


Abstract
Objectives: To determine the overall effect size, identify the study with the strongest effect size, and examine the age group with the strongest relationships between the variables.
Methods: In this study, a meta-analytical analysis was carried out by bringing together 13 studies from around the world examining the statistical relationships between cardiothoracic ratio (CTR) and left ventricular ejection fraction (LVEF). Thus, it is hoped that the results will contribute to studies on the relationships between CTR and LVEF and bring a holistic view to these relationships. To determine CTR, studies were identified through a review of the literature, and those that reported a correlation between the variables under investigation were included in the analysis process. The date range of this study 01.11.2022-15.01.2023.
Results: According to the findings, when all the results were analysed together, the mean effect size for CTR and LVEF correlation was found to be r=-0.12. When all studies were considered separately, generally small negative correlations were observed between CTR and LVEF. It is possible to say that there is no publication bias in the studies.
Conclusion: This study is a meta-analytic study combining 13 studies examining the statistical relationships between CTR and LVEF. The results of this study are expected to make a valuable contribution to the field of research on the relationship between CTR and LVEF, providing a more comprehensive understanding of these associations.
PROSPERO Reg. No.: 392207
The evaluation of heart size is an important parameter in determining the efficacy of the identification, diagnosis and treatment of various heart diseases.1 Significant changes in heart size can occur in many heart diseases such as cardiac enlargement, pericardial inflammation and effusions, cardiogenic pulmonary oedema, cardiac calcification, heart failure, valvular heart diseases, cardiomegaly and congenital cardiac anomalies.1,3 Changes in heart size can be used to monitor the severity and determine the degree of these diseases.3
Heart size can be measured using various medical imaging techniques, including chest radiography (CR), angiography, echocardiography, radionuclide imaging, computed tomography (CT), and magnetic resonance imaging (MRI).4,5 However, CR is widely used in the diagnosis and follow-up evaluation of almost all heart diseases because it is cheaper than other imaging methods and can be easily found in all clinical settings.1,6-8
Congenital or acquired congestive heart failure (CHF) is a clinical condition with a poor prognosis resulting from the inability of the heart to pump blood to the periphery to meet the metabolic needs of the tissues.9 Measurement of left ventricular ejection fraction (EF) is a valuable prognostic indicator for patients with congestive heart failure (CHF).3,6,7
Left ventricular ejection fraction (LVEF) is used to evaluate the global systolic function of the left ventricle. Left ventricular (LV) contractile function indicators, such as EF and LV size, contribute significantly to the identification, diagnosis and treatment of congestive heart failure patients.5-15 Left ventricular size is frequently used to evaluate the morbidity and mortality of cardiovascular diseases.16,17 It has been reported that EF is inversely proportional to the mortality rate.13,18 Although EF can be easily measured by various imaging techniques such as angiographic, radionuclide or echocardiographic imaging techniques, these techniques are quite expensive and may not be readily available in all clinics.15 For this reason, it is important to develop simpler, cheaper and non-invasive methods for EF measurement.3
Cardiothoracic ratio (CTR) is a simple, inexpensive and useful index for estimating heart size.19 It is the most commonly used method for detecting cardiomegaly on digital chest radiographs.20 It continues to be used routinely in clinical practice.3,15 Cardiothoracic ratio is calculated by dividing the maximum transversal diameter of the heart by the largest internal (internal diameter) diameter in the chest cavity.19,21 Normal values for this measurement range from 0.42 to 0.50. A value above 0.50 is considered abnormal and may indicate cardiomegaly.22,23
Therefore, medical imaging methods such as angiography, echocardiography, radionuclide imaging, CT, and magnetic resonance imaging can be used to easily obtain measurements such as heart size, CTR, and LVEF. These values have important prognostic value in terms of the identification, diagnosis and follow-up of various heart diseases.4,5,24-27
In this study, the statistical relationships between CTR and LVEF were examined. A meta-analytical analysis was carried out by bringing together 13 studies carried out worldwide and examining these relationships. This study is expected to contribute to the literature by determining the overall effect size, which study has the stronger effect size and in which age group the relationships between the variables are stronger. Thus, it is hoped that these results will contribute to studies on the relationships between CTR and LVEF and bring a holistic view to these relationships.
Methods
Determination of which studies to include in the meta-analysis
This study is meta-analytic in nature. Within the scope of the research, there were studies in which the relationships between CTR and LVEF variables were reported. The date range of this study was between November 2022 and January 2023. In the process of determining which studies to include in the meta-analysis, databases and internet search engines such as PubMed, Europe PMC, SCOPUS, Medline, Web of Science Core Collection, Google Scholar, and ULAKBİM were used. The keywords ‘cardiothoracic ratio and left ventricular ejection fraction’, ‘CTR and LVEF correlation’ and ‘CTR and LVEF’ were used in Turkish and English to find the studies. The criterion for including the obtained studies in the study was as follows: Studies that reported the correlation coefficient and sample size between the CTR’ and ‘LVEF’ variables were included. In terms of the reliability of the study findings, studies carried out with special groups (such as studies with different other cardiological disease groups) were excluded (Figure 1). It is common to use a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram to provide a visual summary of the study selection process. The PRISMA diagram includes the number of studies identified from the initial database search, the number of studies screened, the number of studies excluded based on eligibility criteria, and the number of studies included in the final analysis. This helps readers understand the study selection process and assess the potential for selection bias.

-Preferred reporting items for systematic reviews and meta-analyses diagram.
In this particular study, a PRISMA diagram was used to present the selection process for studies to be included in the systematic review and meta-analysis. The diagram showed the number of studies identified through database searches, the number of studies screened, the number of studies excluded based on eligibility criteria, and the number of studies included in the final analysis. The list of studies examined within the scope of the research was also presented in Table 1.
-Studies included in meta-analysis.
General characteristics of studies included in the meta-analysis
This analysis encompassed data from a total of 13 studies, utilizing a random effects model to synthesize the findings. The sample sizes of the study groups included in the studies ranged from 30 to 7476. The total number of participants is 9911. Studies were published between 1998 and 2021. The number of studies was determined by years as 1998 (1), 2000 (1), 2002 (1), 2004 (1), 2012 (2), 2013(1), 2014 (2), 2017 (1), 2019 (1), 2020 (1), 2021 (1), respectively. All of the studies included in this research consist of articles published in journals. In most studies included in the meta-analysis, the average age of the participants was not specified. The sample of studies included in the meta-analysis consisted of patients with heart conditions (Table 1 & Figure 1).
Analysis of data
The correlation coefficient was reported in all research results within the scope of the study. In meta-analysis studies, direct correlation coefficients are not used. Instead, correlation values reported in the studies are converted to Fisher’s z-values, and the analyses are performed on these values. The meta-analysis findings are then reported, and the values are converted back into correlation coefficients.37,38 The same method was employed in this study. Cohen39 (1992) categorized effect sizes of correlation coefficients into 5 groups: weak (between 0.00 and ±0.10), small (between 0.10 and ±0.30), moderate (between 0.30 and ±0.50), strong (between 0.50 and ±0.80), and very strong (>0.80).This classification was adopted in this study. The data analysis was carried out using Jamovi (version. 2.2).
There is a statement suggesting that studies reporting higher effect sizes are more likely to be published than those reporting lower effect sizes.37 The finding obtained in this study is in the opposite direction of what was expected.
-Result of the classic fail-safe N (detection of publication bias). Publication Bias Assessment (publication bias).
-Random-effects model (k=13).
The present study employed the error-safe N calculation using the Rosenthal approach analysis. Comparing published and unpublished studies is also covered in the scope of publication bias and sensitivity. Accordingly, it was determined that the findings regarding the relationships between CTR and LVEF would be invalidated if there were 307 more unpublished studies with non-significant findings.
The study used correlation coefficients and Fisher’s z-values for meta-analysis, and the effect sizes were classified using Cohen’s classification. The classic fail-safe N analysis was used to assess publication bias, and the results indicate that the findings regarding the relationships between CTR and LVEF would be invalidated if there were 307 more unpublished studies with non-significant findings. The “Begg and Mazumdar” rank correlation and Egger’s regression tests did not indicate any significant publication bias, and the trim and fill number of studies suggests that no studies were added to the analysis after applying the trim and fill method.
Results
The overall effect sizes of the studies included in the study were first calculated with 2 methods. The first was to analyze all of the correlation values reported in all studies, and the other was to analyze the results by averaging these results in studies that reported more than one result. When all results were analyzed together, the mean effect size for CTR and LVEF correlation was found to be r=-0.12. According to the classification of Cohen,it can be said that this effect size is small in the negative direction.39
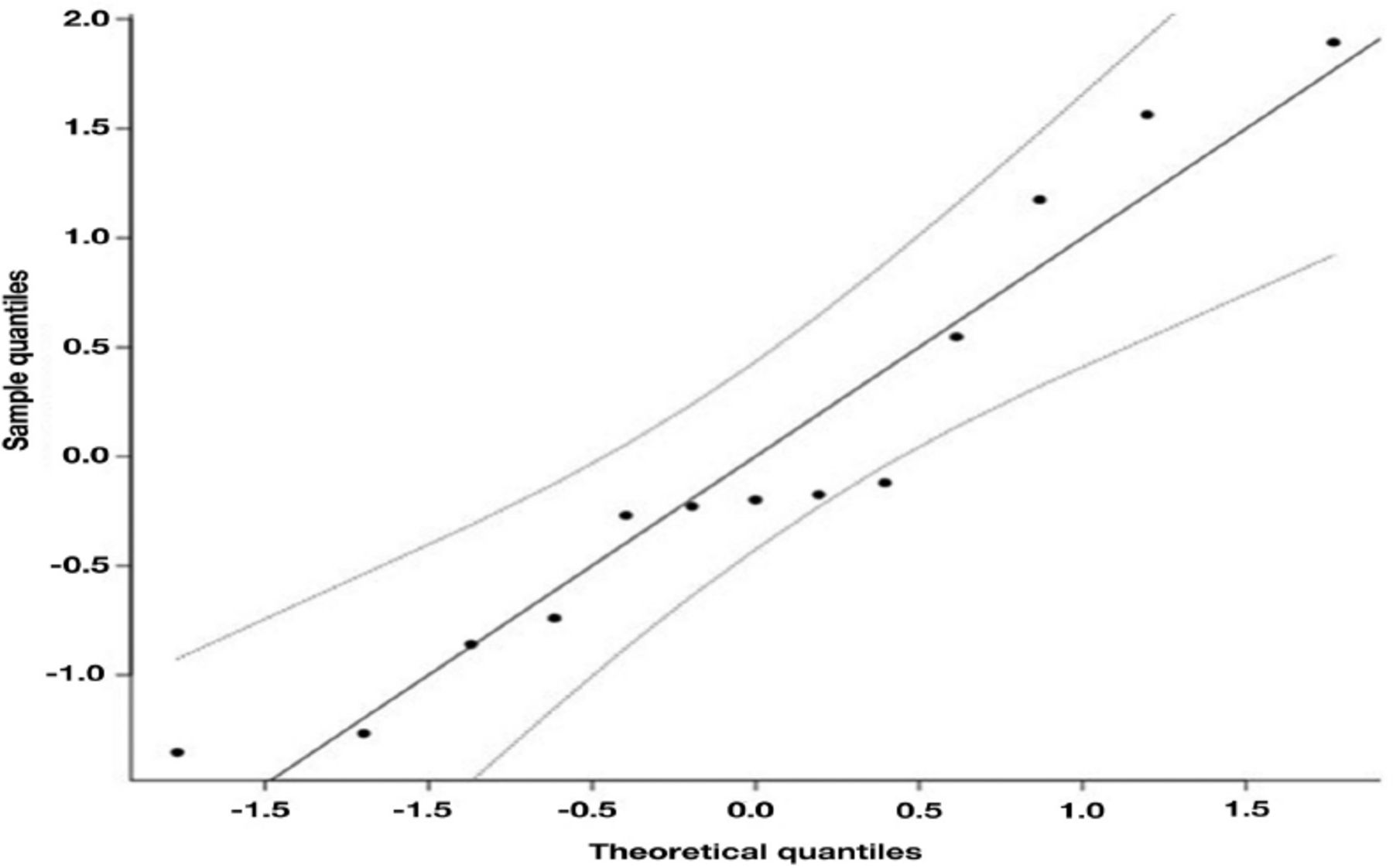
Observing whether the data points are dispersed evenly around a straight line, it was concluded that the distribution of the dataset follows a Weibull distribution with a shape parameter of 2 (Figure 3). Figure 3 in this study represents the Q-Q Plot, which stands for quantile-quantile plot. The x-axis of the Q-Q Plot shows the quantiles of the theoretical distribution, while the y-axis represents the quantiles of the sample data. As the points on the graph are closer to the line of equality, it indicates that the 2 datasets have a similar distribution.

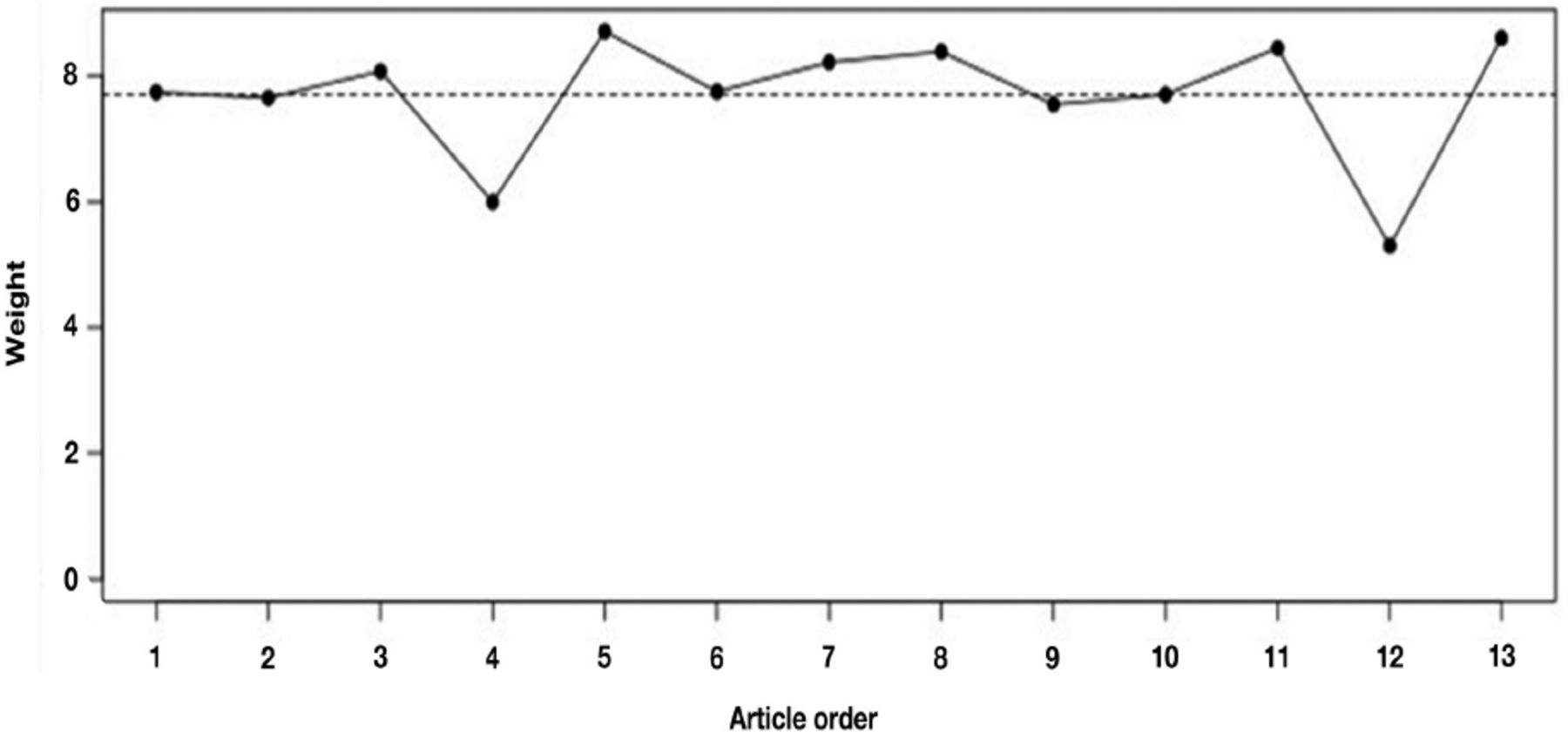
-Identification of impactful observations and effective case diagnosis (weights).

-Quantile-quantile plot of residuals for normality assessment.
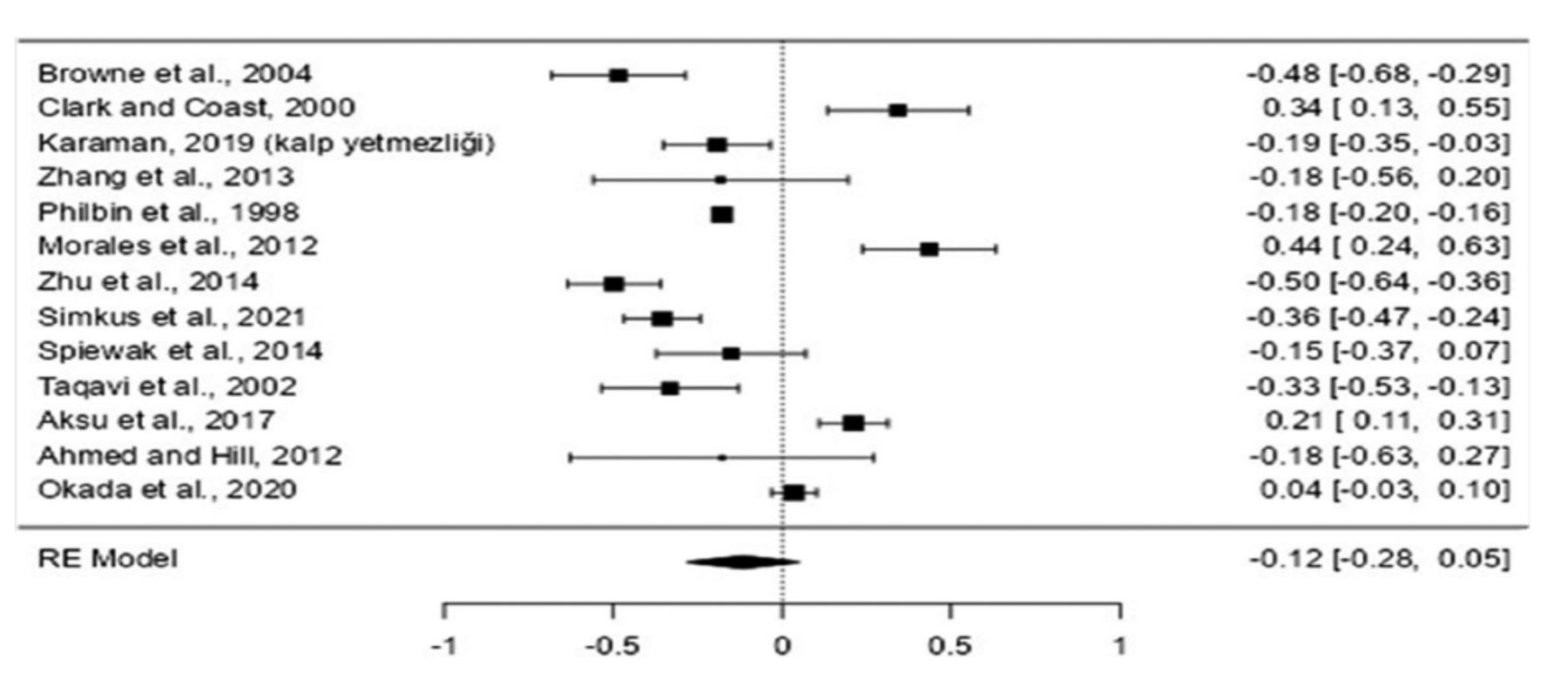
The investigation was carried out utilizing the Fisher r-to-z changed connection coefficient as the result measure. An irregular impacts model was fitted to the information. How much heterogeneity (such as tau²), was assessed utilizing the limited most extreme probability estimator40,41 notwithstanding the gauge of tau², the Q-test for heterogeneity (Cochran,42 1954)and the I² measurement are accounted for. In the event that any measure of heterogeneity is identified (such as tau²>0, no matter what the consequences of the Q-test), an expectation stretch for the genuine results is likewise given. Studentized residuals and Cook’s distances are utilized to analyze whether studies might be anomalies and additionally persuasive with regards to the model. Studies with a studentized lingering bigger than the 100x(1-0.05/(2Xk))th percentile of a standard ordinary circulation are viewed as possible exceptions (such as utilizing a Bonferroni remedy with 2-sided alpha =0.05 for k examinations remembered for the meta-investigation). Studies with a Cook’s distance bigger than the middle in addition to multiple times the interquartile scope of the Cook’s distances are viewed as persuasive. The position relationship test and the relapse test, involving the standard blunder of the noticed results as indicator, are utilized to check for pipe plot deviation (Figure 4). The meta-analysis diagram showing the findings of the relationships between CTR and LVEF is presented in Figure 5. Figure 5 displays a forest plot showing the correlation coefficients for each individual study included in the meta-analysis, as well as the overall pooled correlation coefficient. This plot shows the effect size estimates (represented by squares) and the corresponding confidence intervals (represented by horizontal lines) for each study, with the size of the square indicating the weight of the study in the meta-analysis. This overall pooled correlation coefficient is shown at the bottom of the plot, along with its corresponding confidence interval. This vertical line in the middle of the plot represents the null effect (correlation coefficient of zero), and studies whose confidence intervals cross this line are considered non-significant.

-Heterogeneity statistics of effect sizes.

-Funnel plot of effect sizes for publication bias assessment.
-Heterogeneity statistics of effect sizes in meta-analysis.
A sum of k=13 studies were remembered for the examination. The noticed Fisher r-to-z changed connection coefficients went from - 0.4973 to 0.4356, with most of appraisals being negative (69%). The assessed typical Fisher r-to-z changed connection coefficient in light of the arbitrary impacts model was - 0.1155 (95% CI: - 0.2807 to 0.0497). In this manner, the typical result did not vary altogether from nothing (z=-1.3702, p=0.171). As indicated by the Q-test, the genuine results give off an impression of being heterogeneous (Q(12)=190.1246, p=0.001, tau²=0.0816, I²=96.5409%). A 95% expectation span for the genuine results is given by -0.6992 to 0.4682. Subsequently, albeit the typical result is assessed to be negative, in certain examinations the genuine result may as a matter of fact be positive. An assessment of the studentized residuals uncovered that none of the examinations had a worth bigger than ±2.8905 and thus there was no sign of exceptions with regards to this model. As per the Cook’s distances, the investigations couldn’t really be viewed as excessively powerful. Neither the position connection nor the relapse test demonstrated any pipe plot deviation (p=0.5900 and p=0.9185, individually).
Discussion
In this study, statistical relationships between CTR and LVEF reported in 13 studies conducted worldwide are discussed. According to the findings, when all the results were analyzed together, the mean effect size for CTR and LVEF correlation was found to be r=-0.12. According to the classification of Cohen,39 it can be said that this effect size is small in the negative direction. When all studies are considered separately, generally small negative correlations were observed between CTR and LVEF. From this point of view, it is possible to say that there is no publication bias in the studies.
In conclusion, this study is a meta-analytic study combining 13 studies examining the statistical relationships between CTR and LVEF. The results of this study are expected to contribute to the studies on the relationship between CTR and LVEF and to bring a holistic view to the relationships between these variables.
Highlights:
1) Changes in heart size can be used to monitor the severity of diseases and to determine the degree. Measurements such as heart size, CTR and LVEF; have very important prognostic value in terms of identification, diagnosis, treatment, and follow-up of various heart diseases.
2) In the study, meta-analytical analysis was carried out and it is seen that the Q-value is significant in the heterogeneity tests calculated from the model (Q=190.125, p=0,001).
3) The mean effect size for CTR and LVEF correlation was found to be r=-0.12. When all studies are considered separately, generally small negative correlations were observed between CTR-LVEF.
Acknowledgment
The authors gratefully acknowledge SCRIBENDI (www.scribendi.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 16, 2023.
- Accepted April 11, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.