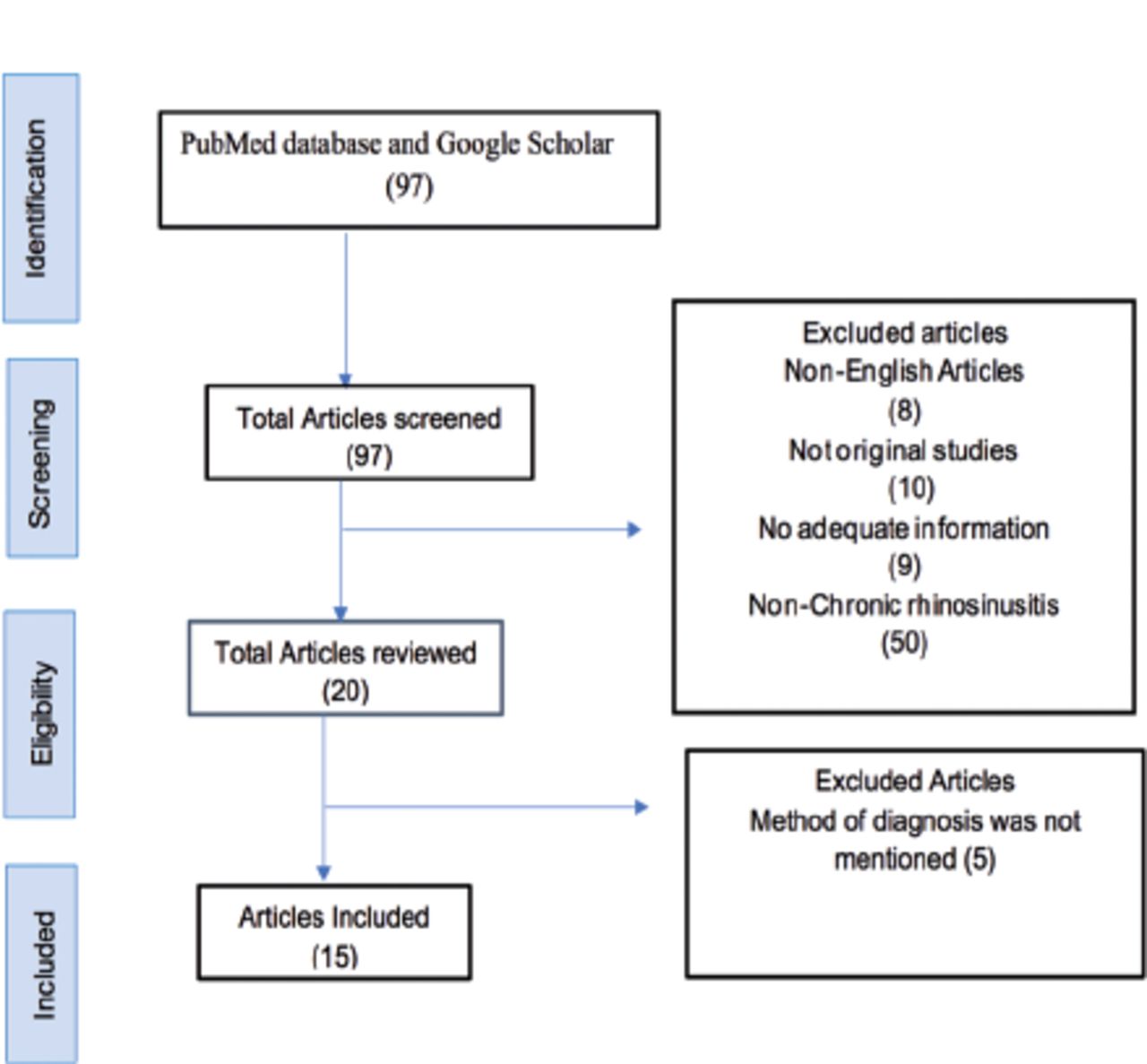
Results: A total of 97 articles were extracted initially, and 15 articles were reviewed after excluding 82 articles that did not match our inclusion criteria. Most studies linked CRS development to smoke exposure (n=9734), followed by living in rural areas as farms (n=5504). Exposure to pesticides (n=4248) contributed to a higher prevalence of CRS. Blue-collar occupations, such as fire fighters, farmers, and fishermen were significantly related to CRS development in a total of 5260 patients. Chronic rhinosinusitis mainly affected more men (n=8912) than women (n=8076).
Conclusion: We found that smoking was the most aggravating environmental factor. Chronic rhinosinusitis symptoms’ severity increased with direct contact with allergens. Thus, the greatest proportion of patients with CRS was those with blue-collar occupations, such as firefighters, farmers, and fishermen.
Chronic rhinosinusitis (CRS), one of the most common chronic diseases, is a condition of chronic inflammation of the paranasal sinus mucosa that lasts for at least 12 consecutive weeks,1 and is characterized by at least 2 of the following symptoms: facial pressure, pain or fullness, headache, nasal obstruction, clear or mucopurulent nasal discharge, and anosmia or hyposmia.2 The prevalence of CRS in Saudi Arabia is 25.3%, and its increase has been recorded in the past few years, particularly in the Eastern Province.4 Chronic rhinosinusitis is classified into 2 categories depending on the presence or absence of nasal polyps and a clinical assessment can be employed to distinguish these two categories: CRS with nasal polyps and CRS without nasal polyps.5 There are several other subtypes, such as dental sinusitis, fungal sinusitis, and pediatric CRS.4 It is evident that CRS is associated with impaired quality of life, decreasing work productivity, and costly medical treatments.6 The pathophysiology of CRS has drawn a lot of attention, leading to an increasing number of studies investigating the risk factors associated with CRS.7-9There are two studies of the Korea National Health and Nutrition Examination Survey that identified several risk factors, such as septal deviation, allergic rhinitis, and influenza vaccination. Moreover, there was an increase in the prevalence of CRS in machinery and plant workers, and with occupational exposure to several factors such as dust, gases, and fumes.10 When patients with occupational rhinosinusitis expose continuously to the causal agents, their conditions may worsen leading to asthma; accordingly, it is important to study the etiology of CRS, specially occupational rhinosinusitis.11 Lastly, the relationship between exposure to occupational risk factors and the development of CRS still remains unclear.12 Thus, this systematic review study is designed to build on previously published studies by expanding the number of studies to find the association between environmental and occupational exposures and CRS development. The findings of these studies may raise the awareness and enhance knowledge concerning the environmental and occupational risk factors in patients with CRS, and these factors may be taken into account when evaluating them to prevent further exacerbations. Moreover, this may also help in planning occupational safety. Additionally, these results may also facilitate a better understanding of the epidemiology of CRS and provide valuable information for its prevention.
Methods
A systematic literature review was carried out to find all published cases of CRS, using the Preferred Reporting Items of Systematic Reviews guidelines by searching PubMed database and Google Scholar. Examination of the studies was carried out by 6 investigators (F.M.K., R.R.M., B.A.A., D.M.A., A.G.M., and F.H.B.) in a specific manner to prioritize determination, and to compare the significant articles. The search was carried out in June 2021 with the following terms: “chronic rhinosinusitis” and “occupation,” “sinusitis” and “environmental factors.” Details of the included and excluded articles are provided in Figure 1.
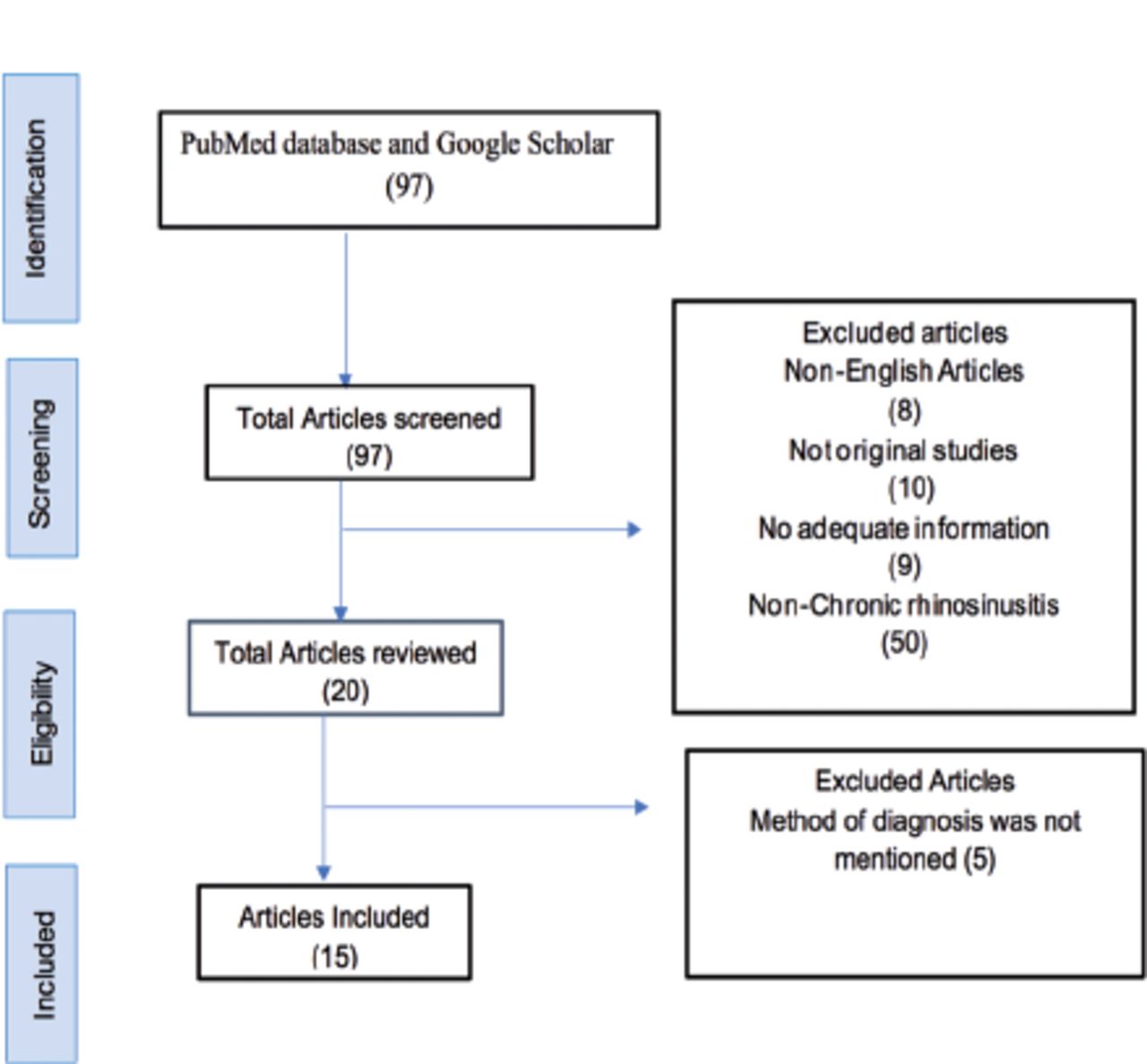
- The PRIMSA diagram details our selection process applied during the overview.
We included all published articles between 1989 and 2021 that reported CRS and occupation, including the following data: age, gender, number of participants with and without CRS, type of environmental and occupational exposure, method of CRS diagnosis, symptoms of CRS, and type of intervention. The articles that reported allergic rhinitis or upper airway diseases were excluded. Non-English articles were excluded from this study.
Results
We reviewed 15 research papers after excluding 82 articles that did not meet our inclusion criteria. A total of 17476 patients were diagnosed with CRS. Most studies linked CRS development to smoke exposure (n=9734), followed by living in rural areas as farms (n=5504). Exposure to pesticide (n=4248) contributed to a higher prevalence of CRS. Blue-collar occupations, such as firefighters (n=2353), farmers, and fishermen (n=1184) were significantly related to the development of CRS in a total of 5260 patients in comparison to 1176 patients with CRS with white-collar occupations, such as sales and service workers (n=320) and managers (n=136). Details of the environmental and occupational factors and the method of diagnosis are provided in Table 1. CRS predominantly affected more men (n=8912) than women (n=8076). The average age of CRS diagnosis was around 40 years; 14 years was the minimum age of CRS diagnosis and 101 years was the maximum age.
- Characteristics of the included studies in terms of number of patients,method of diagnosis and exposure to environmental and occupational factors.
Discussion
We carried out a systematic review study of the association between CRS and occupational and environmental factors that can lead to CRS whichis a prevalent disease considered as inflammation of the upper airway in the paranasal sinus mucosa that lasts for several weeks.1 CRS is characterized by symptoms including nasal obstruction / blockage/ congestion or nasal discharge (anterior/posterior nasal drip or purulent throat mucus), facial pain/pressure, and anosmia/hyposmia, which last at least 3 months.1,2 There were higher rates of hyposmia (16% versus 5%, p=0.003), facial pressure (38% vs. 24%, p=0.008), and sneezing (62% vs. 38%, p<0.001), headache (38% vs. 22%, p=0.003) and nasal pruritus (61% vs. 37%, p<0.001) as mentioned by Veloso-Teles.17 CRS is classified into 2 categories based on the presence or absence of nasal polyps. The prevalence of CRS ranges between 6% and 27.1%; the prevalence of CRS in the United States is 12% and in Europe is 10.9%. However, the prevalence of CRS in Saudi Arabia is 25.3%. There was a significant increase in the prevalence of CRS in machinery and plant operators. It is evident that CRS is associated with impaired quality of life, declining productivity at work, and unaffordable medical treatments. Furthermore, it has a negative effect on patients’ health by causing sleep disturbances, depression, sexual dysfunction, and anxiety. Different diagnostic methods of CRS were used in the articles included in our systematic review; 8 of those articles used the European Position Paper on Rhinosinusitis and Nasal Polyps as the method of diagnosis by fulfilling the European Position Paper on Rhinosinusitis and Nasal Polyps adult criteria in a questionnaire. While 2 articles used the methods of diagnosis based on a questionnaire, which was based on previously diagnosed cases of CRS, 2 other articles utilized subjective and objective assessment for the diagnosis of CRS. While one article adopted subjective and objective assessment for diagnosis of CRS based on the International Consensus Statement on Allergy and Rhinology, another article utilized a survey including 20 questions to investigate the sociodemographic and risk factors of chronic sinusitis as the diagnostic method, and finally one article used a questionnaire based on sinusitis symptoms.
In this study, we found that environmental factors play a significant pathogenic role in the development of CRS. Our data showed that smoking (n=9734, 10%) was positively associated with CRS. There is a 44% higher risk for CRS development among smokers in comparison to non-smokers as illustrated by Clarhed et al.20 According to Chen et al,24 CRS is more prevalent in current smokers (n=1000, 12%) than former smokers (n=1057, 10%). On the contrary, Chen et al24 confirmed that active female smokers (n=654, 7.6%) were at a greater risk for CRS than active male smokers (n=347, 4.2%). Hur et al25 found a statistically significant relation between passive smoking and CRS; however, Wentzel et al26 found equal passive smoke exposure between CRS and control group. Therefore, Christensen et al27 concluded that there is no clear evidence supporting the association between secondhand smoke exposure and CRS. Residents of urban (n=4234, 4%) areas were at a lower risk for CRS. According to Kajiwara-Morita, farmers were more likely to develop CRS compared to non-farmers. This finding is supported by the heavy use of fungicide, pesticides, and insecticide (n=4248, 4%) in their residential areas.18 Similarly, Yu et al28 found that Asian sand dust (ASD), carried through wind from the Mongolian deserts, is associated with the development of CRS and other respiratory diseases. Yeo et al29 described the mechanism by which ASD leads to CRS as ASD increases the replication of rhinovirus leading to disturbance in the local immunological environment, rendering the nasal mucosa more susceptible to dust and microbes. However, Min et al30 and Hoffmans et al31 found no relation between the place of residence and prevalence of CRS. Sundaresan et al32 reported that because of the lack of precision of most studies regarding occupational exposure, no accurate conclusion can be deduced. However, Velazquez et al21 found a linear relationship between occupational exposure to gases vapor, dust, fibers, fumes, and mists (n=150, 1%) and the need for corticosteroids and functional endoscopic sinus surgery in patients with CRS (n=63, 0.6%), which is in agreement with our findings. Moreover, we found that individuals with blue-collar occupations (n=5260, 5.4%) have a greater potential to acquire CRS than those with white-collar occupations (n=1176, 1.22%), which is consistent with Thilsing et al16 findings. Koh et al15 reported that plant and machine operators and assemblers (n=75, 0.077%), craft workers (n=87, 0.09%), and elementary occupations (n=110, 0.11%) were at a greater risk to develop CRS based on data acquired from the Korea National Health and Nutrition Examination Surveys. In contrast, we found that firefighters (n=2353, 2.4%) were at the greatest risk for CRS, which is supported by Webber et al33 based on a cumulative analysis of studies conducted on various countries. In addition, farmers and fishermen (n=1184, 1%) directly follow firefighters, as supported by Siracusa et al.34
Study limitations
This study exhibited that we rely on studies that have subjective or objective diagnosis of CRS, also there is no local studies available which will have an impact on relation between CRS and environmental exposures in our community, and lastly it’s preferred to be carried out along with meta-analysis. Future meta-analysis needs to be conducted to provide further evidence regarding these findings. Also, local studies need to be carried out to evaluate this relation in our community.
In conclusion, CRS is a chronic inflammatory disease of the paranasal sinuses, affected by several environmental and occupational factors. We found that smoking was the most aggravating environmental factor followed by exposure to pesticides, which is observed in rural areas. The severity of CRS symptoms tends to increase with direct contact with allergens. Thus, the greatest proportion of patients with CRS is those with blue-collar occupations, including firefighters, farmers, and fishermen.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 24, 2021.
- Accepted December 26, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.