


Abstract
Objectives: To assess the appropriateness of troponin testing in the Emergency Department (ED) at King Saud Medical City, Riyadh, Saudi Arabia.
Methods: This record-based cross-sectional study examined the electronic records of adult patients who underwent a troponin test following admission to hospital’s ED from January to March 2020.
Results: A total of 367 troponin tests were ordered for 233 patients. Majority of these orders were appropriate (55%) while the remaining (45%) were adjudged as inappropriate. Among the inappropriate orders, majority were single (61%) compared to serial ones (39%). Overall, there were 166 inappropriate orders and the estimated direct monthly cost for inappropriate testing was 49,800 Saudi Riyals in the emergency department alone.
Conclusion: Approximately half of the troponin tests ordered in the ED were inappropriate. The overall financial burden of inappropriate testing greatly impacts patient management and resource utilization. These findings emphasize the pressing need for institutional clinical guidelines to guide appropriate use of troponin testing.
Emergency department (ED) is one of the busiest and most stressful departments for the healthcare providers and especially for physicians, as they have the responsibility of ruling in or ruling out potentially life-threatening and serious conditions such as acute coronary syndrome (ACS), myocardial infarction (MI) and aortic dissection or pulmonary embolism (PE).1 Laboratory testing, in addition to clinical judgement, plays a crucial role in emergency decision-making due to its influence on clinical judgement, treatment, and intervention.2
The skeletal and cardiac muscles contain proteins known as troponins. Troponin T (TnT), troponin I (TnI), and troponin C (TnC) are the 3 subunits that make up Troponin. Troponin I and TnT are the most widely used biomarkers for the detection of cardiac necrosis as they are mainly present in the heart. Under normal conditions, troponin is usually undetectable or present in trace amounts in the blood, however, when heart muscles become damaged, troponin is released into the bloodstream.3,4 The levels of troponin elevation are directly proportional to the damage inflicted on the cardiac muscles.4,5
Troponin I and TnT have replaced creatine kinase-MB (CK-MB) as the gold standard for detection of cardiac injury.6 Thus, availability of troponin assay is essential and fundamental for any ED and the ordering practices should be appropriate due to its importance in clinical assessment and patient management.3,4,7 In ED, troponin test can be ordered by the emergency physicians based on hospital policy or following some guidelines, namely, from the American College of Emergency Physicians. In low-risk ACS patients who were suspected of non-ST segment elevation ACS, testing troponin levels at ED presentation and at 3 hours could be beneficial in predicting a low-rate of major adverse cardiac events within a duration of 30 days.8
Laboratory tests are considered appropriate if they are clinically valid, contribute to improvement of patient care in addition to clinical judgment, and are cost effective.2 Inappropriate testing can be defined as “tests which can be avoided without affecting patient care”.5 Inappropriate testing results in additional workup, over diagnosis, unnecessary treatment, risk of patient harm, increased length of stay and consumes the budget unnecessarily.4,7 Over ordering can also lead to physical and psychological burden, as unexpected results from unnecessary testing may lead to further investigations and delay in commencing appropriate treatment which will cause undue stress and anxiety in patients.4
In modern medical practice, there exists a tendency to order multiple laboratory tests as a profile or panel. Many biochemical tests have a reference range of 2 standard deviations from the mean of a healthy population. Therefore, each test performed on a normal person, there is a 5% probability of getting at least one abnormal result (false negative or false positive). So, if a healthy person undergoes 12 tests, there is a 46% probability that at least one of them will be abnormal.4,9
This current study regarding the appropriate use of troponin testing was carried out in Saudi Arabia. This record-based cross-sectional study aimed to assess the appropriateness of troponin testing within the ED of King Saud Medical City (KSMC), Riyadh, Saudi Arabia. Additionally, the study aimed to estimate the direct cost incurred for inappropriate testing.
Methods
A record-based cross-sectional study was carried out at the ED of a tertiary care hospital, KSMC in Riyadh, Saudi Arabia that receives on an average 100,000 patients per year. Adult patients aged 15 years or older who received a cardiac troponin-I (cTnI) test following admission to the hospital’s ED were identified from January 2020 to March 2020. Patient data was obtained from the hospital information system upon reviewing the electronic files for all relevant clinical and laboratory data. Any uncompleted records were excluded. Ethical approval for this study was obtained from the Research and Innovation Center, KSMC (H1R1-09-Jun20-01).
The cTnI assay was carried out using the Dimension RXL-MAX analyzer (Siemens Healthcare Diagnostics). Troponin levels were considered positive at 0.06 ng/ml, as per the specifications mentioned in the user manual of the assay kit (TNI) manufactured by Siemens (RF621, Dimension® EXL™ integrated chemistry system: LOCI® Module, Flex® reagent cartridge. Siemens Healthcare Diagnostics Inc, Newark, DE, USA). A total of 367 orders of troponin test were assessed for appropriateness by looking at the presenting complaints of the patients to see if the clinical reasons for the orders matched the criteria for appropriateness of troponin testing mentioned in the clinical guidelines. As the hospital does not have its own guideline for troponin ordering, we consulted the guidelines for pathology testing in ED provided by the Australasian College for Emergency Medicine along with other similar studies.4,10-13 Troponin testing was advised in patients presenting with cardiorespiratory symptoms, radiating pain and central nervous system symptoms. The clinical reasons for ordering troponin pathology test are mentioned in Table 1. Any other presenting complaint was classified as “others”.
- Clinical reasons for ordering the troponin pathology test.
For analysis, appropriateness of a single troponin order was classified as appropriate and inappropriate. However, for serial order, the results were categorized into appropriate and repeated appropriately, appropriate and repeated inappropriately, and inappropriate and repeated inappropriately. The data was collected in a sheet for variables including age, gender, presenting complaint, final diagnosis and number of repeats for serial order.
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Science, version 25.0 (IBM Corporation, USA). The frequencies and percentages were used to represent all categorical variables. Total cost incurred for inappropriate testing was calculated based on the cost of an individual troponin test in our hospital (300 Saudi Riyals [SAR]) and the total number of inappropriate tests ordered. This will include the direct test cost and will not include the other indirect costs such as additional testing, prolonged length of stay, and unnecessary intervention.
Results
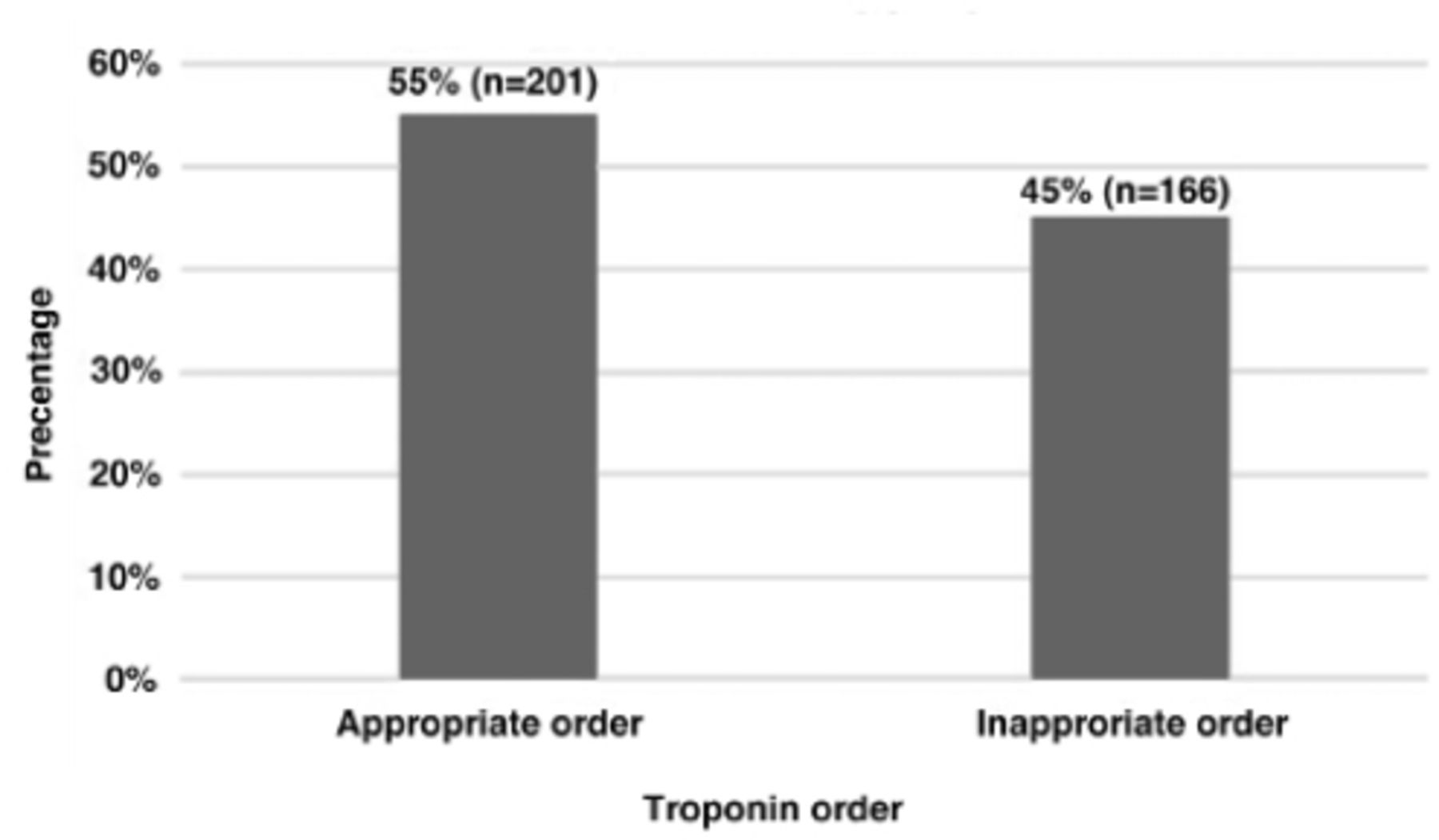
For 233 adult patients, a total of 367 troponin tests were requested for various presenting complaints during the study period. The average age of the patients was 55.1 ± 16.5 years. Overall, 38.7% (n=142) of specimens were from females and 61.3% (n=225) from males. Single troponin orders represent 45% (n=166) and serial troponin orders represent 55% (n=201). From the total troponin orders, 55% (n=201) were found to be appropriate, whereas the remaining 45% (n=166) were judged inappropriate (Figure 1), as per the criteria outlined earlier (Table 1).
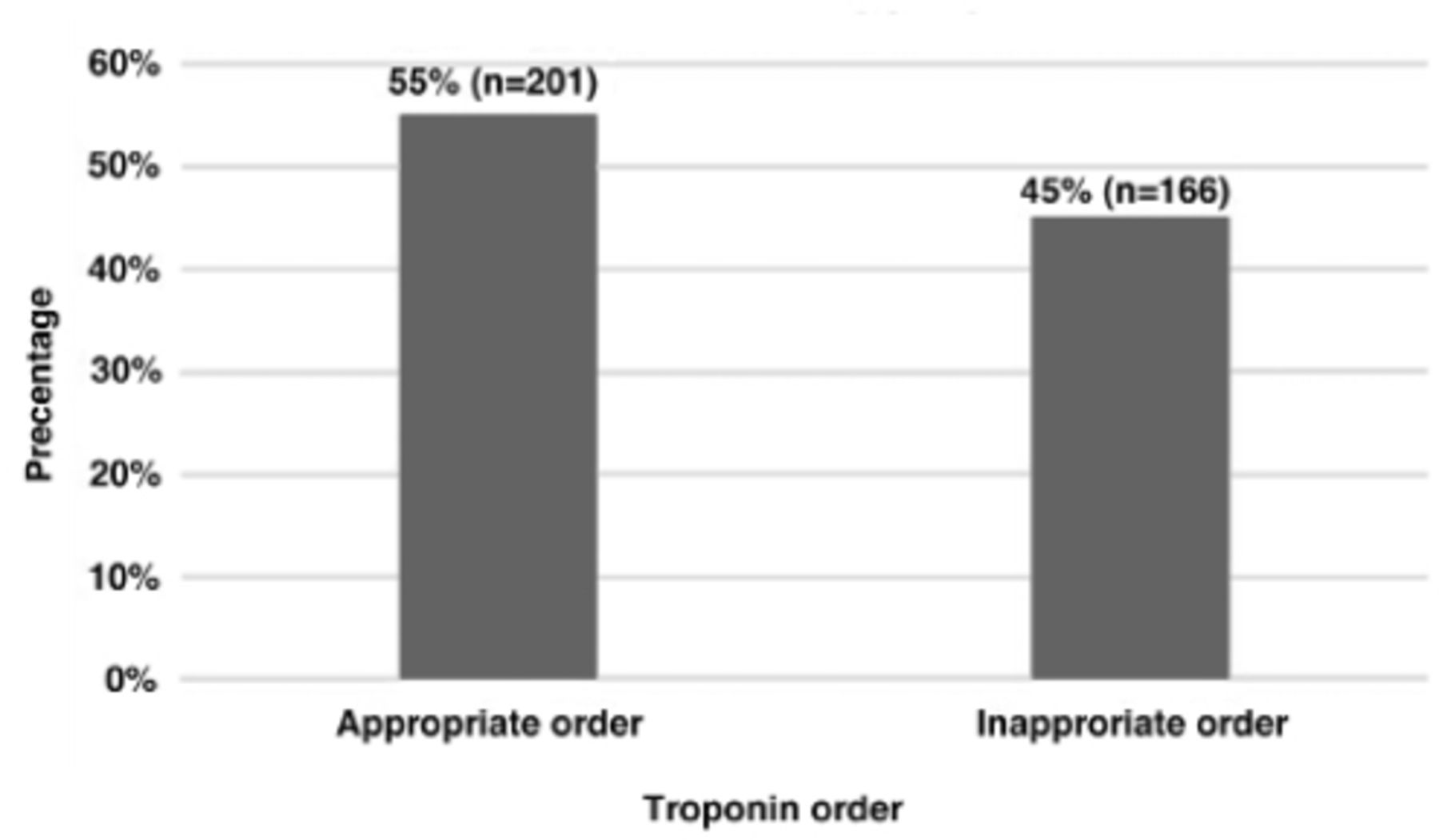
- Representation of appropriateness of total troponin orders.
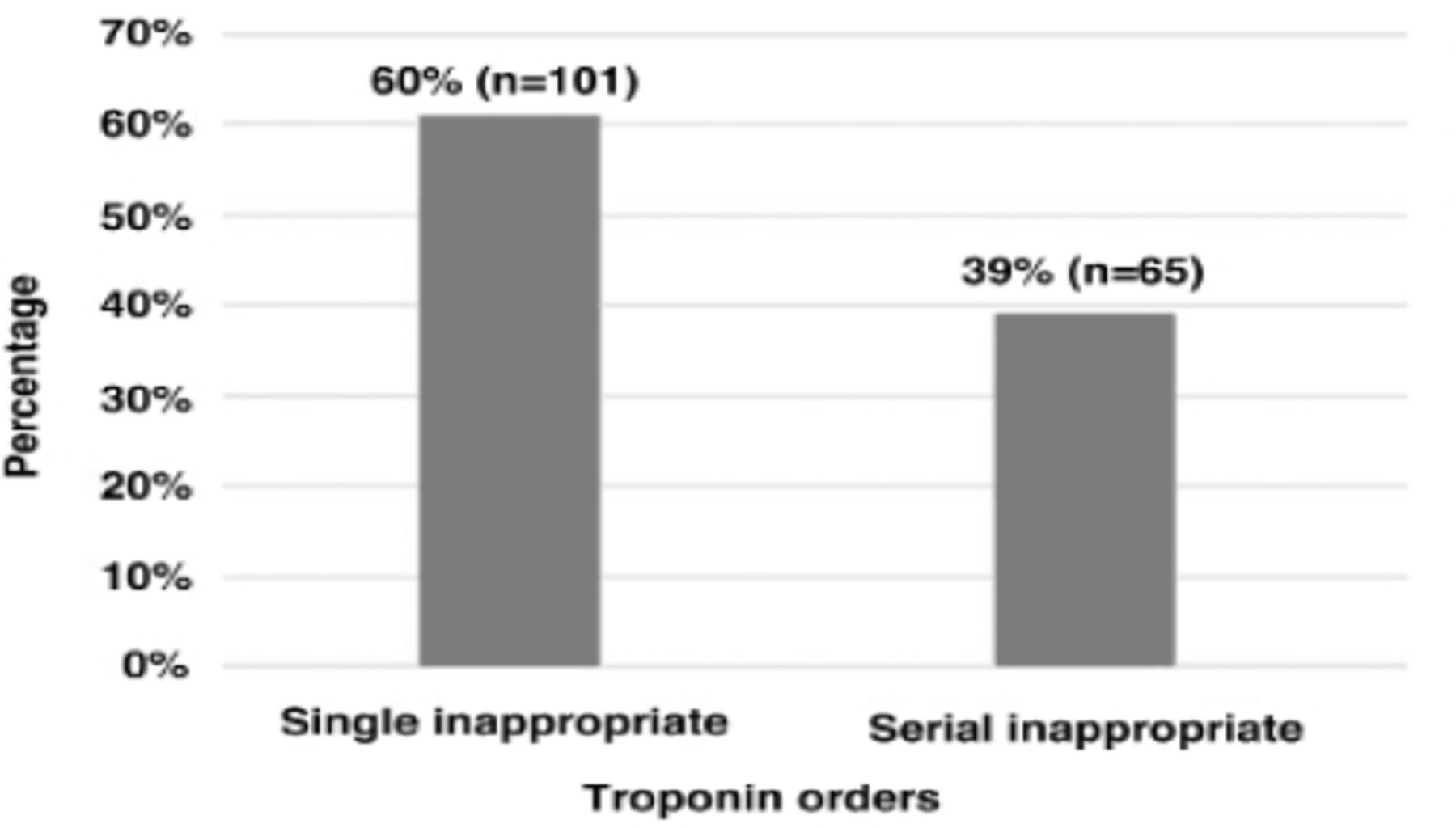
Among the inappropriate troponin orders, majority were single orders (61%, n=101) compared to serial orders (39%, n=65) as shown in Figure 2. Interestingly, 3% (n=5) of those inappropriate orders had tested positive for troponin.

- Distribution of inappropriate troponin orders as single and serial.
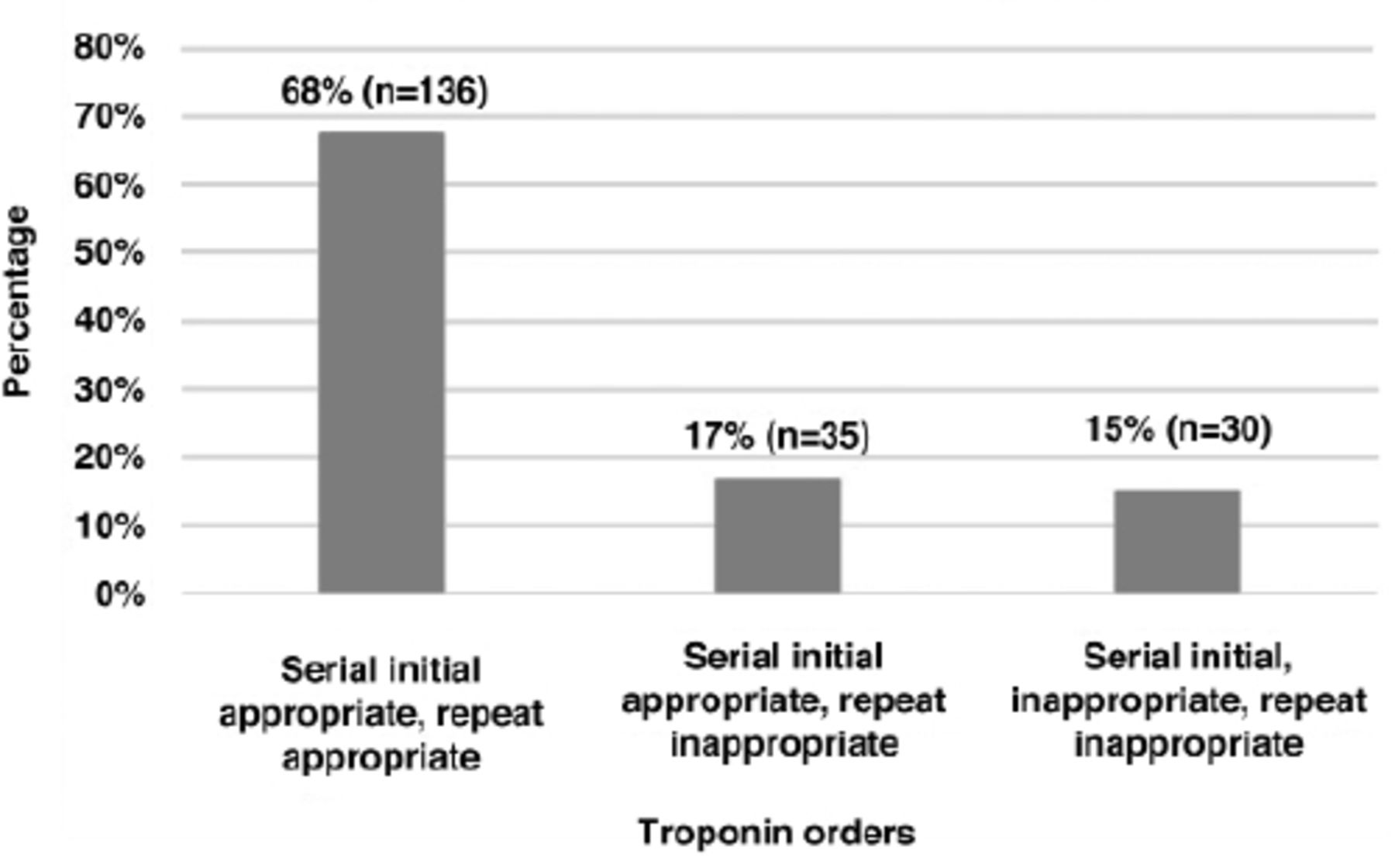
The serial troponin orders were further categorized as shown in Figure 3. Considering the overall number of inappropriate tests (n=166), the estimated direct cost for inappropriate testing was 49,800 SAR in ED of our hospital.
- Appropriateness of serial troponin orders categories.
Discussion
In this study, half of the troponin tests ordered in the ED were inappropriate. This is consistent with the findings of similar studies published from the Western countries. There are several studies, audits and assessments of appropriateness of troponin testing that revealed 23-46% of requested troponin tests to be inappropriate.3,4,12-14 In one such study, Abusalma et al3 found that 41.8% of the Tn I tests were requested inappropriately. The study was followed up after some educational intervention which resulted in the reduction of inappropriate testing of troponin almost by half compared to earlier numbers.3 Furthermore, clinical audits from United Kingdom and Ireland assessing the appropriateness of troponin testing for a period of one and 2 weeks showed that the proportion of inappropriate troponin ordering was 28.1% for a period of one week and 46% for 2 weeks.11 A retrospective study from an Australian teaching hospital showed that 23.4% of troponin tests requested in the ED were deemed inappropriate as they were not in agreement with the clinical guidelines and did not alter the patient management.4
Published report shows that troponin assays are routinely performed in EDs even in the absence of clear clinical suspicion for ACS.4 A study from a large teaching hospital in Oxford where 40% of the troponin tests were ordered inappropriately showed that in addition to patient harm and over utilization of hospital resources, the cost of inappropriate tests amounted to 320£ over a period of just 48 hours.12
In our study, single troponin orders were used more extensively and inappropriately compared to serial orders. This is similar to what has been observed by Davey’s14 audit in 3 Australian hospitals where it was shown that majority of the single troponin orders were used more than the serial orders. In this study, there were 5 orders that were classified as inappropriate based on our pre-determined criteria that turned out to be positive for troponin. Upon analysis of these cases, we found that amongst 5 patients: 2 had bacteremia/sepsis, 2 were diagnosed with end stage renal disease (ESRD), and one had history of meningioma. It has been shown that troponin can be elevated in some non-cardiac conditions as well and there is a significant correlation between ESRD and troponin elevation.5 Similarly, there is a strong association between sepsis and elevated troponin levels as some studies have shown that elevated TnI or TnT can occur in up to 43-85% of patients with sepsis, however, no possible explanation can be attributed to the last case.4,5
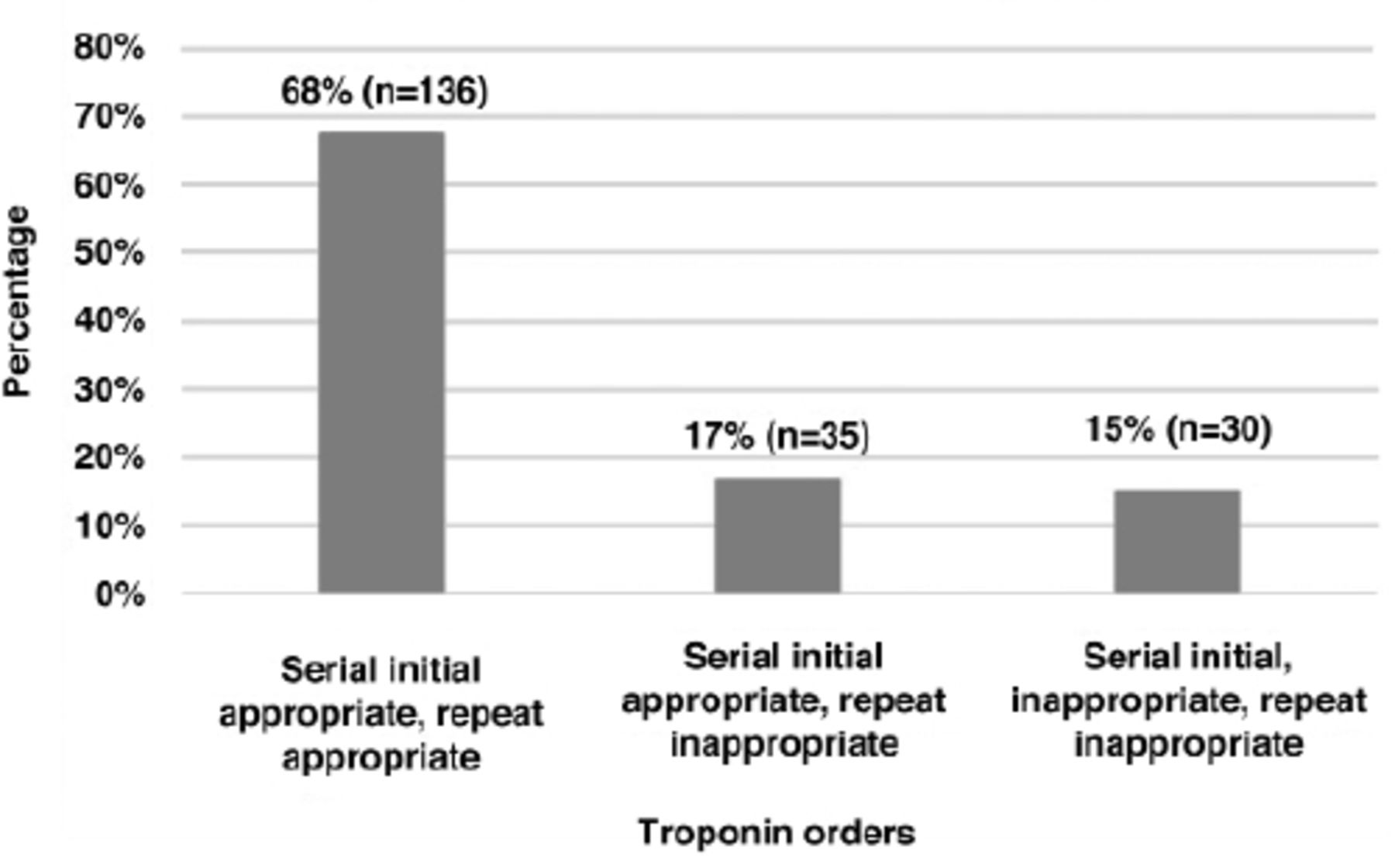
Our study revealed that out of 201 serial troponin orders, the initial test was appropriate in 17% (n=35) of the orders, but the repeated tests were inappropriate and 15% (n=30) of tests were initially ordered as well as repeated unnecessarily without any appropriate indication. Despite the relatively small number of these cases, the overall financial burden is much higher than anticipated because improper patient management may result in additional investigations, a longer length of stay, unnecessary treatment, and, most importantly, additional costs. Therefore, the importance of having an institutional protocol for appropriate test ordering and adherence to the test ordering guidelines cannot be emphasized more.
Reducing inappropriate ordering of troponin tests can generate huge financial benefits.3,4 In our hospital, the cost of a single troponin test is 300 SAR and approximately 4000 troponin tests are ordered monthly from ED. This implies that nearly 1.2 million SAR are spent each month on troponin testing for ED alone. Based on our findings, 45% of these troponin orders could be inappropriate, resulting in a monthly expenditure of more than half a million SAR (0.54 million SAR) on inappropriate troponin orders from the ED. This equates to an estimated 6.48 million SAR that can be potentially saved annually. In fact, this is only a fraction of the total cost that can be saved because it excludes the overall cost, which includes prolonged length of stay, additional testing, delay in patient management, manpower, and time spent on such cases.
Detailed investigative study is required to explore the reasons for ordering inappropriate troponin tests in an acute care setting in the ED. Some of the plausible reasons could be over estimation of MI diagnosis by the physician, absence of a clear protocol for ordering troponin tests, ordering of tests by nurses or junior physicians in the triage area before examination of patients by senior physicians, or reckless ordering of a set of lab tests as a default for patients presenting in the ED (habit of click/tick the box practice).
In conclusion, clinical practices that support ordering of appropriate tests play a critical role in diagnosis, patient care, and proper resource utilization. Many strategies can be formulated to address this issue including creation of institutional protocols and clinical practice guidelines, conducting audits to assess test utilization, multidisciplinary collaborations, and adopting newer concepts in laboratory medicine like establishing diagnostic management teams, and initiating clinical laboratory stewardship programs. These initiatives could yield positive results through effective communication between clinical laboratory staff and physicians ordering the tests, commitment and support from hospital administration together with efficient project management and information technology support. Such firm understanding is crucial for good laboratory practices, improved patient outcomes, and appropriate utilization of healthcare resources.
Acknowledgment
The authors would like to thank the research and innovation center at King Saud Medical City, Riyadh, Kingdom of Saudi Arabia for their continued support. The authors would like to acknowledge Turacoz Healthcare Solutions for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 29, 2021.
- Accepted March 14, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.