


Abstract
Objectives: To review and assess the efficiency of pre-emptive plerixafor administration for poor mobilization (PM) and to review and assess mobilization efficiency (≥2×106 CD34+ cells/kg) in patients who received autologous stem cell transplantation for lymphoma and multiple myeloma (MM) at the Department of Adult Hematology/Blood Marrow Transplant, Princess Noorah Oncology Center, King Abdulaziz Medical City, Jeddah, Saudi Arabia, over the past 7 years.
Methods: This retrospective study evaluated all patients with MM and lymphoma undergoing peripheral blood stem cell mobilization and collection at our institution between February 2014 and August 2021. Plerixafor was administered pre-emptively by a plateau of <10 peripheral blood CD34+/µl after chemotherapy-based mobilization or CD34+ of <8/µL on day 4 after mobilization with G-CSF alone. Between peak CD34+ levels of 10-15/µl, plerixafor will be used at the discretion of the treating physician.
Results: In total, 215 patients were enrolled. Among them, 80% had peak CD34+ level ≥20/µL, 11% had clear poor mobilization (peak CD34+ levels <10/µL), and 9% had borderline PM (CD34+ between 10-19/µL). Plerixafor was administered pre-emptively in 13% of the patients and 75% of patients with borderline PM were collected without plerixafor, suggesting that plerixafor is not needed if CD34+ >15/µL on the anticipated collection day. Mobilization failed in only one patient (<1%).
Conclusion: Our data showed that with plerixafor pre-emptive administration, the primary endpoint was achieved for most patients identified with PM, preventing the need for a second mobilization attempt.
Lymphoma and multiple myeloma (MM) are among the most common hematological malignancies worldwide.1,2 High-dose chemotherapy and autologous stem cell transplantation (ASCT) using mobilized peripheral blood stem cells (PBSCs) are commonly used to treat lymphoma and MM.3,4 Adequate mobilization and collection of PBSCs are important for ASCT outcomes. Over the past decade, different criteria have been proposed to define successful CD34+ cell mobilization, leading to an adequate apheresis yield. The current minimal threshold CD34+ cell dose needed to achieve a fast, complete, and stable long-term engraftment has been determined to be ≥2×106 CD34+ cells/kg for a single ASCT.5,6
Two main strategies are routinely used for PBSC mobilization: I) chemotherapy-based stem cell mobilization, in which the patient receives a cycle of mobilization-specific or disease-specific chemotherapy followed by repeated administration of granulocyte col ony-stimulating factor (G-CSF); or II) G-CSF-based mobilization, where only repeated administration of G-CSF is initiated 5 days before the scheduled first day of apheresis.4,7 Although PBSC mobilization and collection are highly effective in most patients, poor mobilization (PM) has been reported in approximately 15% of patients.7 Risk factors for PM include extensive bone marrow involvement, type of prior chemotherapy agents used, prior irradiation, prior prolonged exposure to lenalidomide, low blood counts before mobilization, presence of baseline thrombocytopenia, an extended interval from diagnosis to mobilization, female gender, and old age.4,5,7,8 Plerixafor (a CXCR4 inhibitor) can be added to both mobilization strategies, and it has been shown to increase CD34+ cell yields and improve mobilization outcomes.9,10 Limitations and challenges to the routine use of plerixafor include the high cost in resource-limited economies and lack of consensus guidelines. In many transplant centers, plerixafor is mostly limited to patients who fail to reach sufficient PB CD34+ levels at maximum stimulation (pre-emptive use).4
The primary objectives of this study include: reviewing and assessing the efficiency of pre-emptive plerixafor administration for PM and reviewing and assessing mobilization efficiency (≥2×106 CD34+ cells/kg) in patients who received ASCT for lymphoma and MM at the Department of Adult Hematology/BMT, Princess Noorah Oncology Center, King Abdulaziz Medical City, Jeddah, Saudi Arabia over the past 7 years.
Methods
This retrospective study analyzed the data of all lymphoma and MM patients who underwent PBSC collection at the Department of Adult Hematology/BMT, Princess Noorah Oncology Center, King Abdulaziz Medical City, Jeddah, Saudi Arabia, between February 2014 and August 2021, this was a record-based data analysis The Institutional Review Board of our institution approved the protocol for data collection and analysis. Clinical and disease-related parameters, such as gender, age at diagnosis, age at PBSC collection, disease status before mobilization, mobilization regimens, body weight (BW), complete blood counts before PBSC collection, parameters of plerixafor administration, and PBSC collection (peak peripheral blood [PB] CD34+ cells/µL at maximum stimulation, absolute PB CD34+ cell/µL at day 1 of leukapheresis [LP], number of LP sessions, total blood volume processed [TBV], and collected CD34+ cells/kg BW) were collected and extracted from the patient medical records and files. Data were evaluated for the overall cohort, disease entity (lymphoma or MM), peak PB CD34+ cell count on the scheduled first day of apheresis (<10/µL, between 10-19/µL or ≥20/µL), and the need for pre-emptive plerixafor.
Mobilization regimens
As stated earlier, there are 2 main strategies to mobilize stem cells in autologous patients: chemotherapy followed by G-CSF or G-CSF alone. For the first method, the following were the most commonly used chemotherapy regimens based on disease entities: cyclophosphamide, (R-)ESHAP (rituximab, etoposide, methylprednisolone, cytarabine, and cisplatin), (R-)IGEV (rituximab, ifosfamide, gemcitabine, and vinorelbine), GDP (gemcitabine, dexamethasone, and cisplatin), R-ICE (rituximab, etoposide, ifosfamide, and carboplatin), cytarabine plus etoposide, (R-)CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), and (R-) DHAP (rituximab, dexamethasone, cisplatin, and cytarabine). Daily G-CSF was administered subcutaneously at a dose of 5-10 µg/kg BW starting from the day after the end of chemotherapy to the end of PBSC collection. Daily complete blood count monitoring was started from day 6 of G-CSF administration, and daily monitoring of PB CD34+ cell count started when leukocytes were ≥1×109/L. For mobilization with G-CSF alone, G-CSF (10 µg/kg BW) was administered subcutaneously in 2 divided doses starting 5 days before the scheduled day 1 of leukapheresis. Here, the daily complete blood count and PB CD34+ cell count were determined on day 4 in order to place a central venous catheter (CVC insertion) and perform LP on day 5.
In case of PM, pre-emptive plerixafor was administered. The pre-emptive use of plerixafor was triggered by a plateau of <10 PB CD34+ cells/µL under continued G-CSF administration (namely, total white blood cell [WBC] count ≥1×109/L, and no increase in PB CD34+ cell count compared to the previous day) after chemotherapy-based mobilization or a PB CD34+ cell count of <8/µL on day 4 after mobilization with G-CSF alone. When PB CD34+ cell count was between 10-15/µL at the peak stimulation, plerixafor was used at the discretion of the treating physician considering the collection goal. Plerixafor (240 µg/kg) was administered subcutaneously 9-12 hours before the LP session.
CD34+ cell enumeration and PBSC collection
When the PB WBC count was ≥1×109/L, the PB CD34+ cell count was determined with a single-platform method by flow cytometry using the BD FACSCanto II system and BD stem cell enumeration kit (Beckton, Dickinson and Company, USA). In patients mobilized with G-CSF alone, LP was started on day 5 if a PB CD34+ cell level was of ≥8/µL on day 4 and in patients mobilized with chemotherapy + G-CSF LP was started if PB CD34+ cell level was of ≥10/µL at peak stimulation. In the case of PM, pre-emptive plerixafor was initiated, as mentioned above. For the initiation of autologous PBSC collection, a hemoglobin level of ≥8.0 gm/dl and a platelet level of ≥40x109/L were mandatory; packed red blood cells or platelets were transfused immediately before or after LP if needed.
Peripheral blood stem cells were collected via central venous catheters or PB using a Spectra Optia® apheresis system and mononuclear cell collection (MNC collection) tubing system according to the manufacturer’s instructions (Terumo BCT). The maximum processed TBV was 4 times the patient’s blood volume. The collection time was restricted to a maximum of 5-6 hours per LP session. The anticoagulant Anticoagulant Citrate Dextrose Ph Eur Solution A (Terumo BCT, Inc.) was used at an inlet: AC ratio of 12-15:1 for 35-70 ml/minutes of inlet flow rate. Continuous calcium gluconate infusion (10%; 2000 mg diluted in 250 ml 0.9% normal saline, initiated at 500 mg/hour) was used to prevent citrate toxicity due to citrate anticoagulation. Daily LP sessions were continued until the collection goal was achieved, or additional LP sessions were considered unpromising due to low PB CD34+ cell counts or low quantities of CD34+ cells collected. The minimum quantity of CD34+ cells collected for a single ASCT was ≥2×106 CD34+ cells/kg BW. High-risk MM patients or young and potential candidates for a second transplant were assigned into the collection for double ASCT group, while other patients were assigned to the collection for single ASCT group.
Statistical analysis
Data management and analyses were carried out using the Statistical Package for the Social Sciences, version 23.0 (IBM Corp., Armonk, NY, USA). Descriptive statistical analyses were carried out on the study sample. Values were reported as proportions and percentages for categorical variables and as means and standard deviations or modes with ranges for continuous variables.
Results
A total of 215 (lymphoma: 149, MM: 66) patients were enrolled in this study (144 men and 71 women). The median age at the time of collection was 40 years (range: 14-69). The characteristics of the enrolled patients are as follows: 86 (40%) Hodgkin’s lymphoma patients, 63 (29%) non-Hodgkin’s lymphoma patients, and 66 (31%) MM patients. The subgroup of patients with non-Hodgkin’s lymphoma was heterogeneous, and diffuse large B-cell lymphoma (60%, 38/63), anaplastic large cell lymphoma (13%, 8/63), T-cell lymphoma (8%, 5/63), Burkitt’s lymphoma (5%, 3/63), and Mantle cell lymphoma (5%, 3/63) were the most frequent entities. The patient characteristics are detailed in Table 1.
- Patient characteristics.
Chemotherapy mobilization was carried out in 71% (153/215) of patients, while mobilization with G-CSF alone was carried out in 29% (62/215) of patients. Pre-emptive plerixafor was administered to 13% (29/215), 76% (22/29) of whom were lymphoma patients and 24% (7/29) were myeloma patients. The records show that 23 patients received one dose of plerixafor, one patient received 2 doses of plerixafor, and one patient received 3 doses of plerixafor, at the first pre-emptive attempt of plerixafor. Furthermore, one patient received 2 doses and 3 patients received 3 doses of plerixafor in the first and second pre-emptive attempts.
The median PB CD34+ cell count at maximum stimulation was 61 (range: 0-1367/µL) among all patients. Multiple myeloma patients had relatively higher PB CD34+ levels at maximum stimulation (median: 76/µL, range: [3-304/µL]) than lymphoma patients (median: 50/µL, range: [0-1367/µL]).
Approximately 80% of all patients (78% of HL patients, 75% of NHL patients, and 86% of MM patients) reached PB CD34+ count of ≥20/µL at peak stimulation. Clear PM (peak PB CD34+ count <10/µL) was recorded in 11% (24/215, 9% lymphoma, and 2% MM) of patients and borderline PM (PB CD34+ count between 10-19/µL at the peak of stimulation) was recorded in 9% (20/215, 7% lymphoma and 2% MM) of patients.
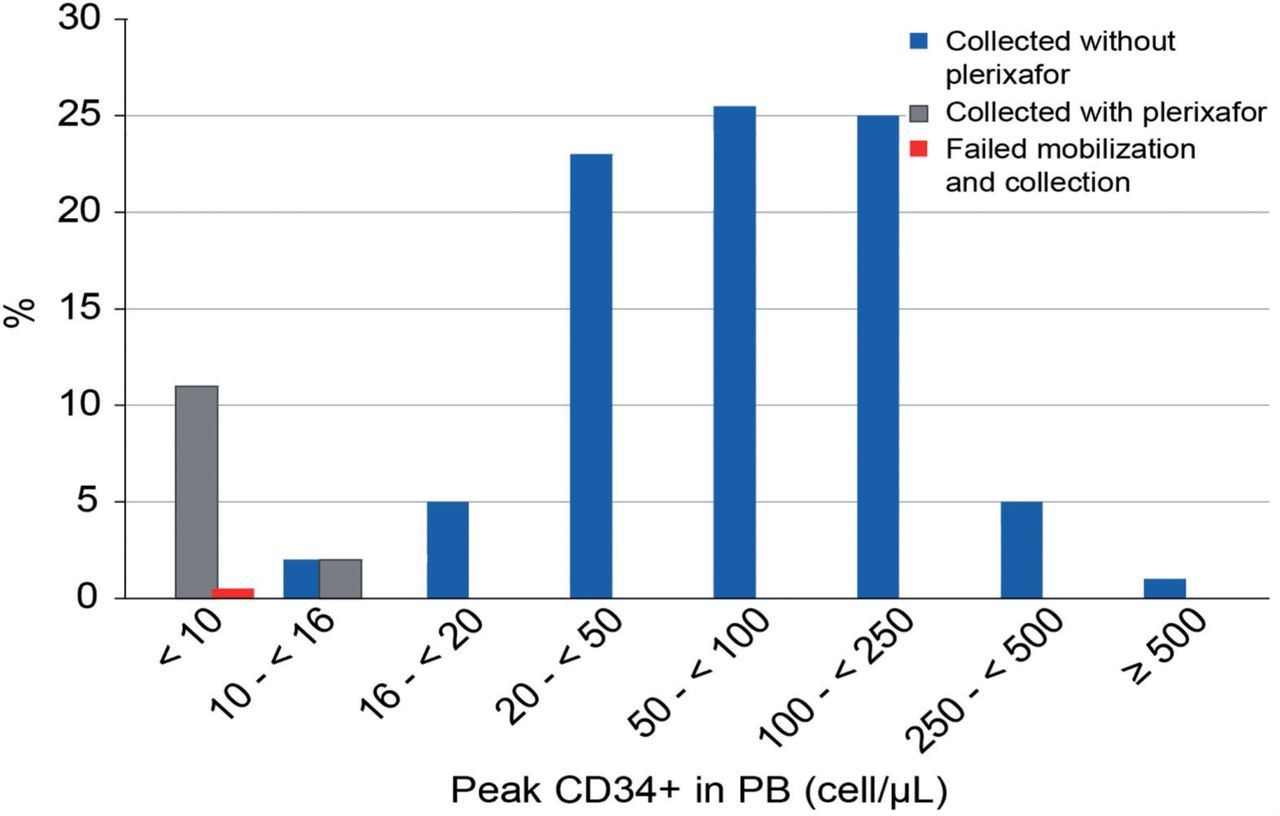
Pre-emptive plerixafor was administered to 13% (29/215) of the patients; this included all patients who had peak PB CD34+ count of <10/µL (24/29) and 5 (5/29) patients who had a CD34+ count between 10-15/µL at peak stimulation. Peripheral blood stem cells were collected in 75% (15/20) of patients with borderline PM without pre-emptive plerixafor; 5/20 patients had a PB CD34+ count between 10-15/µL at maximum stimulation and 10/20 patients had a PB CD34+ count between 16-19/µL at maximum stimulation.
Pre-emptive plerixafor administration failed in 5 (17%) of 29 patients at the first attempt, leading to insufficient mobilization and collection of CD34+ cells. Three (3/5) of them underwent successful PBSC collection after additional plerixafor attempts, and one (1/5) with insufficient mobilization following initial stimulation with G-CSF+ plerixafor underwent successful PBSC collection after mobilization with chemotherapy. One patient had inadequate CD34+ cell mobilization (<10/µL; Figure 1).

- peripheral blood stem cell mobilization and collection (± preemtive plerixafor).
The median value of the circulating CD34+ cells/µL before plerixafor administration was 5 (range: [0-15]). After the first dose of plerixafor, the median number of circulating CD34+ cells/µL was 36 (range: [3-199]). The first dose of plerixafor was associated with a median 7.2-fold increase in PB CD34+ levels among all entities (from a median of 5/µL to 36/µL). We did not observe statistical differences between MM and lymphoma patients in terms of CD34+ increase. The median value of the circulating CD34+ cells/µL at first day of LP was 63 (range: [9-1367]) in all patients.
The overall median CD34+ cell collection result in the entire patient population was 5.1×106 (range: [2.03-66.2]×106 cells/kg BW), with the highest median number of 6.6×106 cells/kg BW in MM patients, in whom the collection goal was 2 ASCT. The minimum 2×106 CD34+ cells/kg BW (representing one transplant) was achieved in 214 (>99%) patients: 100% in MM patients and 99% in lymphoma patients. Mobilization failure at this threshold occurred in one patient (<1%).
The mean of overall processed TBV was 2.2±0.62 among all entities. The median number of LP sessions carried out was 1 (range: [1-2]), with cells successfully collected in 83% of patients following just one LP session. Mobilization regimens, blood counts before collection, and mobilization and collection results are summarized in Table 2.
- Parameters and results of peripheral blood stem cells mobilization and collection.
Discussion
Peripheral blood stem cell mobilization and collection failure or use of suboptimal stem cell doses can have major adverse effects on patient outcomes and increase the cost and risk of re-mobilization. Plerixafor has been shown to improve CD34+ cell yield and mobilization outcomes. Limitations and challenges to the routine use of plerixafor include the lack of consensus guidelines and its high cost, especially in resource-limited settings. This study is a real-world experience data from the Middle East region elaborating on stem cell mobilization and the pre-emptive plerixafor approach for lymphoma and MM patients undergoing autologous PBSC transplantation.
Overall, ≥2×106 CD34+ cells/kg BW were collected in 98% (210/215) of patients at the first mobilization attempt with or without plerixafor. A total of 83% (24/29) with PM who received pre-emptive plerixafor achieved the primary endpoint and did not require further mobilization sessions. In the present study, the mobilization and collection failure rate (29/215; 13%) was reduced to 2% (5/215) at the first mobilization attempt, rendering the collection of at least a single transplant with a single mobilization attempt (a realistic goal in all patients undergoing PBSC mobilization).
Clear PM (peak PB CD34+ count <10/µL) decreased from 11% to <1% with pre-emptive plerixafor administration after chemotherapy or G-CSF mobilization in the present study. Similarly, the collection failure rate at a threshold of 2×106 CD34+ cells/kg BW was reduced to <1% with pre-emptive plerixafor.
Data from a prospective trial by Milone e al11 showed that the use of plerixafor as pre-emptive or rescue post-chemotherapy mobilization decreases the rate of PM (peak CD34+ cell levels in PB of <20/µL) to 3% versus 13% in a historical control group mobilized without plerixafor. In addition, the rate of collection failure at a threshold of 2×106 CD34+ cells/kg BW decreased from 21% to 4% with pre-emptive/rescue plerixafor.
Attolico et al6 reported successful collections after mobilization with chemotherapy followed by G-CSF plus plerixafor in 73% of patients: 65% of lymphoma patients and 82% of MM patients. In our study, mobilization with chemotherapy followed by G-CSF plus plerixafor in the patients with PM allowed for successful stem cell collection in 81% of patients: 75% of lymphoma patients and 100% of MM patients.
In this study, adequate PBSC collection (≥2x106 CD34+ cells/kg BW) was recorded in 84% (181/215) of all patients who achieved a PB CD34+ cell level of >15/µL at maximum stimulation on the first day of apheresis. The number of PB CD34+ cells strongly correlated with the collected CD34+ cells/kg in our study, allowing the establishment of a CD34+ cells level threshold of >15/µL in PB as predictive of achieving ≥2x106 CD34+ cells/kg BW.
According to our study, poor mobilizers were those lymphoma or MM patients whose CD34+ cell counts in PB were <8/µL on the fourth day of G-CSF mobilization and <10/µL at the peak of stimulation. A CD34+ cell count of >15/µL in PB on the scheduled day of apheresis can be used as a threshold to differentiate between the poor and the good mobilizers.
Sancho et al8 proposed that a threshold of 13.8 CD34+ cells/µL in PB was enough to ensure adequate PBSC collection (>2x 106 CD34+ cells/kg), with a high sensitivity and specificity in both lymphoma and MM patients. Overall, 255 (64%) of the patients achieved a PB CD34+ cell count of 13.8/µL before their initial apheresis.
Several groups have developed algorithms to guide the use of plerixafor.7,8 Costa et al12 developed and validated a decision-making algorithm based on the PB CD34+ cell count on day 4 of G-CSF administration and a CD34+ cells collection target to guide the cost-effective use of plerixafor. Micallef et al9 explored the use of plerixafor in patients with PB CD34+ cell count of <10 on day 4 of G-CSF or day 1 yield <1.5x106 CD34+/kg BW. In another retrospective analysis of 1556 patients with lymphoproliferative disorders initially mobilized with G-CSF alone, sensitivity-specificity analysis was used to identify ideal PB CD34+ count cutoff points that would allow early intervention and prevent collection failure.7,13 This study recommended considering plerixafor for patients who fail to reach a PB CD34+ count of 6/µL on day 4 or 10/µL on day 5 after starting G-CSF.13
Horwitz et al14 reported that the administration of plerixafor can be delayed to day 5 of G-CSF until after the peak mobilization response to G-CSF has been completely assessed. Patients were eligible for plerixafor if they had less than 7 circulating CD34+ cells/µL on day 5 of G-CSF or if <1.3×106 CD34+ cells/kg were collected on the first day of apheresis.
A group of experts suggested to estimate the patient’s risk of PM and to consider additional interventions.7 Peripheral blood CD34+ cell counts before apheresis is the most robust predictor for patients at risk of PM. For patients with >20 CD34+ cells/µL in PB before apheresis, no pro-active intervention is needed, whereas the pre-emptive use of plerixafor is recommended to reach a minimum cell target of 2×106 CD34+ cells per kg BW in patients with <10 CD34+ cells/µL in PB before apheresis. For patients with 10-20 CD34+ cells/µL at the mobilization peak before apheresis (namely, gray zone), a dynamic approach is suggested.
Wuchter et al5 defined patients with MM or NHL with <20 CD34+ cells/µL as poor mobilizers, despite patients with a peak level of CD34+ cells between 11-19/µL (considered as borderline poor mobilizers) achieving ≥2×106 CD34+ cells/kg BW, and 86% of those with CD34+ cells in PB between 6-10/µL also obtaining a target dose of ≥2x106 CD34+ cells/kg. Similar results were reported by Pusic et al,15 who described a peak level of CD34+ cells >20/µL to achieve >2x106 CD34+ cells/kg BW in a single day collection. Sinha et al13 also reported that patients with MM and a CD34+ cell count of 11/µL in PB achieved 2×106 CD34+ cells/kg BW.
These slight differences in the cutoff value of PB CD34+ cell count are attributable to differences in the definition of PM, as well as differences in the PBSC collection procedure (type of apheresis system, number of TBVs processed, timing to start daily monitoring of PB CD34+ cell count with chemotherapy mobilization). A definitive PB CD34+ cells cutoff value is useful as a successful predictive parameter for the pre-emptive administration of plerixafor.
Study limitations
Its retrospective design, inability to generalize the findings to different populations, and the small sample size of patients who received pre-emptive plerixafor on subjective decisions were the limitations of this study. However, we believe that the impact of these factors is minimal on the results of the study. We believe that the uniformity in the CD34+ cell count enumeration and apheresis system provides additional value.
Our data suggest that plerixafor is not needed if PB CD34+ level is>15/µL on the predicted day of LP. We recommend pre-emptive plerixafor if PB CD34+ level is <10/µL at maximum stimulation after chemo-mobilization and <8/µL on day 4 of G-CSF mobilization. For levels between 10-15 CD34+ cells/µL at maximum stimulation, a dynamic approach with case-by-case decision-making is recommended.
In conclusion, mobilization of PBSCs with mobilization regimens (chemo-mobilization or G-CSF mobilization) incorporating pre-emptive plerixafor for PM in patients with lymphoma or MM was efficient. It allowed for the collection of a minimum of 2×106 CD34+ cells/kg BW required for a single ASCT in nearly all patients (>99%).
Acknowledgment
The author gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 29, 2021.
- Accepted April 25, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.