


Abstract
Objectives: To compare the efficacy of negative pressure wound therapy (NPWT) and alginate dressings on wound bed preparation prior to split thickness skin graft (STSG) surgery for patients with chronic diabetic foot ulcers (DFUs).
Methods: Between September 2022 and March 2023, we completed a randomized controlled trial in Nanjing First Hospital and PLA 454 Hospital. Patients were divided into 2 groups: i) the NPWT group (with vacuum-assisted closure, n=50); ii) the control group (with alginates dressings, n=50). Once DFU wound was filled with healthy granulation tissues, STSG surgery was performed. The time to STSG surgery was regarded as the primary outcome. The survival rates of skin graft, the wound blood perfusion, the wound neutrophil extracellular traps (NETs) formation, and polarization of M1 and M2 macrophages in DFU wounds were regarded ad secondary outcomes.
Results: Patients in the NPWT group had less time to STSG surgery than the control group. The patients in the NPWT group had prominently increased survival rates of skin graft, increased wound blood perfusion, and decreased NET formation in comparison with the control group. The macrophages in DFU wounds switched from M1 to M2 phenotype in the NPWT group.
Conclusion: Negative pressure wound therapy is superior to conventional moist dressings in wound bed preparation prior to STSG surgery for patients with chronic DFUs.
For patients with diabetes, diabetic foot ulcers (DFUs) represent serious complications. Diabetic foot ulcers include infections, ulcers, and tissue destructions of the foot below the medial malleolus. Diabetes mellitus plagues more than 400 million people around the world. Researchers predict that in 2040, more than 600 million people will suffer from diabetes.1 For patients with diabetes, the probability of developing DFUs exceed 20%. Diabetic foot ulcers cause many complications, including infections, sepsis, multiple organ dysfunctions, and limited mobility.2 Compared to diabetic patients without DFUs, diabetic patients with DFUs are associated with a 2.5-fold higher risk of 5-year mortality. In one year, the relapse rates of DFUs are approximately 40%. In 3 years, the relapse rates of DFUs exceed 60%.3 Diabetic foot ulcers bring huge economic burdens to the society owing to the necessity of multiple surgical procedures, nursing care, and frequent hospital admissions.4
Patients with DFUs experience great challenges during clinical treatment. The standard of care involves radical surgical debridement, treatment of infections, control of blood glucose, improvement of blood perfusion, offloading therapies, and closure of DFU wounds.5 There are many advanced treatments to close DFU wounds, such as negative pressure wound therapy (NPWT), and cellular, or tissue-based therapies particularly in North America, Oceania, and parts of Asia. Notably, split thickness skin graft (STSG) is one of the techniques of choice to close DFU wounds in Europe and parts of the Middle East when DFU wounds do not respond to standard of care for a period of time (such as 4 weeks).6 Compared to spontaneous closure, STSG surgery leads to more rapid recovery and fewer medical expenses and provides the wound with more durable barriers.7 Skin grafts fail if they are applied to the wound bed with insufficient blood supply, if the tissue has a bacterial infection, or if the patient has a serious inflammatory response. Therefore, wound bed preparation prior to STSG surgery is very important for skin grafts.8
Adequate blood perfusion plays a pivotal role in wound bed preparation. Laser speckle contrast imaging device can detect wound blood perfusion locally and noninvasively.9 Chronic DFU wounds are more prone to bacterial infections than acute wounds.10 Neutrophil extracellular traps (NETs) are network of compressed deoxyribonucleic acid strands outside the cells that are mixed with myeloperoxidase (MPO), neutrophil elastase (NE), and proteinase 3. Neutrophil extracellular traps are generated following bacterial infections. Neutrophil extracellular traps have antibacterial activities. Excessive NETs are associated with excessive inflammatory responses and tissue damage.11 Therefore, NETs are detrimental to wound bed preparation. Bacterial infections promote macrophage migration to the wound. The effects of macrophages on wound bed preparation depend on macrophage phenotypes.12
The most appropriate intervention should be selected to improve wound bed preparation. In previous studies that compared the efficacy of novel therapies with standard therapy, alginate dressings were applied in the control group.13 The alginate dressings created a moist environment and promoted autolytic debridement and neovascularization.5 In this study, we regarded patients using alginate dressings as the control group. Negative pressure wound therapy is an important means to treat chronic and refractory wounds by providing adjustable negative pressure. According to the guidelines, NPWT is recommended as local therapy to treat patients with DFUs.14 In our study, all the patients received STSG surgery to repair DFU wounds, but the methods of wound bed preparation prior to STSG surgery were different. For patients in the NPWT group, wound bed preparation was facilitated by a vacuum-assisted closure (VAC) device. For patients in the control group, wound bed preparation was facilitated by the alginate dressing change method. The study objective is to compare the efficacy of NPWT and alginate dressings on wound bed preparation prior to STSG surgery, as well as to investigate the underlying mechanisms.
Methods
The ethical approval was obtained from the Ethics Committee (approval number: KY20220825-08, approval date: August 25th, 2022). The registration number is ChiCTR2200059940. Clinical research of human subjects complied with principles of Helsinki Declaration. The patients with DFUs in Nanjing First Hospital and PLA 454 Hospital (located in Nanjing, China) between September 2022 and March 2023 were enrolled in this study. We obtained the signed consent form from patients or their authorized family members.
Patients were assigned into the NPWT group (with VAC) or the control group (with alginates dressings) (in 1:1 ratio, randomly) with a random-number generator in blocks of 10. The randomization was carried out centrally through the electronic system in order to conceal the randomization sequence until interventions were assigned. Nontransparent envelopes (for patient assignment) containing the random group assignment were numbered according to order. Technicians who did not know the grouping assignment collected the clinical data.
The inclusion criteria were patients who have type 1 or 2 diabetes with a chronic wound located on the foot below the medial malleolus, aged 20-80 years, Wagner grade 2 to 3, chronic DFU wounds (duration of disease ≥2 weeks), ankle brachial index (ABI) 0.5~0.9, wound area 8~20 cm2. While the exclusion criteria were foot ulcers caused by other reasons, loss to follow-up, pregnancy, lactation, organ dysfunctions (heart failure, respiratory dysfunction, liver dysfunction, renal insufficiency or intestinal failure), coagulation dysfunction, or autoimmune disorders. Patients who received growth factors or hyperbaric oxygen therapies for DFU wounds within 1 month before enrolment were not included. Patients who received immunosuppressive therapies within 6 months before enrolment were not included.
All enrolled patients received the following treatments. When patients were admitted to hospital, we applied radical surgical debridement to cut off the necrotic and unhealthy tissues in the wound. We prescribed antibiotics for patients with bacterial infections (fever, positive bacterial culture, procalcitonin (PCT)>0.5 ng/ml, C-reactive protein (CRP)>50 mg/L). Since the patients would receive STSG surgery recently, insulin pumps were applied for glycaemic control (therapeutic goal: fasting blood glucose (FBG) ≤8.8 mmol/l).15 The strategies for improving blood perfusion included keeping warm, smoking cessation, and the combined use of vasodilator and antiplatelet aggregation drugs (aspirin, dipyridamole, prostaglandin, or clopidogrel). The offloading therapies were as follows: During hospitalization, all the patients were asked to elevate their affected leg with a cushion. During the follow-up period, the patient’s foot was offloaded using a removable cast walker (Chushi Technology Company, Shanghai, China) or standardized total-contact cast kit (Chushi Technology Company, Shanghai, China).
All the patients received STSG surgery, but the methods of wound bed preparation prior to STSG surgery were different. For patients in the NPWT group, wound bed preparation was facilitated by a VAC device. For patients in the control group, wound bed preparation was facilitated by the alginate dressing change method.
A mini-computer with a touch screen and a negative pressure-producing pump constitute the VAC system (KCI Company, Texas, America). For patients in the NPWT group, the black foam was tailored to the specific needs of the wound. Then, we put the tailored black foam and transparent occlusive on the wound. The VAC pump was programmed to deliver a negative pressure of 125 mmHg (in the continuous mode). The VAC foams were changed once every 72 hours (h).
For patients in the control group, the wound was disinfected, and then covered with alginates dressings (Biatain®, Coloplast Company, Copenhagen, Denmark) and fabric dressings (MEDICOM Company, Shanghai, China). The dressings were changed once every 48 h.
Before radical surgical debridement (Day 0), peripheral venous blood and wound granulation tissues (1 mL) were collected from the patients for analysis. After NPWT or alginate dressing change therapy for 6 days (Day 6), peripheral venous blood and wound granulation tissues (1 mL) were collected again. The definition of healthy granulation tissues: bright red, grainy appearance, soft, pulsatile, and painless. The wound bed was judged as ready for skin grafting based on healthy granulation tissues and the absence of infections. Three experts who were unaware of the grouping made decisions on the timing of skin grafting surgery.
For all patients in the 2 groups, once their wound beds were appropriate for skin grafting, STSGs were performed. Medium-thickness STSGs (at a depth of 0.5-0.6 mm) were harvested from the upper lateral thighs using a drum dermatome (Belevor Medical Technology Limited Company, Berlin, Germany) to repair skin defects of the foot. After washing the seroma under the skin graft, petrolatum gauze (Shunda Medical Technology Limited Company, Shanghai, China) was applied to the recipient site as a primary dressing. Then, we covered the recipient site with fabric dressings (Shunda Medical Technology Limited Company, Shanghai, China) and compression bandages. The donor sites were also successively covered with petrolatum gauze, fabric dressings, and compression bandages.
The primary outcome included the time to STSG surgery (the duration from first surgical debridement to STSG surgery). The secondary outcomes included the survival rates of skin graft, the wound blood perfusion, the wound NET formation, and percentages of M1 and M2 macrophages in DFU wounds of the 2 groups. Patients were assessed for adverse events. Adverse events were defined as any unexpected medical occurrence after randomization, including unfavourable and unintended signs, symptoms, and disease. The events which led to physical deformity, inpatient hospitalization, prolongation of hospitalization or even mortality were regarded as serious adverse events.
The wound tissues were cultured for bacterial colony counts. We applied a Doppler detector (Hitachi Company, Tokyo, Japan) to calculate ankle/brachial index.The wound granulation tissues were fixed, embedded and cut into sections. The sections were stained by anti-CD31 antibody or Masson. The collagen fibers were dyed blue. The sections were observed by optical microscope (original magnification ×200, Hitachi Company, Tokyo, Japan).
We applied a laser speckle contrast imaging instrument (Perimed Company, Stockholm, Sweden) to measure blood perfusion of the DFU wounds. The imaging setting was applied with 0.2 mm/pixel spatial resolution, 25 Hz display rate and 785 nm wavelength. We applied the optical coherence tomography (Hitachi Company, Tokyo, Japan) to measure the parameters of blood vessels in the DFU wounds.
Samples were stained with anti-human NE, anti-human MPO antibodies and corresponding secondary antibodies (Abcam Company, Cambridge, England). Visualization was performed with confocal microscopy (Hitachi Company, Tokyo, Japan).
The wound granulation tissues were washed, lysed and homogenized. The percentages of M1 macrophages and M2 macrophages in DFU wounds were detected by flow cytometry (M1 macrophages: CD86+CD11b+, M2 macrophages: CD206+CD11b+).
Statistical analysis
The calculation module “Two-Sample T-Tests Assuming Equal Variance” in PASS 2013 statistical software (NCSS, statistical software, N.Y., USA) was used to determine the sample size.16 The sample size was calculated depending on the mean time to STSG surgery in our previous study (the control group: 11±4 days, the NPWT group: 7±4 days). The type II error rate was set to 0.1. With the above assumptions, we needed to enroll at least 18 patients for in each group (the total amount: 36 patients) (type I error rate (2-sided): 0.05, power: 0.9). To accommodate for the loss rate and increase credibility, we planned to recruit 100 patients. In cases of serious adverse events, the clinical trial was stopped urgently to ensure the safety of patients. If 2 or more of the top 10 patients in the clinical trial had serious adverse events, the trial would be discontinued. This situation did not occur in our clinical trial.
The intention-to-treat population, which included all the patients who underwent randomization were used for all the efficacy and safety analyses. Continuous variables were described as the mean ± standard deviation (SD) (categorical variables as numbers with percentages). We applied Chi-squared test and Student’s t test to analyze the patient and wound demographics between the treatment groups at baseline, as appropriate. The survival curve of the primary outcome (mean time to STSG surgery) was illustrated by Kaplan‒Meier plot and we compared the primary outcome between the 2 groups by the log-rank test. The secondary outcomes were compared by Chi-squared test (survival of skin graft) or Student’s t test (the wound blood perfusion, the wound NETs formation, and percentage of M1 and M2 macrophages). We applied the analysis of covariance (ANCOVA) models (covariates: the baseline value, underlying normality assumption: Shapiro–Wilk test) to compare the laboratory outcomes (point estimates and 95% confidence intervals). To control type I error inflation caused by multiple comparisons, the statistical significance level of secondary outcomes was adjusted with Bonferroni adjustment. We carried out statistics analyses by IBM SPSS Statistics for Windows, version 19.0 (IBM Corp., Armonk, N.Y., USA). For the primary outcome, p-value of <0.05 was considered as significance (a 2-sided p).
Results
The period of recruitment was 6 months. The period of follow-up was 2 months. A total of 201 patients were recruited, and 98 patients were excluded (not meeting inclusion criteria: n=63, declined to participate: n=22, other reasons: n=13). A total of 103 patients were allocated into the NPWT group (n=52) and the control group (n=51) randomly. Finally, 50 patients were analyzed in each group (for NPWT group: withdrew consent: 2, loss to follow-up: none; For the control group: withdrew consent: 1, loss to follow-up: none). The 2 groups were well matched (including in gender, age, Wagner grade, baseline wound area, underlying disease or and duration of diabetes mellitus). The patients’ demographics were displayed (Table 1).
- Demographics of patients in the 2 groups.
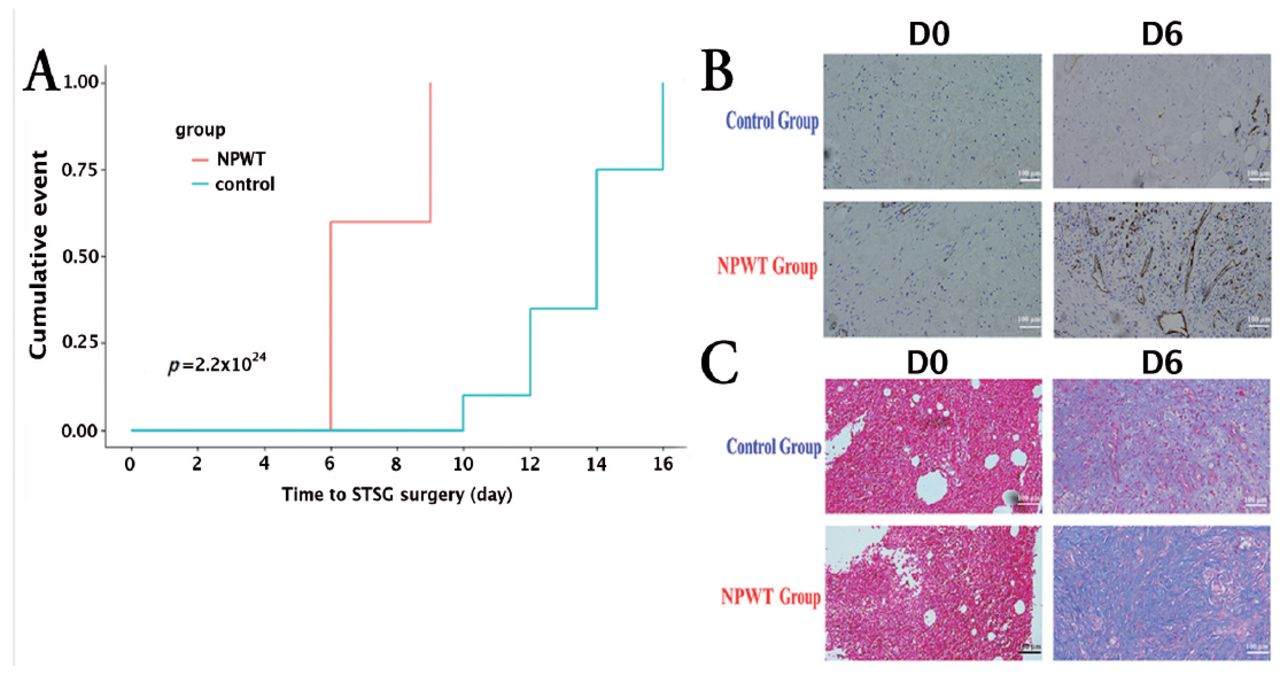
A Kaplan‒Meier plot also demonstrated that patients in the NPWT group (mean days: 7.2, 95% CI: 6.8 to 7.6) had less time to STSG surgery in comparison with the control group (mean days: 13.6, 95% CI: 13.1 to 14.7), and the log-rank p=2.2×10-24 (Figure 1A). The number of hospital days in the NPWT group (mean days: 15.0, 95% CI: 13.8 to 16.2) was also significantly reduced in comparison to the control group (mean days: 24.1, 95% CI: 22.3 to 25.8, p=1.2×10-53). In the NPWT group, the skin graft had a 100% survival rate. In contrast, the skin graft had a 76% survival rate in the control group (mean difference: 24%, 95% CI: 23.1% to 27.5%, p=3.1×10-19).
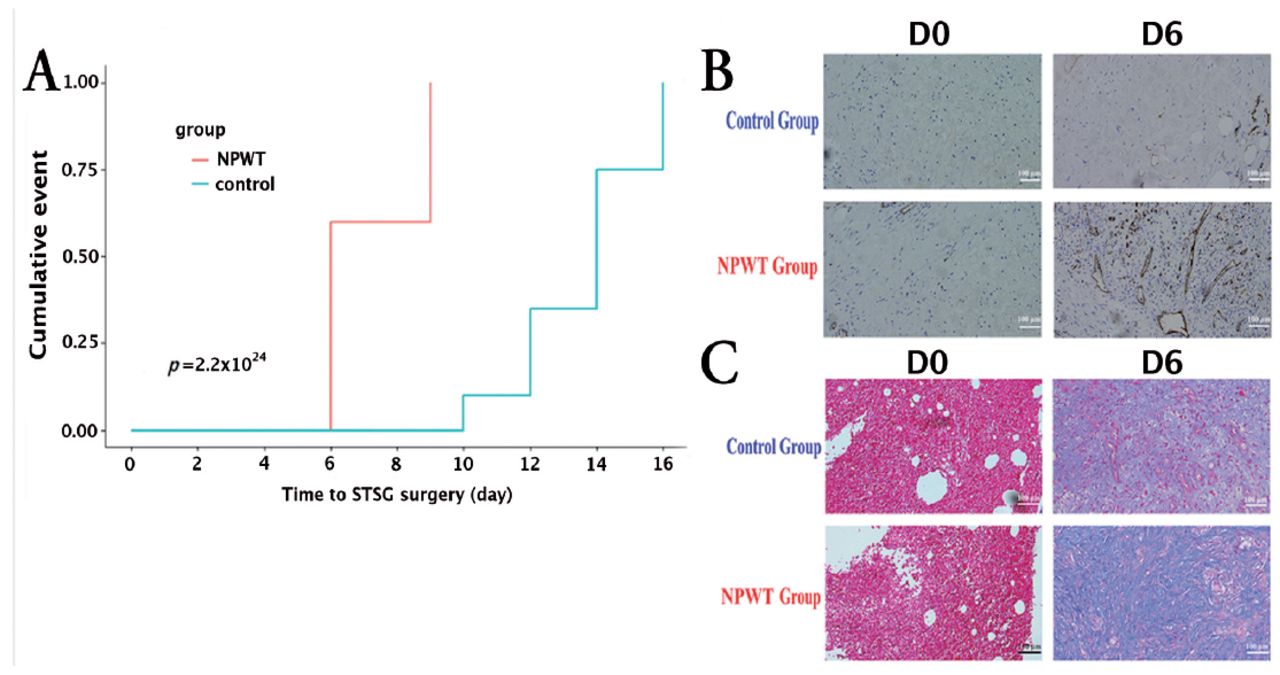
- A Kaplan‒Meier plot and histological analysis. (A) A Kaplan‒Meier plot demonstrated that patients in the NPWT group had less time to STSG surgery. X axis: time to STSG surgery (day), Y axis: cumulative event. (B) Representative CD31 immunohistochemical staining for granulation tissues (original magnification ×200). (C) Representative Masson staining for collagen fibers (original magnification ×200). NPWT: negative pressure wound therapy, STSG: split thickness skin graft
On Day 6, serum levels of white blood cells counts (WBC) and CRP were dramatically diminished in the 2 groups. The statistical analysis showed that these decreases were more obvious in the NPWT group. On Day 6, serum levels of albumin were dramatically increased in the 2 groups. The statistical analysis showed that this increase was more obvious in the NPWT group (Table 2).
- The laboratory variables before and after treatment.
Histological analysis revealed that, compared to the control group, the patients in the NPWT group had an enhanced angiogenic response and collagen deposition (Figure 1B-C).
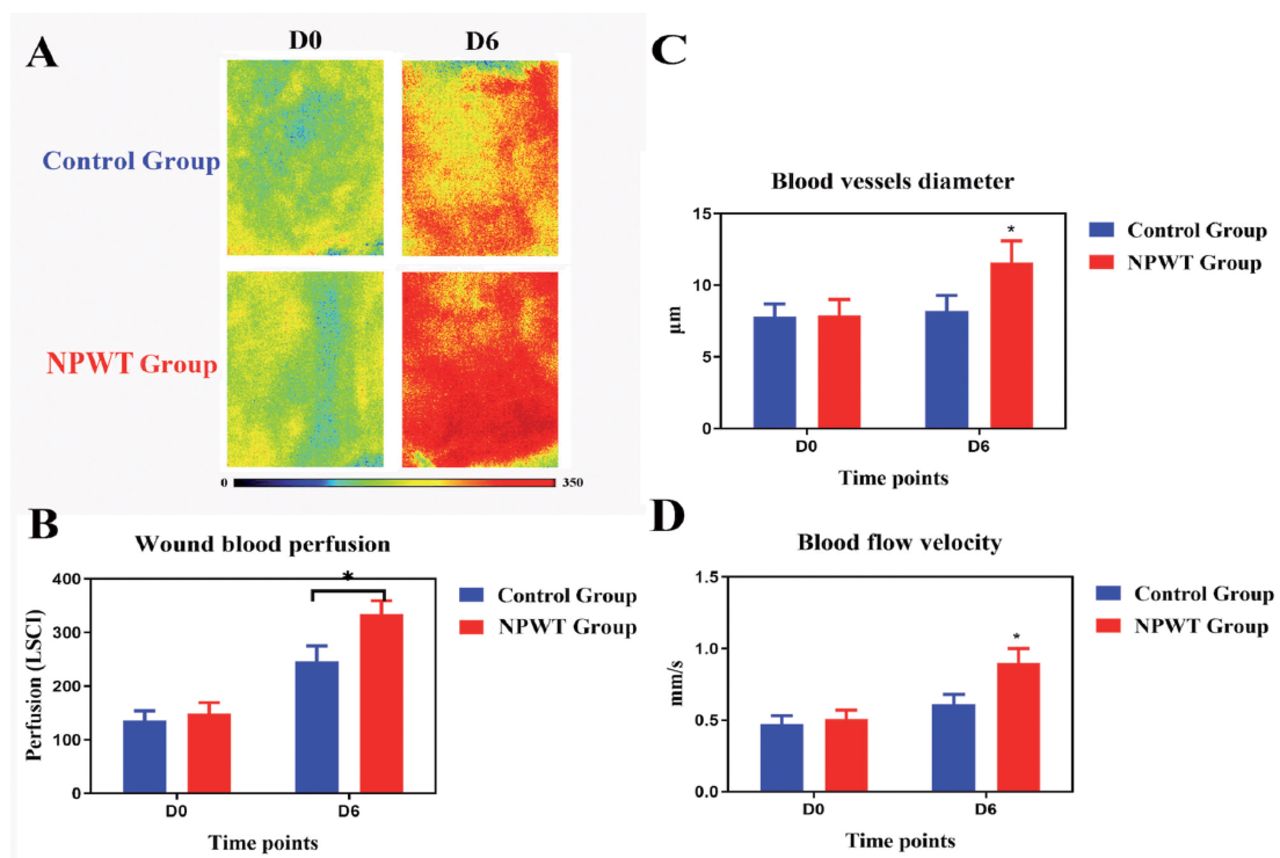
On Day 0, the wound blood perfusion was low in the 2 groups. Blood perfusion was distributed differently in the wound area. On Day 6, we found that the blood perfusion dramatically enhanced in the NPWT group in comparison to the control group (334±42 LSPU in the NPWT group versus 247±42 LSPU in the control group, p=4.6×10-4) (Figure 2). The blood vessel diameters and blood flow velocity were much greater in the NPWT group than the control group.
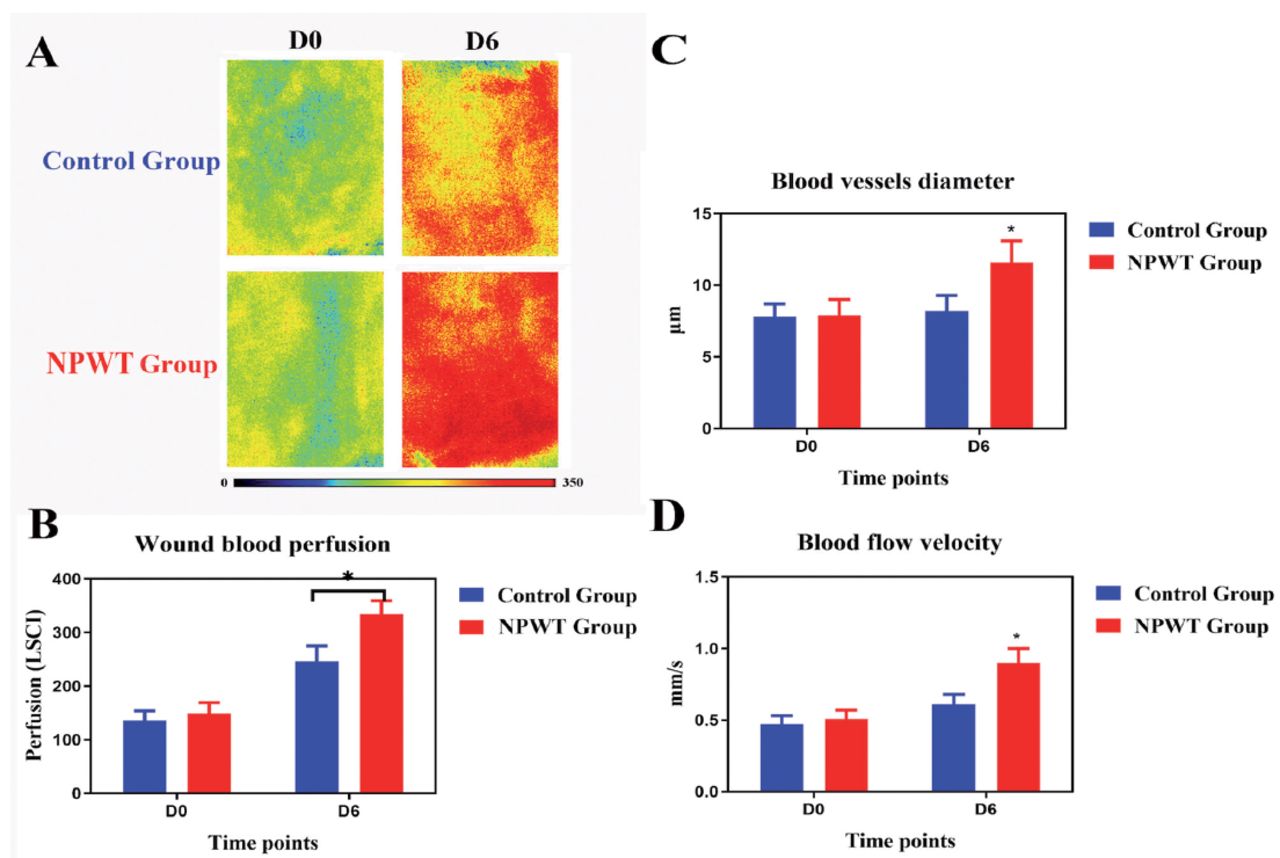
- The wound blood perfusion. (A) The wound blood perfusion image. (B) The wound blood perfusion. X axis: time points (day), Y axis: perfusion (LSCI). *P=4.6×10-4. (C) The blood vessel diameters of DFU wounds. X axis: time points (day), Y axis: µm. *P=1.2×10-4. (D) The blood flow velocity of DFU wounds. X axis: time points (day), Y axis: mm/s. *P=3.5×10-5. LSCI: laser speckle contrast imaging, DFU: diabetic foot ulcer
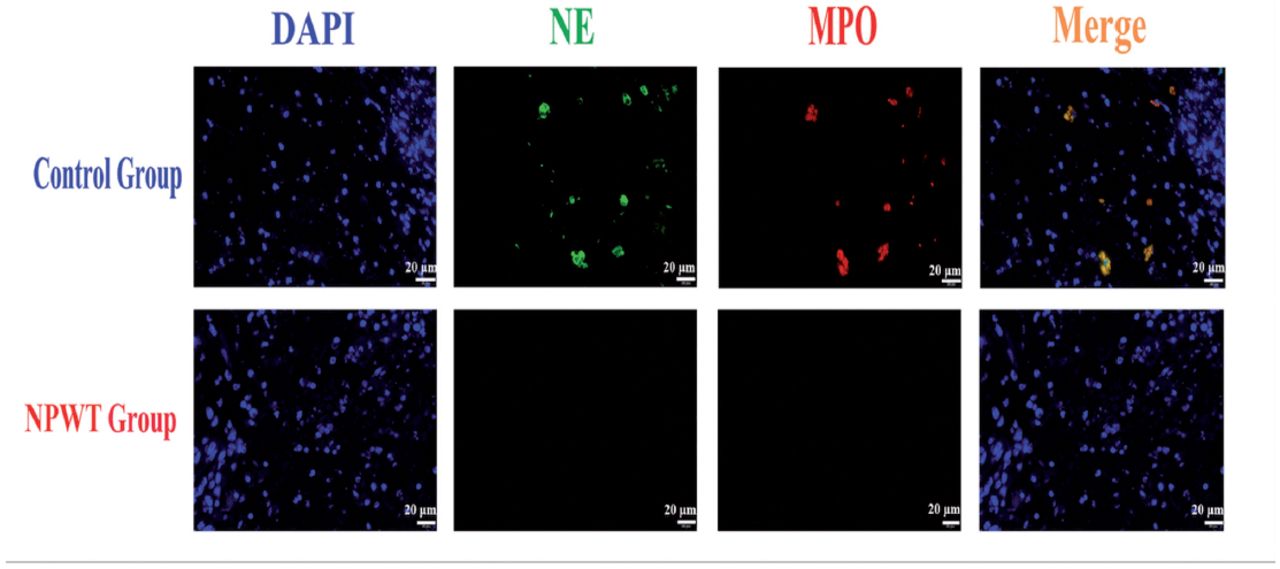
On Day 0, for the 2 groups, the predominant organisms in the wounds were Staphylococcus aureus, Pseudomonas aeruginosa and Escherichia coli (For the NPWT group: Staphylococcus aureus: 26%, Pseudomonas aeruginosa: 30%, Escherichia coli: 24%; For the control group: Staphylococcus aureus: 24%, Pseudomonas aeruginosa: 24%, Escherichia coli: 16%). Figure 3 showed representative immunofluorescent double labelling results for NETs in the 2 groups on Day 6. In the control group, we observed overlapping staining for NE and MPO, confirming large amounts of NET structures in DFU wounds. Compared to the control group, the patients in the NPWT group had a significantly reduced number of NETs.
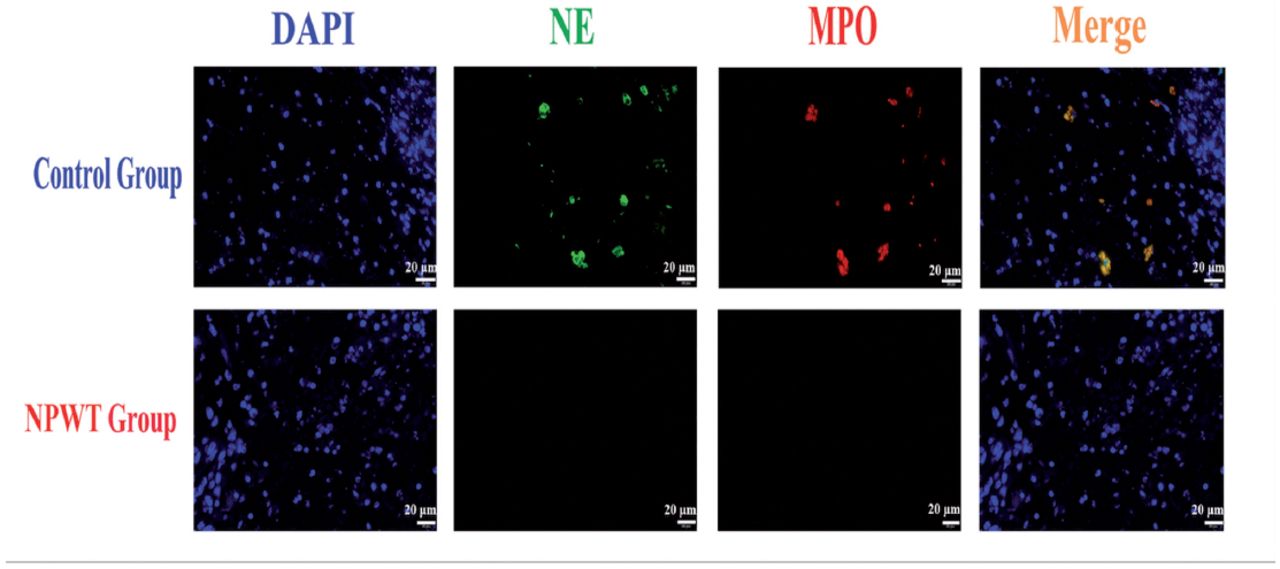
- The NET formation in DFU wounds on Day 6. NETs: neutrophil extracellular traps, DFU: diabetic foot ulcer, NE: neutrophil elastase, MPO: myeloperoxidase
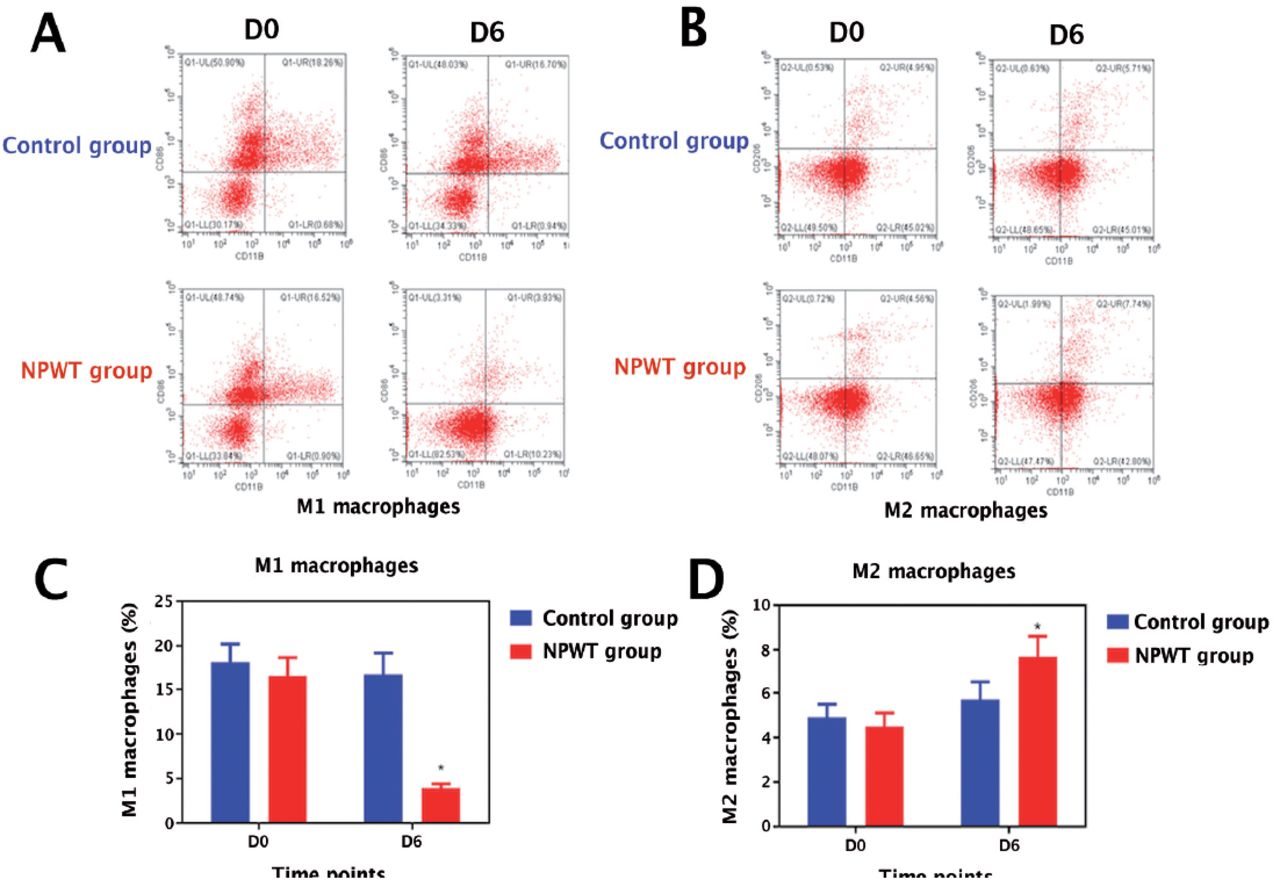
The DFU wounds in the control group displayed a pronounced M1 macrophage activation profile. In contrast, the M1 macrophages percentage was diminished in the DFU wounds of the NPWT group. Notably, the M2 macrophages percentage was increased in the DFU wounds of the NPWT group. The macrophages isolated from DFU wounds switched from M1 phenotypes to M2 phenotypes in the patients from the NPWT group (Figure 4).
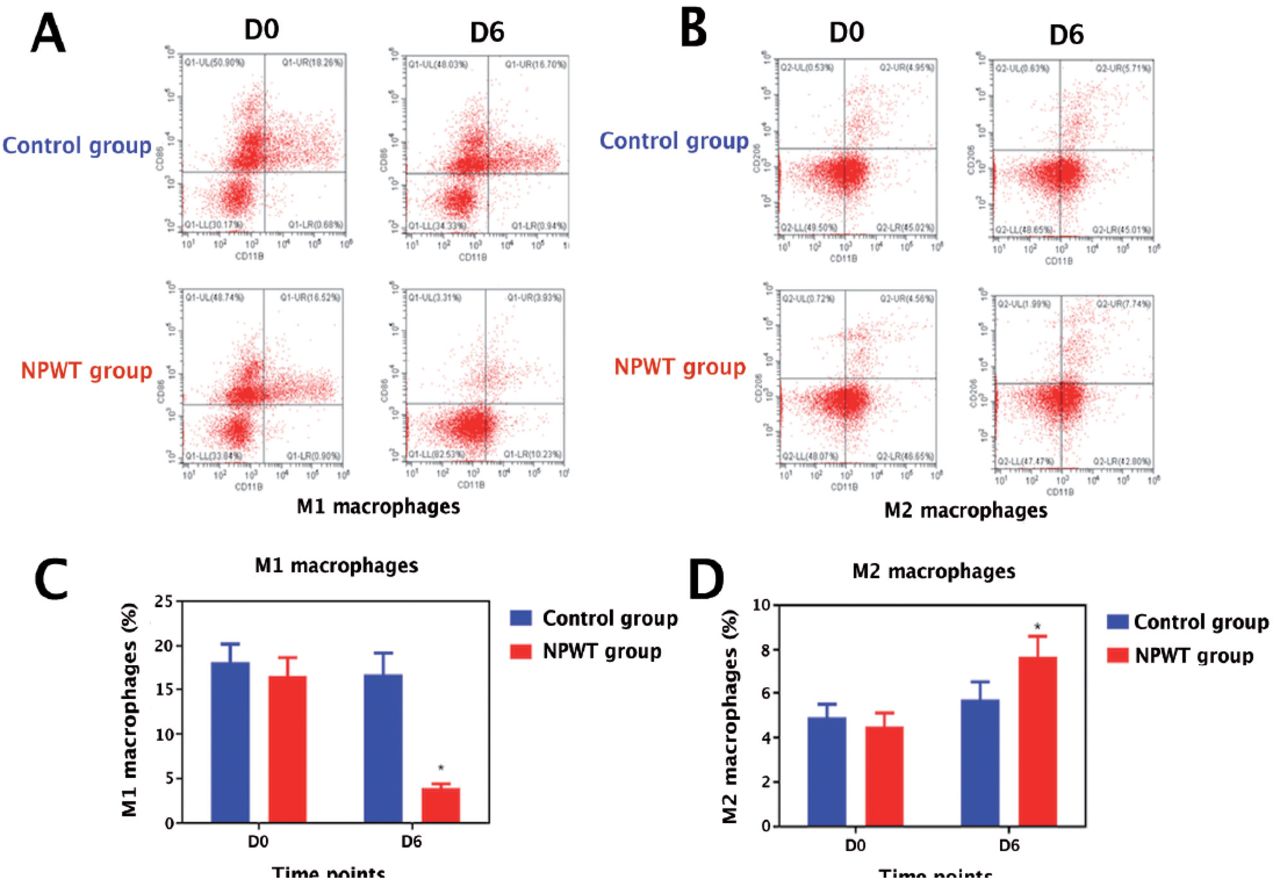
- M1 and M2 macrophages. (A) The M1 macrophages. (B) The M2 macrophages. (C) The M1 macrophages percentage in DFU wounds. X axis: Time points (day), Y axis: percentage. *P=1.5×10-4. (D) The M2 macrophages percentage in DFU wounds. X axis: yime points (day), Y axis: percentage. *P=2.3×10-5. DFU: diabetic foot ulcer.
All of the patients adapted well to NPWT, with no complications. No serious adverse events (abrasion, edema, medullitis, wound infections, cellulitis) were reported in the NPWT group or the control group.
Discussion
It is well established that NPWT has advantages over conventional moist dressings as it accelerates wound healing, promotes granulation, decreases the wound area, and reduces complication rates.17 Researchers applied NPWT to prepare wound beds prior to STSG surgery for recurrent leg ulcers. They found that in comparison with conventional wound dressings, NPWT markedly increased the STSG survival rates and decreased complication rates for leg ulcers.8 However, there have been no RCTs that compare the efficacy of NPWT and alginate dressings on wound bed preparation for chronic DFUs. Our study proved the superiority of NPWT to conventional moist dressings prior to STSG surgery to improve the wound bed.
In addition, we investigated the mechanisms underlying the superiority of NPWT. Negative pressure wound therapy has the following advantages: First, NPWT prepared the wound bed by increasing blood perfusion in the wound. Blood perfusion is responsible for transporting nutrients and oxygen, as well as stimulating the formation of granulation tissues. Local blood perfusion plays an important role in wound bed preparation.18 In patients with diabetes, hyperglycaemia prevents the activation of antioxidants. Oxidative stress activates alternative damaging biochemical pathways, leading to endothelial cell dysfunction and vascular damage.19 In addition, oxidative stress results in the inactivation of antiatherogenic enzymes, contributing to the development of vascular stenosis. Consequently, DFU wounds usually lack blood supply.20 We found that wound blood perfusion increased by many times in the NPWT group. The negative pressure around the wound promoted vasodilatation and increased the blood flow velocity. Accordingly, we speculated that the increased wound blood perfusion was due to mechanical vasodilation. Furthermore, we speculated that the increased wound blood perfusion was attributable to angiogenesis. The patients in the NPWT group had enhanced angiogenesis, as demonstrated by the increased number of CD31-positive cells. The VAC foam provides a hydrophobic foam-tissue interface. The micromechanical deformations draw tissues into the foam pores, which stimulates the generation of blood vessels.21
Second, NPWT prepared the wound bed by decreasing NET formation. Neutrophil extracellular traps are extracellular web-like strands of decondensed DNA that are mixed with MPO, NE, and proteinase 3. Neutrophil extracellular traps possess antibacterial activities. However, excessive NETs are considered to cause tissue damage.11 Myeloperoxidase can produce hypochlorous acid and tyrosyl radicals, which may cause cytotoxic injury.22 Neutrophil elastase and proteinase 3 can degrade related cytokines that are beneficial for wound healing. NETs can induce epithelial cell death, aggravate the inflammatory response and hinder tissue proliferation.23
A large number of NETs were detected in DFU wounds from the control group by immunofluorescence staining. Our results were in accordance with previous studies that showed that NETs were enhanced in diabetic patients.24 The bacterial culture results showed that the main bacteria in DFU wounds included Staphylococcus aureus, Pseudomonas aeruginosa and Escherichia coli. Chronic DFU wounds provide an ideal environment for bacterial infections, as they exhibit elevated levels of glucose and sufficient nutrients.25 Neutrophils are recruited continuously to the site of bacterial colonization. The toxins released by bacteria lead to the destruction of neutrophils and the formation of NETs. In addition, previous studies reported that hyperglycaemia can activate neutrophils to release NETs.26
In contrast, the number of NETs in DFU wounds was significantly reduced in the NPWT group. We speculated that NPWT might decrease NET formation by destroying NET structures and changing the bacterial microenvironment.
Third, NPWT prepared the wound bed by regulating the polarization of macrophages. Macrophages are classified as proinflammatory M1 phenotypes and anti-inflammatory M2 phenotypes. Macrophages are able to reversibly switch from one phenotype to another. M1 phenotype macrophages develop from macrophages under the stimulation of inteferon-gamma and tumor mercosis factor alpha. M1 macrophages induce the production of proinflammatory cytokines, ROS and nitrogen radicals. M1 macrophages contribute to host defence. However, M1 macrophages also lead to cytokine storms and tissue damage, which are deleterious for wound bed preparation.27 The development of M2 phenotype macrophages is triggered by interleukin (IL)-4 and IL-10. M2 macrophages are beneficial for wound bed preparation by producing anti-inflammatory cytokines and remodelling the extracellular matrix.28
We found that macrophages were polarized towards the M1 phenotype in DFU wounds. DFU wounds are chronic wounds with a high volume of exudate, which are prone to bacterial infections.29 In this study, bacterial infections led to the production of proinflammatory cytokines in the wound bed, thus promoting M1 macrophage polarization. In comparison with the control group, the M1 macrophages percentage prominently reduced but the M2 macrophages percentage dramatically raised in the wound bed of the NPWT group. Negative pressure wound therapy can be used repeatedly to remove exudate and necrotic tissues through the evacuation tube.30 Continuous drainage inhibited the accumulation of bacteria and regulated the proportion of pro-/anti-inflammatory cytokines, thus promoting macrophage polarization towards M2 (the wound transformed from inflammatory phase to proliferative phase).12
Study limitations
Firstly, our trial was not a multi-center RCT. Multi-center RCTs with long-term follow-up are warranted to confirm our findings. Secondly, the cost of VAC foam is rather high ($550 for the small-size foam; $700 for the middle-size foam). In developing countries where citizens are economically constrained, the application of NPWT is unaffordable.
In conclusion, compared to the control group, patients in the NPWT group had less time to STSG surgery and higher skin graft survival rates. The superiority of NPWT was due to increased wound blood perfusion, decreased NET formation and a reduced percentage of M1 macrophages in the wound bed. NPWT is superior to conventional moist dressings in wound bed preparation for patients with DFUs. The RCT design of our study provided Level 1 evidence regarding the treatment of DFUs.
Acknowledgment
We would like to thank AJE (www.aje.cn) for the English language editing.
Footnotes
Disclosure. This study was funded by the National Natural Science Foundation of China (Nos. 82202445).
- Received May 30, 2023.
- Accepted August 24, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.