


Article Figures & Data
Figures
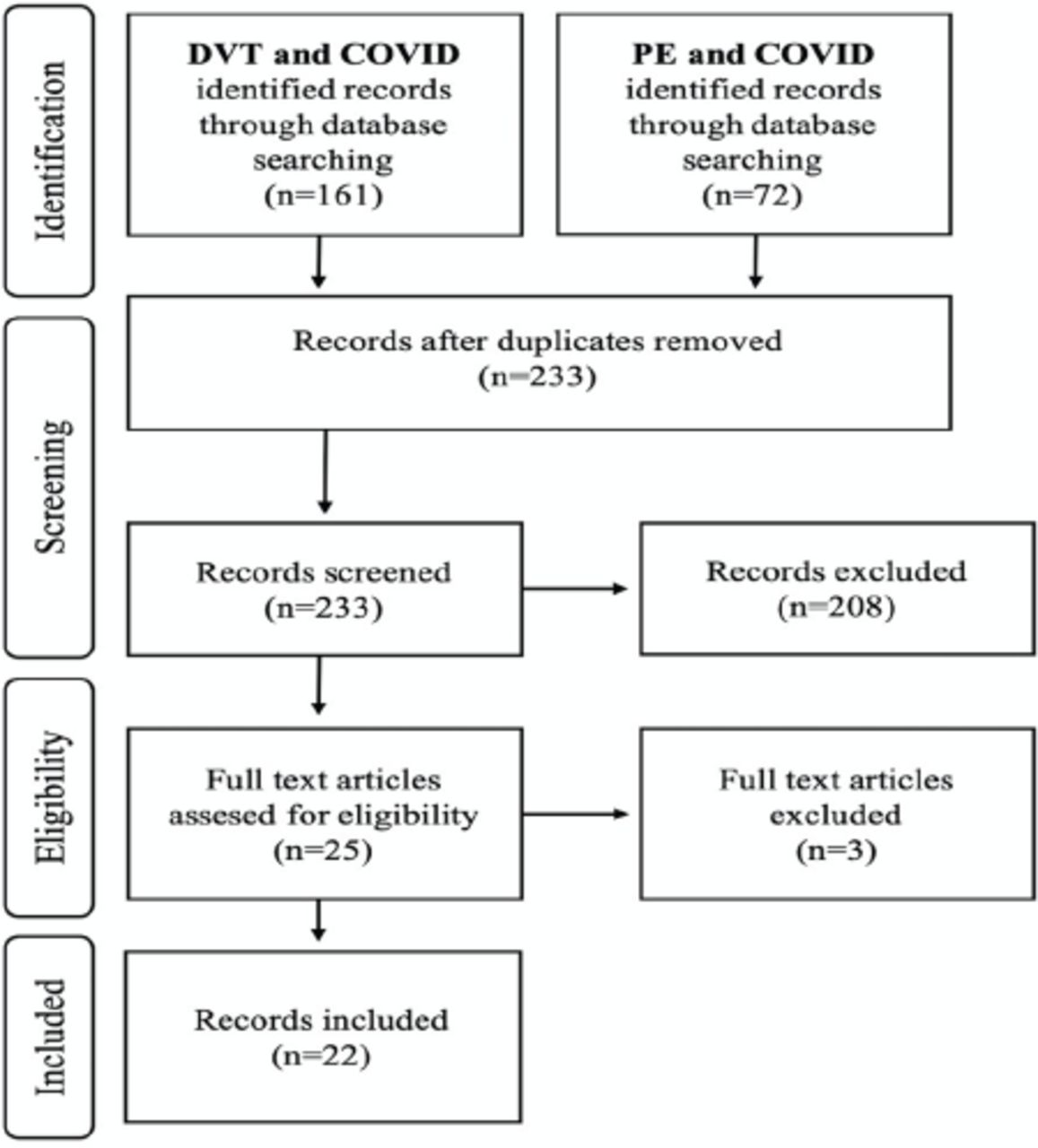
- Figure 1
- Flow chart of study selection.
Tables
- Table 1
- Characteristics of published cases of coronavirus associated venous thromboembolism (N=48).
Variable Valid= (n/48) n (%) Confirmed PE (n=38) Confirmed DVT (n=10) P-value Age (years)** 48 56±17.17 56±16.90 58.00±19.07 0.796 Male 48 34 (70.8) 26 (68.4) 8 (80.0) 0.745 Presenting symptoms of COVID-19 45 Fever 29 (60.4) 24 (63.2) 5 (50.0) 0.694 Chills 3 (6.2) 2 (5.3) 1 (10.0) 1.000 Cough 29 (60.4) 26 (68.4) 3 (30.0) 0.065 SOB, dyspnoea 24 (50.0) 22 (57.9) 2 (20.0) 0.076 Fatigue, malaise 9 (18.8) 7 (18.4) 2 (20.0) 1.000 Myalgia 9 (18.8) 6 (15.8) 3 (30.0) 0.569 Headache 6 (12.5) 5 (13.2) 1 (10.0) 1.000 New loss of taste or smell (anosmia) 1 (2.1) 1 (2.6) 0 (0.0) 1.000 Nausea or vomiting 2 (4.2) 2 (5.3) 0 (0.0) 1.000 Diarrhea 6 (12.5) 5 (13.2) 1 (10.0) 1.000 Chest pain (pleuritic pain) 5 (10.4) 4 (10.5) 1 (10.0) 1.000 Presenting symptoms/signs of PE 38 Chest pain 9 (18.8) 8 (21.1) 1 (10.0) 0.733 Tachycardia 2 (4.2) 1 (2.6) 1 (10.0) 0.882 Shortness of breath (dyspnea) 30 (62.5) 27 (71.1) 3 (30.0) 0.044 Hypoxia (O2 saturation <90%) 9 (18.8) 9 (23.7) 0 (0.0) 0.211 Presenting symptoms of DVT 9 Unilateral erythematous swelling of the lower extremity 4 (8.3) 1 (2.6) 3 (30.0) 0.032 Leg pain or tenderness of the thigh or calf 3 (6.2) 0 (0.0) 3 (30.0) 0.006 Comorbidities 34 Diabetes mellitus 13 (27.1) 10 (26.3) 3 (30.0) 1.000 Hypertension 19 (39.6) 14 (36.8) 5 (50.0) 0.694 Dyslipidemia 11 (22.9) 8 (21.1) 3 (30.0) 0.86 Asthma 6 (12.5) 6 (15.8) 0 (0.0) 0.42 Atrial fibrillation 5 (10.4) 3 (7.9) 2 (20.0) 0.594 Coronary artery disease 4 (8.3) 1 (2.6) 3 (30.0) 0.032 Congestive heart failure 4 (8.3) 2 (5.3) 2 (20.0) 0.391 Hypothyroidism 4 (8.3) 2 (5.3) 2 (20.0) 0.391 Obstructive sleep apnea 2 (4.2) 2 (5.3) 0 (0.0) 1.000 Risk factors for VTE 41 Overweight/ obese 6 (12.5) 6 (15.8) 0 (0.0) 0.42 Immobility 1 (2.1) 1 (2.6) 0 (0.0) 1.000 Prior VTE 3 (6.2) 1 (2.6) 2 (20.0) 0.199 Advanced age (>40 years) 38 (79.2) 30 (78.9) 8 (80.0) 1.000 Hospitalization, surgery 2 (4.2) 1 (2.6) 1 (10.0) 0.882 Family history of VTE, stroke 2 (4.2) 1 (2.6) 1 (10.0) 0.882 Recent or recurrent cancer 1 (2.1) 0 (0.0) 1 (10.0) 0.468 Serology 48 D-dimer >500ng/ml 38 (79.2) 30 (78.9) 9 (90.0) 0.403 Lactate (mml/L) ** 4.93±4.40 5.74±4.39 0.90 N/A LDH (units/L) ** 454.89 ±222.34 454.89±222.34 0 (0.0) N/A Ferritin >1000 ng/ml 8 (16.7) 8 (21.1) 0 (0) N/A EKG 4 4 (8.3) 4 (10.5) 0 (0.0) 0.668 Normal sinus rhythm 3 (6.3) 3 (7.9) 0 (0.0) Sinus tachycardia 1 (2.1) 1 (2.6) 0 (0.0) Echocardiogram 11 Right ventricular dysfunction 6 (12.5) 6 (15.8) 0 (0.0) 0.42 Values are presented as number and percentages (%). **Median, N/A- not available, COVID-19: coronavirus disease 2019, PE: pulmonary embolism, DVT: deep vein thrombosis, VTE: venous thromboembolism, EKG: electrocardiogram, ICU: intensive care unit, LDH: lactic acid dehydrogenase, O2: Oxygen, SOB: shortness of breath
- Table 1
- Characteristics of published cases of coronavirus associated venous thromboembolism (continuation).
Variable Valid= (n/48) Total cases (n=48) Confirmed PE (n=38) Confirmed DVT (n=10) P-value Covid management 25 Hydroxychloroquine 15 (31.2) 15 (39.5) 0 (0.0) 0.044 Azithromycin 6 (12.5) 6 (15.8) 0 (0.0) 0.42 Amoxicillin clavulanate 4 (8.3) 4 (10.5) 0 (0.0) 0.668 Dexamethasone 5 (10.4) 3 (7.9) 2 (20.0) 0.594 Cefepime 5 (10.4) 3 (7.9) 2 (20.0) 0.594 Linezolid 3 (6.2) 2 (5.3) 1 (10.0) 1.000 Outcome 48 Recovery or discharge 37 (80.4) 30 (81.1) 7 (77.8) 1.000 Death 9 (19.6) 7 (18.9) 2 (22.2) 1.000 Undetermined 2 (4.1) 1 (2.6) 1 (0.10) 0.882 Severity of Covid infection 28 ICU admissions 10 (20.8) 9 (23.7) 1 (10.0) 0.663 Average length of ICU admission (days) 3.31 (±8.25) 1.84 (±3.54) 40.00 (1 patient) N/A Average length of hospital admission 4.90 (±4.45) 4.83 (±4.67) 5.50 (±2.12) 0.847 Complication during admission 13 (27.1) 10 (26.3) 3 (30.0) 1.000 Time of dx till VTE discovery** 10.30 (±7.92) 10.82 (±8.28) 8.11 (±6.11) 0.363 Duration of COVID symptoms** 43 7.91 (±7.03) 7.97 (±7.45) 7.57 (±4.65) 0.892 Values are presented as number and percentages (%). **Median, N/A- not available, COVID-19: coronavirus disease 2019, PE: pulmonary embolism, DVT: deep vein thrombosis, VTE: venous thromboembolism, dx: diagnosis, ICU: intensive care unit
- Table 2
- Imaging characteristics of confirmed cases of coronavirus associated venous thromboembolism.
Author name Age/Gender D-dimer >500 ng/mL** Chest x-ray with pneumonia Echocardiogram CTPA Duplex ultrasound / CUS Other Davis, Kenyani 34 M N/A + N/A Right Lower Lobe PE N/A N/A Aoi et al 70 F + N/A Dilated RV and clot in transit Saddle PE N/A N/A Brüggemann et al 57 M ++ + N/A Right pulmonary artery and bilateral sub-segmental PE N/A CT Brain showed right frontal lobe infarction Colombo et al 73 F N/A + N/A Bilateral PE Normal N/A Delcros et al 31 M ++ N/A N/A Bilateral PE N/A CT venography showed a femoropopliteal DVT expanding to the subrenal vena cava Fiorini et al 26 F + N/A Normal Bilateral sub-segmental PE Normal N/A Haider et al 46 F + + N/A Bilateral PE (segmental and sub-segmental) N/A N/A Kasinathan et al 20 F + + N/A Bilateral PE N/A N/A Mene-Afejuku et al 67 M ++ + N/A Bilateral PE N/A N/A 58 F ++ + N/A Large saddle PE extending to lobar, segmental, and subsegmental pulmonary arteries. N/A N/A 89 F ++ N/A N/A Bilateral PE N/A N/A 82 F ++ + N/A Bilateral PE N/A N/A Akel et al 28 F ++ N/A Dilated RV with interventricular septal flattening Bilateral extensive PE N/A N/A 52 M ++ + N/A Bilateral PE N/A N/A 62 M ++ N/A McConnell’s sign Bilateral PE N/A N/A 49 M ++ N/A RV dilatation along with systolic and diastolic flattening of the septum Right segmental PE N/A N/A 59 F + + N/A Bilateral PE N/A N/A 69 M ++ N/A N/A Large bilateral PE N/A N/A Fortuzi et al 52 M ++ + N/A Right PE N/A N/A 74 F ++ N/A N/A Bilateral PE N/A N/A 31 M + N/A N/A Right sub-segmental PE N/A N/A Kanso et la 68 M ++ + N/A Right segmental PE N/A N/A 62 M ++ + N/A Left segmental PE N/A N/A Lewis et al 77 M ++ N/A N/A Bilateral PE N/A N/A 70 M + N/A N/A N/A Partial occlusion in popliteal and femoral veins N/A 76 M ++ N/A N/A Right segmental and sub-segmental PE N/A N/A 80 M N/A N/A N/A N/A DVT of femoral vein N/A 92 M + Care withdrawn Manek et al 66 M ++ N/A N/A Bilateral PE DVT of the left femoral vein N/A Mangala et al 55 M + N/A N/A Right segmental PE. N/A EKG showed normal sinus rhythm 67 F N/A + N/A PE in right upper lobe pulmonary artery and segmental branches of right lower lobe pulmonary artery N/A EKG showed normal sinus rhythm Nelson, et al 61 M + + N/A Right segmental PE Multiple areas of turbulent flow in lower extremity N/A 54 M ++ + N/A Negative for PE Turbulent blood flow in the right lower extremity and right calf vein thrombosis N/A Overstada et al 55 M ++ N/A N/A N/A DVT in the left leg N/A 39 M + N/A N/A Bilateral PE N/A N/A 57 M + N/A N/A Left segmental PE N/A N/A 55 M ++ + N/A Bilateral PE N/A N/A Sakr et al 66 M ++ + Dilated RV and paradoxical septal motion Bilateral PE Right femoral vein thrombosis N/A 65 M N/A + Mild dilatation of the RV with preserved LV function Right segmental PE Normal N/A 56 M N/A + N/A Right segmental PE Normal N/A 41 M N/A + Acute right heart failure with paradoxical septal motion and large thrombus in the right pulmonary artery N/A Thrombosis of the left femoral vein N/A 49 M N/A + N/A Right segmental PE Normal N/A Salam et al 36 M + + McConnell’s sign with septal flattening Saddle PE with significant clot burden. Normal EKG showed sinus tachycardia Sethi et al 44 M ++ + EF of 45%, severely dilated and reduced RV systolic function with a flattening of the septum. N/A Normal N/A Singh et al 69 F + N/A N/A N/A N/A CTA showed thrombotic occlusion in tibial arteries on the right leg, aortic thrombus in the aorta, with evidence of splenic infarct. 33 M + N/A N/A N/A N/A CTA showed occlusive thrombus at the aortic bifurcation with near-complete occlusion of right common iliac arteryy. 69 F + N/A EF of 25%-35% and evidence of a large LV thrombus at the apex. N/A N/A N/A Uppuluri et al 32 M N/A + N/A Left segmental and subsegmental PE. N/A EKG showed normal sinus rhythm N/A: not available, RV: right ventricle, EF: ejection fraction, LV: left ventricle, PE: pulmonary embolism, Echo: echocardiogram, CT: computed tomography, CTPA: CT pulmonary angiography, CUS: compression ultrasonography, CTA: computed tomography angiography, EKG: electrocardiogram, F: female, M: male, **(+) means >500 ng/mL, (++) means >5000 ng/mL.
- Table 3
- Anti-coagulation type used to treat confirmed cases of coronavirus associated venous thromboembolism.
Author name Age/Gender Type of anticoagulant Outcome Complications Prior to VTE VTE treatment (during hospitalization) Upon discharge Kenyani Davis 34 M N/A N/A NOAC Recovery or discharge N/A Aoi et al 70 F Heparin IV Heparin N/A Death Cardiac arrest Brüggemann et al 57 M LMWH (nadroparin) LMWH (tinzaparin) N/A Recovery or discharge Ischemic stroke Colombo et al 73 F LMWH (enoxaparin) LMWH (enoxaparin) NOAC Recovery or discharge Obstructive shock Delcros et al 31 M LMWH (enoxaparin) LMWH (enoxaparin) LMWH (enoxaparin) Recovery or discharge N/A Fiorini et al 26 F N/A LMWH (enoxaparin) NOAC Recovery or discharge N/A Haider et al 46 F Heparin LMWH (enoxaparin) NOAC Recovery or discharge N/A Kasinathan et al 20 F N/A LMWH (enoxaparin) LMWH (enoxaparin) Recovery or discharge N/A Mene-Afejuku et al 67 M Heparin NOAC NOAC Recovery or discharge N/A 58 F Heparin LMWH (enoxaparin) NOAC Recovery or discharge N/A 89 F Heparin IV Heparin NOAC Recovery or discharge N/A 82 F LMWH (enoxaparin) LMWH (enoxaparin) NOAC Recovery or discharge N/A Akel et al 28 F LMWH (enoxaparin) tPA, LMWH (enoxaparin) NOAC Recovery or discharge N/A 52 M LMWH (enoxaparin) LMWH (enoxaparin) NOAC Recovery or discharge N/A 62 M N/A tPA, IV heparin NOAC Recovery or discharge N/A 49 M LMWH (enoxaparin) LMWH (enoxaparin) NOAC Recovery or discharge N/A 59 F LMWH (enoxaparin) LMWH (enoxaparin) NOAC Recovery or discharge N/A 69 M Heparin IV Heparin NOAC Recovery or discharge N/A Fortuzi et al 52 M Heparin IV Heparin N/A Death AKI, Septic shock 74 F LMWH (enoxaparin) LMWH (enoxaparin) NOAC Recovery or discharge N/A 31 M N/A NOAC NOAC Recovery or discharge N/A Kanso et la 68 M LMWH (enoxaparin) LMWH (enoxaparin) Warfarin Recovery or discharge N/A 62 M LMWH (enoxaparin) LMWH (enoxaparin) NOAC Recovery or discharge N/A Lewis et al 77 M NOAC (Apixaban) LMWH (enoxaparin) N/A Death Multi-system organ failure 70 M NOAC (Apixaban) LMWH (enoxaparin) NOAC (Apixaban), LMWH (enoxaparin), loaded warfarin Recovery or discharge N/A 76 M NOAC (Rivaroxaban) LMWH (enoxaparin) NOAC (Rivaroxaban) Recovery or discharge N/A 80 M NOAC (Rivaroxaban) LMWH (enoxaparin) LMWH (enoxaparin) Death N/A 92 M NOAC (Apixaban) Care withdrawn Care withdrawn Death Left-sided facial droop, left-sided hemiplegia and stroke Manek et al 66 M N/A IV heparin NOAC (Apixaban) Recovery or discharge N/A Mangala et al 55 M LMWH (enoxaparin) LMWH (enoxaparin) NOAC (Apixaban) Recovery or discharge aspiration pneumonia 67 F LMWH (enoxaparin) IV heparin NOAC (Apixaban) Recovery or discharge N//A Nelson et al 61 M N/A IV heparin N/A Death Septic shock 54 M N/A tPA, LMWH (enoxaparin) N/A Death N/A. Overstada et al 55 M N/A NOAC (Apixaban) N/A Recovery or discharge N/A 39 M N/A NOAC (Apixaban) NOAC (Apixaban) Recovery or discharge N/A 57 M N/A NOAC (Apixaban) NOAC (Apixaban) Recovery or discharge N/A 55 M N/A LMWH (Dalteparin) LMWH (Dalteparin) Recovery or discharge N/A Sakr et al 66 M N/A tPA and IV heparin N/A Death Progressive multi-organ failure 65 M N/A LMWH (enoxaparin) LMWH Recovery or discharge N/A 56 M N/A LMWH (enoxaparin) LMWH Recovery or discharge N/A 41 M N/A tPA, VA -ECMO, LMWH (tinzaparine) LMWH Recovery or discharge Ventilator-associated pneumonia, severe hypoxemia. 49 M LMWH (enoxaparin) LMWH N/A Death Necrotizing pneumonia Salam et al 36 M N/A tPA , LMWH (enoxaparin) NOAC (Apixaban) Recovery or discharge N/A Sethi et al 44 M N/A tPA, LMWH (enoxaparin), VA -ECMO LMWH Recovery or discharge Bleeding within the oropharynx Singh et al 69 F N/A IV heparin NOAC (Rivaroxaban) with low dose ASA Recovery or discharge N/A 33 M N/A IV heparin NOAC (Rivaroxaban) Recovery or discharge N/A 69 F NOAC (Apixaban) LMWH N/A Undetermined Massive stroke in the territory of the left middle cerebral artery and clinically deteriorated. Uppuluri et al 32 M N/A LMWH (enoxaparin) NOAC (Apixaban) Undetermined N/A VTE: venous thromboembolism, N/A: not available, M: male, F: female, LMWH: low molecular weight heparin, IV: intravenous; NOAC: novel oral anticoagulants, VA-ECMO: venoarterial extracorporeal membrane oxygenation, AKI: acute kidney injury, tPA: tissue plasminogen activator, ASA: acetylsalicylic acid (aspirin)
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.