


Abstract
Objectives: To measure tramadol intake in the first 24 hours post-surgery. In addition, pain scores and quality of recovery were evaluated as secondary outcomes.
Methods: A total of 80 adult patients scheduled for laparoscopic cholecystectomy were randomized into 2 groups (with and without external oblique intercostal plane block [EOIPB]). Control group of patients received standard multimodal analgesia, EOIPB was applied on each side to patients in EOIPB group in addition to multimodal analgesia. The primary outcome was to evaluate tramadol consumption at postoperative 24 hours. Secondary outcomes were evaluating the Numeric Rating Scale (NRS) scores, postoperative Quality of Recovery score (QoR-15), sedation score, the incidence of nausea and vomiting, and antiemetic consumption.
Results: In EOIPB group, median (Q1, Q3) tramadol consumption values for 24 hours (0 [0,50] mg) were found to be significantly lower than the control group (50 [50,100] mg) (median difference -50) (p<0.001). NRS values during rest and motion were lower in EOIPB group compared to the control group at all measurement points within 24 hours (p<0.05). The total QoR-15 scores were significantly higher in EOIPB group compared to the control group (p<0.001). No differences were detected in other secondary outcome parameters.
Conclusion: External oblique intercostal plane block resulted in less postoperative tramadol consumption. However, there were no minimal clinically important differences about postoperative opioid consumption. On the other hand, compared to multimodal analgesia addition of EOIPB improved overall QoR-15 scores at postoperative 24 hours.
Clinical Trial Reg. No.: NCT05536557
Pain following laparoscopic cholecystectomy (LC) is a common complaint that prolongs hospital stay and therefore increases morbidity.1 Most patients experience mild to moderate pain after LC. Previous studies have shown that analgesia is inadequate in 17-41% of patients following LC.2
In the 2018 update of the PROSPECT review, which explored evidence-based pain management following LC, the need for multimodal analgesia was emphasized and basic analgesic techniques were recommended.3 Effective fascial plane blocks have recently become popular as candidates to be a part of multimodal analgesia, especially for patients who require limited use of drugs in multimodal analgesia (such as active liver disease, liver failure, renal failure, platelet dysfunction, and peptic ulcer) or those with hypersensitivity to any of these drugs. As there are potential advantages such as a longer distance between the needle and neurovascular structures, less motor blockade and less hemodynamic change, fascial plane blocks can provide effective solutions to many difficulties faced by anesthesiologists in the perioperative period. Erector spinae plane block (ESPB), oblique subcostal transversus abdominis plane block (OSTAP), quadratus lumborum block (QLB), transversus abdominis plane (TAP) block, and serratus intercostal plane block (SIPB) are some of the fascial plane blocks used for postoperative analgesia in LC.4-6
External oblique intercostal plane block (EOIPB) is a novel block, which has been described as an important modification of the fascial plane blocks that can consistently involve the upper lateral abdominal walls.7,8 In comparison to QLB and ESPB, EOIPB has the benefit of being performed when the patient is supine. It also has an advantage over SIPB in that it produces greater analgesia throughout the midline of the abdomen.9 Many previous studies that have concentrated on the use of different TAP block strategies, including OSTAP, have shown that it could not sufficiently block the lateral cutaneous intercostal branches.10-12 Although previous case series have shown that EOIPB provides effective analgesia in LC, there is a lack of randomized studies in the literature.8,13
The hypothesis of this randomized study was that patients who underwent EOIPB would have less tramadol consumption in the postoperative period than patients who received routine multimodal analgesia alone. The study aimed to measure tramadol intake in the first 24 hours post-surgery. In addition, pain scores and quality of recovery were evaluated as secondary outcomes.
Methods
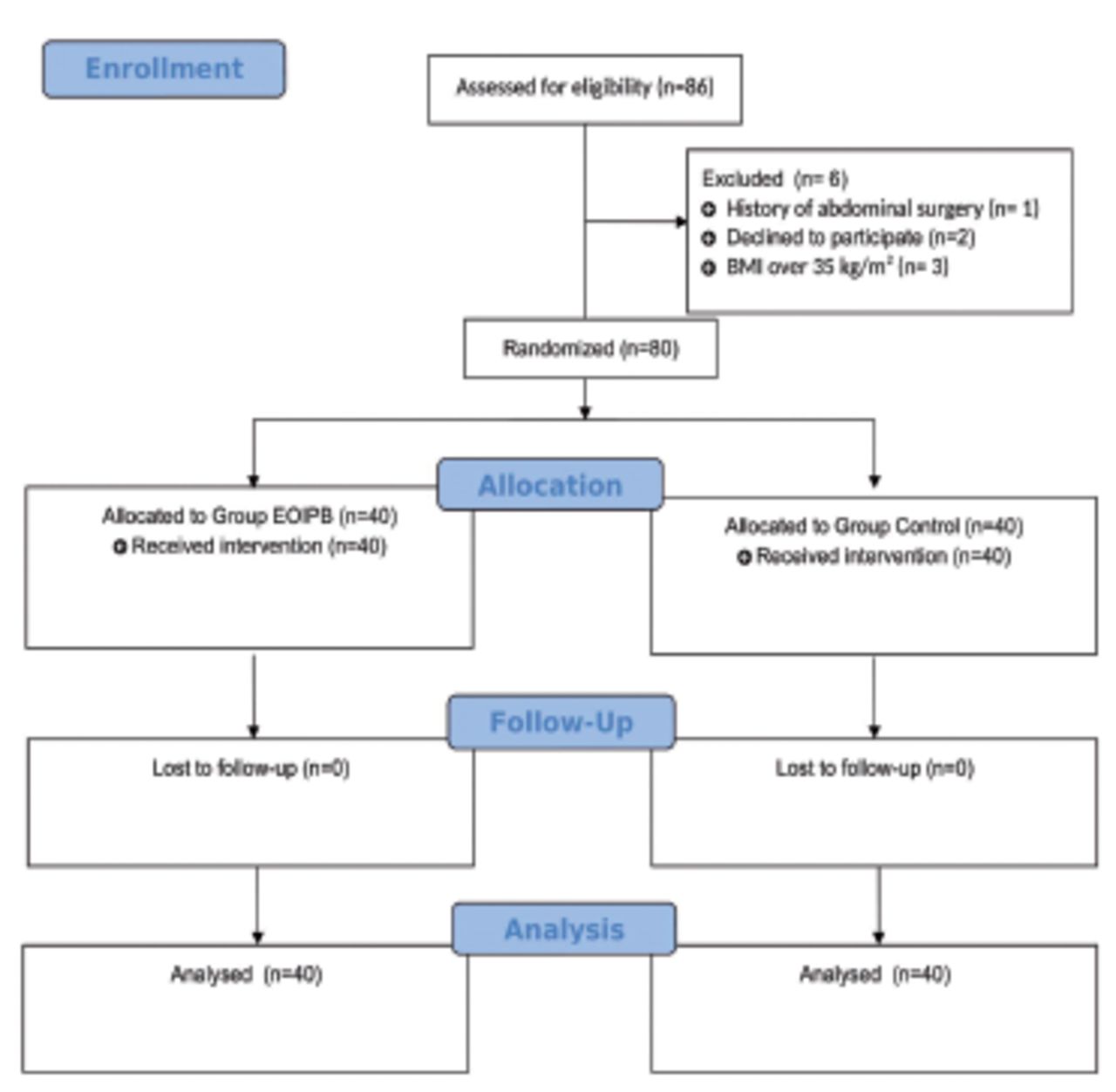
This study was carried out at Karaman Training and Research Hospital, Karaman, Turkey from September 15 to November 24, 2022. The Local Ethics Committee of Karamanoglu Mehmetbey University, Karaman, Turkey, approved the study (Ref No: 02-2022/11). All patients were recruited according to Declaration of Helsinki-2013 guiding principles. The flow diagram for the trial’s Consolidated Standards of Reporting Trials (CONSORT) is shown in Figure 1.

- CONSORT flow diagram of study.
The study enrolled patients between 18 and 70 who were scheduled to undergo elective LC and had an ASA Physical Status Classification of I-II. Study exclusion criteria included coagulation disorders, liver/kidney disease, abdominal surgery history, infection in the block application area, chronic opioid use, local anesthetic (LA) allergy, pregnancy, or BMI ≥35 kg/m2. Written and verbal consent was obtained from all patients.
The sample option in Minitab® (version 21,State Collage, PA: Minitab,Inc.) software was used for randomization. The results of the randomization were delivered to the anesthesiologists who were involved in the induction of anesthesia and the application of the block in the operating room in a sealed envelope. After the block had been performed, the patients were managed intraoperatively by a care provider blinded to the patient group by only entering the operating room after the patient was covered for the surgery.
Patients in the operating room were monitored using electrocardiography, oxygen saturation, capnography, and non-invasive blood pressure. For anesthesia induction, intravenous propofol 2 mg/kg, rocuronium bromide 0.6-1 mg/kg and fentanyl 1-2 µg/kg were used. Tracheal intubation was then performed approximately 2-3 minutes after anesthesia induction. Anesthesia was maintained using remifentanil infusion and sevoflurane at a concentration of 0.8-1 minimum alveolar. Remifentanil was administered at a rate of 0.01-0.2 µg/kg/min to maintain mean arterial pressure within 20% of baseline. Mechanical ventilation was conducted using volume-controlled mode with a tidal volume of 6-8 ml/kg, resulting in an end-tidal carbon dioxide pressure range of 35-40 mmHg. Tramadol 1 mg/kg was administered just before the remifentanil infusion was ended. Tracheal extubation was performed in patients with regular spontaneous breathing after residual neuromuscular blockade was antagonized. The interval between the start of anesthesia induction and tracheal extubation was defined as the “anesthesia time”.
External Oblique Intercostal Plane Block was administered by a single anesthetist following the intubation. Preblock preparation was performed before the block to decrease the time of block. A linear ultrasound transducer (2-14 MHz, Samsung RS85 Prestige, Seoul, Republic of Korea) was positioned in the sagittal plane at the 6th rib level, between the anterior axillary and midclavicular lines. The ribs, lungs, pleura, intercostal muscles, external oblique muscle and subcutaneous tissue were visualized in the image. The in-plane technique with a 22G, 80 mm block needle (Stimuplex B-Braun Medical, Melsungen, Germany) was used to inject 25 ml of 0.25% bupivacaine into the external oblique intercostal plane on both sides.8
The anterior rami of the T6-T12 nerves continue as intercostal nerves between the transversus abdominis and internal oblique muscles and give rise to lateral cutaneous branches that innervate the lateral abdominal wall and the midaxillary line at the junction of the serratus anterior muscle and the external oblique muscle.14 The lateral cutaneous branches at the midaxillary level can be blocked with a local anesthetic drug application to the external oblique intercostal plane between the anterior and midaxillary line at the sixth or seventh costa level. The linea semilunaris is the entry point for the thoracoabdominal nerves’ terminal anterior cutaneous branches into the rectus muscle sheath.15 The external oblique muscle fascia joins with others to create the anterior rectus sheath. By following this pathway, the LA reaches the rectus sheath and blocks the cutaneous branches of the associated intercostal nerves in the anterior region. This is the mechanism of pain reduction by which EOIPB blocks the lateral and anterior branches of T6-T10 intercostal nerves between the fascial layers.8
Surgery was performed with a standard 4-port surgical technique, and a pneumoperitoneum was created with unhumidified carbon dioxide (CO2) at an intra-abdominal pressure of 12 mm Hg. The surgeon inserted 4 trocars into the superior umbilicus, epigastric, mid-clavicular, and subcostal regions on the right side to prepare for LC.
For postoperative analgesia, all patients were given dexketoprofen (50 mg) twice a day and paracetamol (1 g) 4 times a day with equal intervals between doses. The first application of analgesic drugs was administered after anesthesia induction. The numerical rating scale (NRS) for the patient was assessed by a post anesthesia care unit (PACU) nurse in the PACU ward and a ward nurse in the general ward. Both nurses were blinded to group assignments. The NRS was questioned and recorded at 15, 30, and 60 minutes in PACU and at 2, 6, 12, and 24 hours in the general ward. When their Aldreth score was ≥9 and they completed the first one-hour NRS evaluation, patients were discharged from PACU. The patients were informed in the preoperative period on the NRS characteristics and the necessity to request analgesia when the NRS of pain at rest was ≥4. Intravenous tramadol (50 mg) was given when the patient’s pain level at rest was 4 or higher (≥4) on the NRS. If NRS of pain at rest was still ≥4 after 30 minutes, additional analgesia (tramadol 50 mg) was administered. If the patient continued to have complaints of pain, re-evaluation was continued. In the NRS evaluation, ‘0’ means no pain and ‘10’ indicates the worst pain possible.
Secondary outcomes for this study were postoperative Quality of Recovery score (QoR-15), NRS scores, sedation score, Postoperative nausea and vomiting (PONV) score, and antiemetic consumption at designated time points during the first postoperative 24 hours.
Quality of Recovery score-15 was evaluated with 15 parameters, which is accepted as an optimum scale for the patient-centered measurement of post-surgical recovery.16 The evaluation of QoR-15 took place 24 hours after the surgery. The QoR-15 is scored between 0-150, with 150 indicating an excellent improvement. Data collection was performed by a blinded investigator who was trained before the start of study; and QoR-15 was collected in the patients’ whose mother language were Turkish. A verbal descriptive scale of 0 to 4 was used to evaluate PONV (0: no nausea, 1: mild, 2: moderate, 3: vomiting once, 4: multiple vomiting episodes). A scale of 0-3 was used to evaluate the sedation score (0: awake, 1: sleepy but can be woken up easily by calling, 2: sleepy, 3: Can not be woken up by commands). The NRS, the sedation, and PONV scores were evaluated simultaneously. When the PONV score was ≥2, 10 mg of metoclopramide was administered.
The patient demographic characteristics were documented preoperatively, together with the postoperative time to stand up unaided, and the time to first oral intake following surgery. The first mobilization time was defined as the first time of standing up unaided in the general ward. The first oral intake time was defined as the time of first oral feeding. All the patients were encouraged for early mobilization and early feeding provided there was no nausea or vomiting after surgery. The decision to discharge was made by the surgeon if there is no clinical complaint. However, even if the discharge criteria of the general surgery clinic was achieved, discharge procedures were performed after the completion of 24-hour observation in our surgical clinic. As the block areas were covered with dressings in both the block and control groups, the patients and those who evaluated postoperative pain and secondary outcomes were blinded to the groups. Patients were also unaware of the group assignments.
Statistical analysis
A pilot study including 10 patients per group was carried out to determine the optimal sample size. The postoperative 24th-hour tramadol consumption was found to be 75±35.4 mg in the control group and 55±36.9 mg EOIPB group. These findings showed that there was approximately 30% difference in measures between the EOIPB and control groups. A 30% reduction in the postoperative 24th-hour scores was expected to provide statistical significance. According to the obtained scores, a sample size of 80 patients (40 per group) was calculated to provide 80% study power with α=0.05.
In the data analysis process, a variety of statistical methods were used to compare the EOIPB and control groups based on the measurements including tramadol consumption, NRS and QoR-15 scale scores. Statistical analyses were carried out using Minitab (Version 21.3.1, State College, PA: Minitab, Inc., 2022) and R-software (version 4.2.1, R Core Team, 2022). Statistical assumptions including the normality and the homogeneity of variances were checked with the Shapiro-Wilk/Kolmogrov-Smirnov and Levene tests, respectively. In addition, the existence of outliers were checked via Box plot and z-scores of each quantatitive variable. Based on the assumptions results, the Mann-Whitney U test or Independent Samples t-test was used to compare the EOIPB and control groups. To examine the association between categorical measurements, the Chi-square test was applied. Descriptive statistics were stated in the tables as frequency and percentage values for qualitative variables and as mean and standard deviation (SD) or median and Q1-Q3 values for quantitative variables. A statistical significance level of 5% was established.
Results
Out of the 86 eligible patients, after excluding 6 (BMI ≥35 kg/m2 n=3, declined to participate n=2, history of abdominal surgery n=1), the remaining 80 were randomly divided into 2 groups. The EOIPB procedure was completed all patients assigned to the block group underwent it successfully.
The descriptive statistics for qualitative and quantatitive variables are presented in Table 1 and showed no significant difference between EOIPB and control groups (p>0.05).
- Comparison of demographic data between groups.
The results of the comparison of the groups in terms of tramadol consumption are shown in Table 2. The median (Q1, Q3) tramadol consumption at 24 hours was significantly lower in EOIPB group (0 [0, 50] mg) than in control group (50 [50, 100] mg) (median difference -50) (p<0.001). No minimal clinically important differences (MCID) were observed between the 2 groups. (MCID 10 mg morphine or equivalent opioid), (10 mg morphine=100 mg tramadol).17,18
- Comparison of postoperative tramadol consumption.
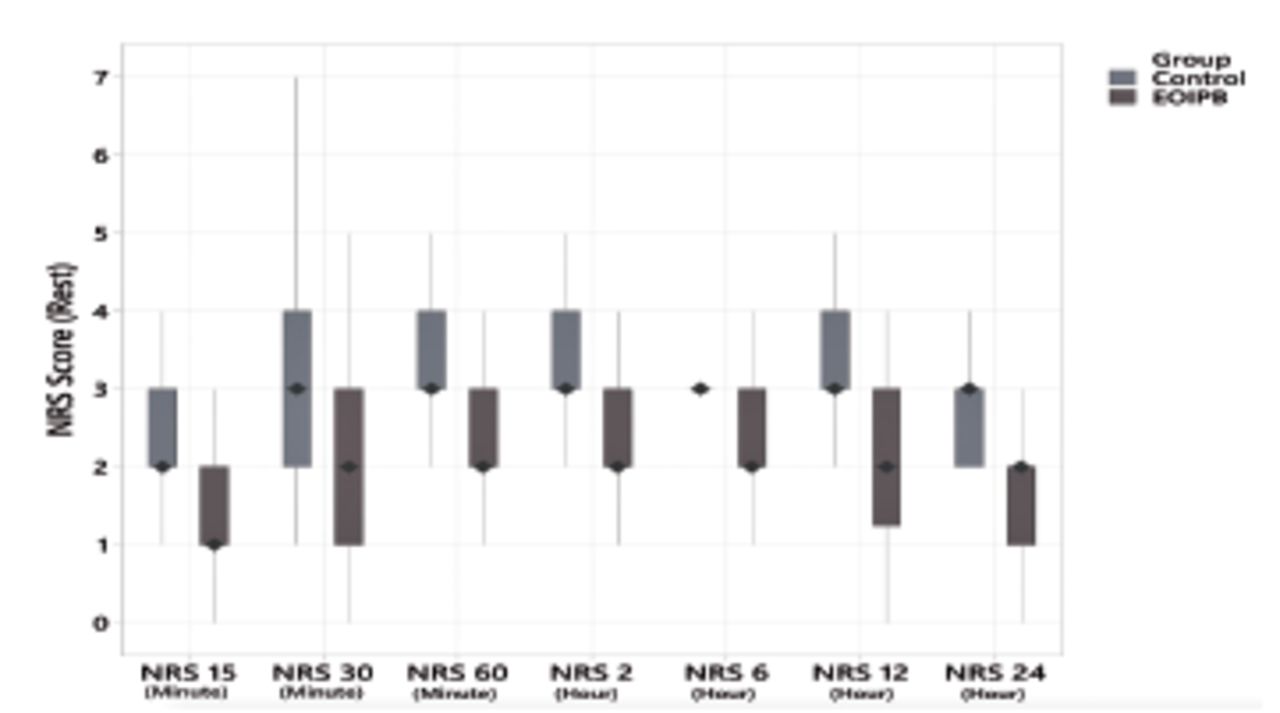
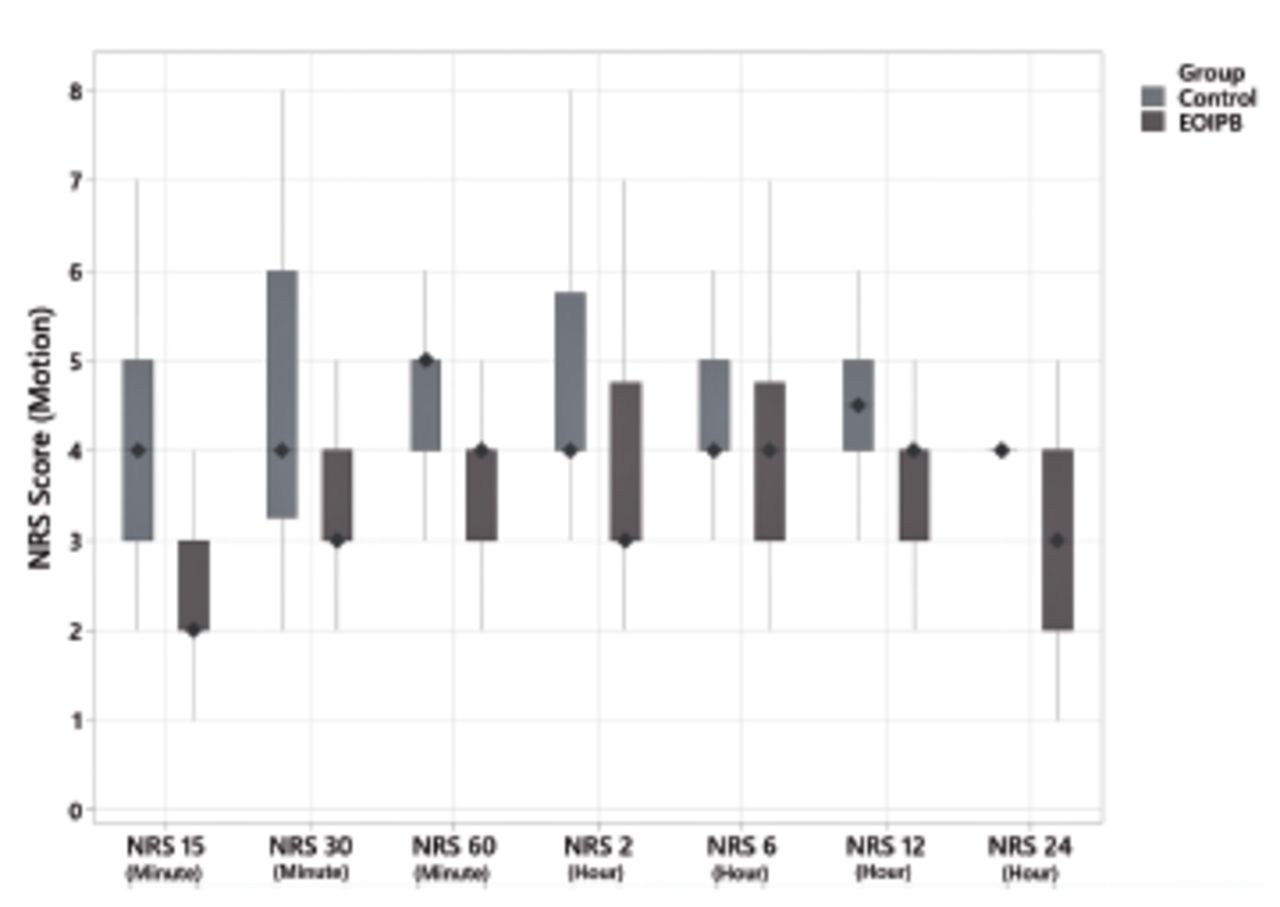
The NRS values in EOIPB group were statistically significantly lower from the 15th minute to the 24th hour, both during rest and motion, compared to the control group (p=0.019 during rest 6th hour, p=0.029 during motion 6th hour, p<0.001 at each other time point). Comparisons of the NRS scores at rest are given in Figure 2 and comparisons of the NRS scores with motion are shown in Figure 3.

- Comparison of numerical rating scale scores at rest.

- Comparison of numerical rating scale scores scores with motion.
The postoperative quality of recovery QoR-15 scores are presented in Table 3. The EOIPB group was determined to have significantly higher median (Q1, Q3) scores (137 [135, 139]) than control group (129.5 [126, 130.5]) (p<0.001).
- Comparison of postoperative QoR-15 scores between research groups.
Throughout all time points analyzed, both study groups’ sedation and PONV scores showed no significant difference (p>0.05). There was no variation in the groups in terms of consumption of metoclopramide.
Discussion
The study results showed that patients who underwent ultrasound-guided bilateral EOIPB following the induction of general anesthesia for postoperative analgesia after LC had lower tramadol consumption at postoperative 24 hours and at all other measurement times compared to the control group. Although tramadol usage in postoperatively was statistically significant at the specified intervals, it did not reach a level of minimal clinically important differences.17 The EOIPB was also determined to have further reduced NRS at all measurement points and resulted in higher QoR-15 scores.
As LC is considered minimally invasive, most patients experience mild to moderate postoperative pain. There are three basic sources of pain after LC, the incision site, local and systemic effects of pneumoperitoneum, and post cholecystectomy wound in the liver. The largest component of total pain originates from the incision site (50-70%), followed by pneumoperitoneum (20-30%) and cholecystectomy wound (10-20%)..19 Total abdominal pain following LC is a difficult and important issue to control. Multimodal analgesia is often the preferred method. Various regional anesthesia applications are widely used in multimodal analgesia. In this way, the use of postoperative analgesic drugs and their related side-effects are decreased.20,21 Regional anesthesia for LC should target the intercostal nerves T6 to T10 dermatomes innervating the upper abdominal wall for the relief of somatic pain occurring after LC.22
External oblique intercostal plane block has recently been described as a novel block for upper abdomen surgery.7,8 Hamilton and Manickam23 suggested in 2018 that administration of local anesthetic to the thoracic fascial area may result in blockade of the lateral cutaneous branches of the T7-T11 spinal nerves. Over time, Hamilton et al7 investigated drug diffusion after the external oblique fascial plane block with a cadaver study using dyes, strengthening this hypothesis. Elsharkawy et al8 (2021) presented EOIPB as a block providing upper midline and lateral abdominal wall analgesia. They demonstrated the probable mechanism of the block with the dyeing of both the anterior and lateral branches of the intercostal nerves T7-T10. This block also provides a dermatomal sensory block at the T6-T10 level in the anterior axillary region and the T6-T9 level in the midline.8 The 4 trocars used for LC are placed in the umbilicus, epigastric region, right lateral subcostal region, and right subcostal-midclavicular region under the xiphoidal process. The incision sites at the trocar entry points for LC are associated with T6 to T10 dermatomes.24 The EOIPB was preferred in the present study as it creates analgesia in the lateral and anterior abdominal walls between the T6 - T10 dermatomes, and is therefore aimed at the somatic component caused by the incisions at the entry sites of the trocars.
Following the definition of EOIPB, some case series with application of EOIPB for upper abdominal surgery were published. White and Ji13 performed EOIPB on 2 patients for upper abdominal surgery, and found that it included T7 - T11 dermatomes in the anterolateral plane. In another study, Coşarcan et al25 retrospectively compared patients who received various fascial blocks to patients without any block for bariatric surgery. In that study, EOIPB was applied to 15 patients using 30 ml 0.25% bupivacaine and it was reported that the TAP+RB (rectus sheath block), ESPB, and EOIPB that were used in the study all decreased morphine consumption, but the TAP+RB and EOIPB seemed to be the most effective blocks.25
Based on the findings of the current investigation, although tramadol consumption was statistically lower at postoperative 24 hours compared to the control group, it did not reach a level of minimal clinically important difference.17 Fascial plane blocks’ contribution to visceral analgesia is less effective than the somatic part.26 As with other fascial blocks, a limitation of EOIPB is the lack of visceral analgesic coverage, which suggests that the visceral component of post-LC pain may be the cause of EOIPB failure to achieve a minimal clinically important difference. Combining EOIPB with other regional anesthesia techniques that also block the visceral component of pain, such as paravertebral block (PVB) and ESPB, may further reduce postoperative analgesic use.27 Future studies may focus on the combination of regional anesthesia techniques where patients may need less additional analgesics.
Preemptive analgesia can prevent central sensitization by interrupting the transmission of harmful perioperative inputs to the spinal cord, resulting in decreased pain intensity and lower analgesic needs even after the analgesic effects of (preemptive) medications have worn off.28 The effectiveness of preemptive analgesia is measured by its ability to reduce postoperative pain.29 In this study, EOIPB had been applied before the incision to produce preemptive effect in order to reduce postoperative tramadol use and NRS scores. The lower NRS scores observed in the EOIPB group might be attributed to preemptive effect of this block also in the early period during rest and recreation beyond blocking nerve fibers related somatic pain.
The QoR-15 is a widely used, internationally validated patient-centered approach that assesses the general quality of recovery following a variety of surgeries.30 Developments in anesthetic drugs and techniques, and multimodal treatments for postoperative analgesia have led to patient-centered postoperative quality of recovery as an important endpoint. It is now more common for the patient to self-report the quality of recovery. As QoR-15 is accepted as an optimum scale for patient-centered measurement of post-surgical recovery, it was preferred in the present study. The fact that the QoR-15 total score and many sub-category scores were higher in the EOIPB group suggests that EOIPB accelerates recovery after LC.
Although low pain scores and opioid use are crucial signs of a successful block, it is just a partial predictor of how well a patient is recovering overall.31 According to the results of the present study, although tramadol consumption was statistically lower at postoperative 24 hours compared to the control group, it did not reach a level of minimal clinically important difference.17 However, EOIPB was seen to result in higher quality of recovery scores with a median difference of 8, which is higher than the reported minimal clinically important difference of the QoR-15 score.32
The appropriate LA concentration and volume has not yet been determined for application of EOIPB in LC. Cadaver studies have used a volume of 15 ml and a retrospective study used 30 ml (0.25%) bupivacaine for one side of the blockade.8,25 White and Ji13 placed catheters in the EOI plane and injected 20 ml of 0.2% ropivacaine and 40 ml of 0.5% ropivacaine. In the present study, 25 ml (0.25%) bupivacaine was used for each side. There is a clear need for further comprehensive studies to determine the most effective drug concentration and volume in EOIPB block for LC.
The EOIPB application may cause vascular injury, hematoma, and LA toxicity. In addition, complications such as pneumothorax may occur because of the proximity to the lungs.33 In this study, no complications related to the block occurred. The American Society of Regional Anesthesia and Pain Medicine (ASRA) guidelines do not recommend the use of central nerve blocks and deep nerve plexus blocks in patients using anticoagulant agents. However, the application blocks to superficial nerve plexus and peripheral nerves is recommended. Since the area where these blocks are applied is lack of vascularity and convenient to compression.34 The EOIPB is a superficial block and there are no big vessels in the application area of the block. However, there was no patients with coagulation disorders in this cohort, Therefore, until this recommendation was a subject of another study recruiting patients with coagulation disorders, EOIPB should not be offered in this patient population.
Study limitations
First, the sample size was based on postoperative tramadol consumption and may not have been sufficient for the NRS, PONV, or sedation scores. A second limitation was that recommended local anesthetic doses and volumes for EOIPB have not yet been identified. Therefore, 25 ml (0.25%) bupivacaine was used per side. Thirdly, cold sensation and pinprick tests for determination of affected dermatomes were not performed because they would have disrupted the blinding process. As a result, EOIPB may have failed in some patients.
In conclusion, EOIPB resulted in less postoperative tramadol consumption following LC, although not to a level of minimal clinically important difference. The EOIPB was also seen to result in lower NRS scores of pain within postoperative 24 hours. Better overall quality of recovery on the QoR-15 scale was obtained with EOIPB compared to without EOIPB. Therefore, EOIPB may be effective as a multifaceted analgesic method in LC when multimodal analgesics are not possible, as ultrasound-guided EOIPB is easy and safe to apply with no reported side-effects or complications. Nevertheless, there is a need for further studies to investigate the effectiveness of EOIPB in different upper abdominal surgeries and to compare it with other fascial blocks in LC.
Acknowledgment
We thank to operating room staff for helpfull and support in Karaman Training and Research Hospital. We would like to thank Caroline J. Walker for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 12, 2023.
- Accepted September 12, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.