


Abstract
Objectives: To describe the increasing number of gastric cancer cases at Bahrain Defense Force Hospital with implementation of immunohistochemistry markers as prognostic factors.
Methods: This study included histologically confirmed malignant gastric tumors diagnosed at Bahrain Defense Force Hospital from January 2009 to June 2019. Various epidemiological and pathological data were abstracted and recorded with immunohistochemical analysis of the proliferation marker Ki67 and cell-cycle regulator p53 as prognostic factors.
Results: A total of 53 patients with gastric cancer were included in the study, with mean age of 59.75 ± 12.9 years. The typical histological types were signet ring cell adenocarcinoma (68%) and intestinal type adenocarcinoma (17%). Helicobacter pylori and intestinal metaplasia were significantly associated with gastric cancer (p<0.01). The studied population’s mortality was 39 (74%). The Ki67 proliferation index showed a mean and standard deviation of 67.09 ± 16.338, with a higher mortality rate in patients with low Ki67 but no difference in survival time. No statistically significant association was found between clinicopathological findings with p53 immunostaining positivity.
Conclusion: The common gastric cancers are signet ring cell adenocarcinoma and intestinal type adenocarcinoma, affecting a wide range of age groups (33-91 years), with those over 60 years at greater risk. Interestingly, low Ki67 is associated with a higher mortality rate, whereas p53 has no prognostic significance. Expression of both Ki67 and p53 showed no association with survival time.
Gastric cancer is one of the most common cancers globally (ranked 5th), with a high mortality rate.1 According to the World Health Organization report in 2020, gastric cancer globally accounted for 770,000 deaths. It represents one of the leading causes of death worldwide,and it is the fourth most common cause of cancer-related deaths worldwide and has a dismal prognosis, with an average 5-year survival rate of less than 20%.1-3
Gastric cancer incidence has a wide geographical variation globally, with the lowest rates reported in North America and Northern Europe and the highest in Asian countries.4 Over 70% of new gastric malignancy cases are reported in developing countries. Approximately half of these cases are in East Asia, in which China is the most influenced country, accounting for 42.6% of the worldwide incidence and 45% of all gastric cancer-related deaths.5,6 The incidence of gastric cancer in Bahrain from 2009 to 2018 was 89 in males and 75 in females.7 The age standardized rate is 3.9 in males and 3.0 in females. It is the 9th in the order of malignancies among both genders.7

- Frequency of total number of diagnoses per year from 2009-2019.

- Mortality rates according to demographics, clinical findings, and diagnoses.

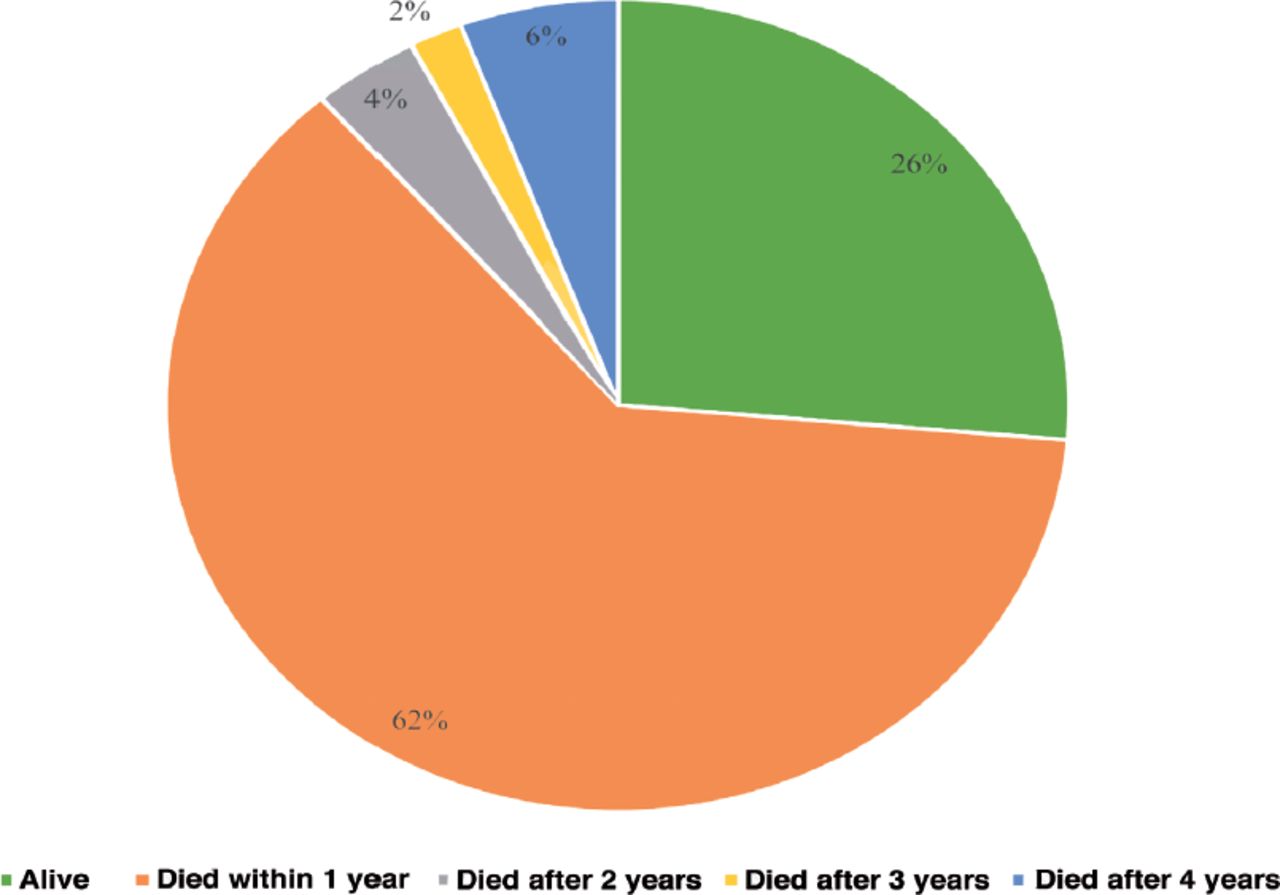
- Mortality and death after diagnosis.
Primary prevention plays an important role in reducing the incidence of gastric cancer mainly by early detection with an effective screening program and having a healthy diet by avoiding precancerous food and consuming fresh fruits and vegetables.8-11 A multidisciplinary approach for the treatment of gastric cancer is mandatory.12
Helicobacter pylori (H. pylori) infection presents a major risk in predisposition to gastric cancer.13 Genetic predisposition is a significant risk factor. Regeneration gene 3 (reg3) is expressed in gastric mucosa tissues with H. pylori.14 Various gastric cancer biomarkers facilitating early detection and promising for better outcomes of gastric cancer have been identified through experimental research.15-17
Previous reports in Bahrain indicated that adenocarcinoma is the most common type of gastric cancer. Omran and Ansari2 showed that the incidence of histologically confirmed stomach cancer in Bahrain, derived from the study figures of 116 cases of gastric cancer out of a population of 1 million over 7 years, is 1.7/100,000/year.
Although gastric cancer incidence has decreased globally, we have noticed an increase in cases diagnosed with gastric cancer in our institute, especially the signet ring cell adenocarcinoma (SRCC), over the last years. This study aimed to describe the increasing incidence of gastric cancer and its association with clinical factors and outcomes among patients diagnosed with gastric cancer in at Bahrain Defense Force (BDF) Hospital covering the period from January 2009 to June 2019, along with the implications of Ki67 and p53 immunohistochemical studies as prognostic indicators.
Methods
This study included all histologically confirmed malignant gastric tumors diagnosed at BDF Hospital from January 2009 to June 2019. All cases of gastric cancer were identified by a computer search engine. All cases were reviewed by 2 histopathology consultants (A.D. and M.A.). Patients’ mortality data were retrieved from the national death registry office. The data were collected using a coded master sheet in Excel form MS 2019. The ethical clearance obtained from the research and ethical committee of the BDF Royal Medical Services received hospital acceptance (no. BDF/R&REC/2022-660).
Immunohistochemistry
Sections from 2 representative paraffin blocks of each case were immunostained with p53 (mouse monoclonal antibody, clone DO-1, (Bp53-11) by Ventana) and Ki-67 (mouse monoclonal antibody, clone MIB1, [30-9] by Ventana). Ki-67 expression was defined as the presence of nuclear staining with the following criteria: <25% = very low, 25%-50% = low, 51%-75% = moderate, and >75% = high.18
P53 mutation status was defined as positive in the presence of nuclear staining with the following criteria: negative = cytoplasmic staining, focal positive = unequivocal staining in 10%-50% of tumor cells, diffuse positive = >50% of the tumor cells were positive.19
Statistical analysis
Continuous variables were represented as mean ± standard deviation (SD), whereas categorical variables were represented as frequencies and percentages. Fisher’s exact test was used to assess associations between categorical variables. The SPSS, version 26 (IBMCorp, Armonk, NY, USA) software was used to conduct all analyses. A p value of <0.05 was considered statistically significant.
Results
A total of 53 patients were diagnosed with gastric cancer during this study period; of those, 28 (53%) were females and 25 (47%) were males. The common histological types reported were SRCC (36/53, 68%), intestinal type adenocarcinoma (9/53, 17%), diffuse large B-cell lymphoma (5/53, 9%), high-grade MALToma (1/53, 2%), and high-grade gastrointestinal stromal tumor (2/53, 4%). Adenocarcinoma represented 45/53 (85%) of all types of gastric cancer in general among the studied population (Figure 1).
The highest prevalence of gastric cancer (9 cases in total) was recorded in 2013, with SRCC accounting for 8 of those cases and diffuse large B-cell lymphoma for 1 case. With a total of 7 patients, 2019 was the year with the second highest number of reports of gastric cancer diagnosis, with 3 cases of intestinal type adenocarcinoma, 2 cases of SRCC, and 2 cases of diffuse large B-cell lymphoma.
The frequencies and associations of demographics and clinical findings with the diagnosis of gastric cancer are presented in Table 1.
The youngest patient was 33 years old, and the eldest was 91, with a mean age of 59.75 ± 12.9. The most common age group was over 60 years old, with 26/53 (50%) of reported cases. This age group’s common type was SRCC, which constituted 50% (18/36) of the total number of cases diagnosed with SRCC.
Helicobacter pylori, intestinal metaplasia, and patient mortality rate showed a significant association with the diagnosis of gastric cancer, as shown in Table 1. H. pylori was found in patients with intestinal type adenocarcinoma (78%), SRCC (8%), and MALToma (100%). Both intestinal type adenocarcinoma (56%) and SRCC (8%) diagnoses were found to have intestinal metaplasia.
- Frequencies and associations of demographics and clinical findings with the diagnosis of gastric cancer.
Signet ring cell adenocarcinoma and intestinal type adenocarcinoma both had high mortality rates (80% and 78%). Patients who underwent chemotherapy or surgery showed a better survival rate compared with patients who did not receive any treatment. The mortality rates according to demographics, clinical findings, and diagnoses are illustrated in Figure 2. Of the 39 died patients, 24 were females (60%), and 15 were males (40%). A high mortality rate was reported for SRCC, with a total of 29 of 39 total deaths (75%) and 7 survivors. Diffuse large B-cell lymphoma had a better prognosis, with 1 dead patient and 4 survivors. Following diagnosis, 18 patients underwent surgery; 8 of them passed away, and the remaining 10 are still alive, as shown in Figure 2.
The highest number of deaths occurred in the first year after diagnosis, with a total of 33 patients, followed by 2 deaths after 2 years, 1 death after 3 years, and 3 deaths 4 years after diagnosis, as shown in Figure 3.
The Ki67 proliferation index showed a mean and SD of 67.09±16.338, ranging from 15 (lowest) to 90 (highest). The mortality rate was found to be statistically significantly associated with Ki67, as illustrated in Table 2. All patients with low Ki67 proliferation, 90.5% with moderate Ki67, and 50% of patients with high proliferation died. Diffuse large B-cell lymphoma showed a statistically significant association with Ki67 staining, with all patients (5 in total) having a high proliferation (>75%). No statistically significant association was found between demographics, clinical findings, and diagnosis and P53 immunostaining, as illustrated in Table 3.
- Frequencies and associations of demographics, clinical findings, and diagnosis with immunostaining (Ki67).
- Frequencies and associations of demographics, clinical findings, and diagnosis with p53-immunostain.
Two patients had diffuse positive p53 with high Ki67 immunostaining, and 76% of patients with moderate Ki67 had focal positive p53 immunostaining.
The median survival time for negative and weak positive p53 was 13.3 and 13 months, whereas for strong positive p53, it was a median of 26.2 months, with only 2 patients. Hence, there was no statistically significant correlation between survival time and p53 expression.
The median survival time for low and moderate Ki67 was 11.6 and 13 months, whereas high Ki67 had a median survival time of 26.2 months. No statistically significant correlation was found between survival time and Ki67 expression.
Discussion
In this study, most cases were diagnosed as adenocarcinoma (85%). This finding was similar to a previous report by Omran and Ansari2 at our center 10 years ago, and the finding is correlated with the currently available literature.13,14,20 There were complex factors related to gastric cancer based on the social determinants of health and environmental and nutritional factors. A better understanding of these relationships can help researchers determine the most effective intervention strategies for reducing the risk of this disease. In Bahrain, health and research centers work together to understand health promotion and control the condition with a promising outcome.
During the study period, deaths were reported in 39 cases of gastric cancer for various causes due to health status deterioration. The most aggressive type is SRCC, which was significantly associated with mortality in 29 out of 39 deaths. The literature confirmed that gastric cancer is one of the most common causes of cancer-related mortality worldwide.1 The SRCC can be presented in sporadic and familial settings. Mutations in the CDH1 (E-cadherin) gene are most commonly identified. The CDH1 gene is a tumor suppressor gene and is located on chromosome 16q22. Heredetary diffuse gastric cancer (HDGC) is an autosomal dominant disorder with approximately 40% of HDGC families have germline mutations in the CDH1 gene and the cumulative risk of GC for CDH1 mutation carriers by the age of 80 years is reported to be 70% for men and 56% for women.21
The current findings examine the biological, clinical, and environmental factors that influence the rate of this disease.22 Based on this study’s findings, we recommend applying different intervention methods that could increase the awareness of gastric cancer and increase screening in efforts to reduce the risk of gastric cancer. In our study, over 50% of patients had abdominal pain or anemia, which should prompt the clinician to conduct further investigations, mainly endoscopy. The majority of cases are sporadic subtypes that are strongly associated with environmental risk factor.23 Therefore, modification of environmental factors together with lifestyle is of great benefit. H. pylori is a strong risk factor, especially in intestinal type adenocarcinoma. It was reported in 11 cases, mainly with the intestinal type. Addressing the risk factors in a separate program will lead to overall community health. The association between gastric cancer and H. pylori is well established in many regions worldwide, including Korea, China, Iran, and Austria. Other potential risk factors include occupational risk factors, water supply, and food.24 Many risk factors of gastric cancer have been identified worldwide: diet, lifestyle, infections, and sociodemographic characteristics.25-28 These risk factors are complex and interact with other environmental factors to represent significant hazards in most populations.
Ki67 present during all active phases of the cell cycle (G1, S, G2, and M), but is absent in resting cells (G0). Ki67 expression is associated with tumor cell proliferation and growth, and is widely used in pathological assessments as a proliferation marker. The nuclear protein Ki67 (pKi67) has prognostic and predictive values in many types of cancer. Clinically, pKi67 has been associated with metastasis and tumor stage. Moreover, it has been shown that Ki67 expression is significantly higher in malignant tumors with poorly differentiated component, as compared with normal tissue. Its predictive role in that pKi67 expression determines patients who are more likely to respond to a given therapy. The Ki67 labeling index is an independent prognostic factor for survival rate, which includes all stages and grade categories.18
In some studies, Ki67 showed limited clinicopathologic and prognostic value in gastric cancer, whereas in others, it showed a correlation with poor prognosis.18,29-31
The p53 gene is a tumor suppressor gene that monitors genomic integrity and cellular homeostasis. P53 is a nuclear transcription factor with a pro-apoptotic function located on the short arm of chromosome 17. Activated p53 promotes cell cycle arrest to allow deoxyribonucleic acid (DNA) repair or apoptosis to prevent the propagation of cells with serious DNA damage. Mutant p53 has oncogenic potential. P53 mutation was found to be associated with worse outcome in some tumors.33
As for Ki67, for p53, the significance of positivity in gastric cancer is controversial. Jovanović et al32 showed no prognostic significance of p53 positivity. Al-Moundhri et al33 showed that p53 expression was associated with poor overall survival. Finally, Sanaat et al34 showed that p53 positivity was significantly associated with improved survival. In our study, the Ki67 proliferation marker was associated with mortality rate; interestingly, patients with low Ki67 had a high mortality rate (all were diagnosed with SRCC) compared with patients with high ki67 (Table 2), which could be attributed to other factors, such as tumor type, stage, completeness of excision, and coexistence of other comorbidities. P53 positivity showed no significant association with demographic data or mortality rate (Table 3). Expression of Ki67 and p53 was not associated with differences in survival time.
For the use of diagnostic biomarkers that can facilitate the early detection of gastric cancer, many ongoing studies have identified oncogenes and tumor suppressor genes, especially microRNAs (miRNAs), as novel gastric cancer biomarker.35 Despite its decreasing incidence, gastric cancer remains one of the world’s leading cancers and a significant global health problem due to its overall high prevalence and high mortality rate. Gastric cancer is still an important health problem, with several aspects that remain significant challenges.
Study limitations
One of the limitations of this study was the unavailability of the TNM staging system in some of the cases, as the patients were transferred to the oncology center for further management. However, other patients preferred to travel overseas for management, others refused any further treatment, and a few died before initiation of the treatment plan. Missing paraffin blocks in some of the cases was another obstacle, especially when taken by patients for other opinions. Some of the data were not available and kept as “unknown” as they were not mentioned in the patients’ data or the patients were lost to follow-up or treated outside our institution. Another limitation of our study is that it was a single-center project with a small number of patients.
In conclusion, the common gastric cancers are SRCC and intestinal type adenocarcinoma, both of which had high mortality rates (80% and 78%). However, gastric cancer affected a wide range of age groups (33-91 years), with those over 60 years old at greater risk. The main warning signs at presentation among gastric cancer patients were abdominal pain and anemia. Older patients with the mentioned warning signs should be carefully screened to facilitate early detection and management. The mortality rate is higher in patients with low Ki67 proliferation, which could be attributed to other factors, such as the comorbidities, tumor type, and stage. Ki67 and p53 expression showed no significant association with survival time.
Acknowledgment
Thanks are extended to our colleagues at BDF Hospital. Special thanks to the histopathology department for technical support and Crown Prince Center for statistical analysis support. The author also would like to than SCRIBENDI (www.scribendi.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 6, 2023.
- Accepted November 5, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.