


Abstract
Objectives: To contribute to this discussion by comparing the complications associated with early-diagnosed versus (vs.) late-diagnosed gestational diabetes mellitus (GDM) for mothers and infants in order to provide baseline data that might guide future changes in the current recommendations for screening.
Methods: The study compares the risk factors and complications for early- vs. late-diagnosed GDM in a cohort from Saudi Arabia. Prenatal, perinatal, postpartum, and neonatal variables were compared between the early vs. late-diagnosed GDM groups using information gathered from the patient’s hospital records.
Results: Significant predictors of early-diagnosed GDM included pregestational BMI and GDM history. Additionally, early diagnosis of GDM was linked to a higher incidence of pre-eclampsia and intrauterine fetal death. Women with early-diagnosed GDM also required more glycemic control interventions, like administering insulin and metformin and controlling their diet. The fetal birth weight and postpartum BMI were significantly higher in the early onset GDM group. The need for insulin and pre-eclampsia were significant factors linked to an early diagnosis of GDM, according to a logistic regression analysis.
Conclusion: Therefore, the current findings emphasize the need for early screening in pregnant women with high pregestational BMI and a history of GDM and show that those with early-onset GDM more likely to need insulin therapy and be at a higher risk of developing pre-eclampsia.
Carbohydrate intolerance that is discovered during pregnancy and can range in severity is known as gestational diabetes mellitus (GDM), a common pregnancy complication.1 The worldwide prevalence of GDM was 10.1% in 2019 according to a meta-analysis and systematic review, with a moderate 27% heterogeneity found between the included studies.2 Overall, the reported prevalence is highly variable, ranging from 1% to 28%, and is influenced by a number of variables, including the diagnostic screening criteria used, the population’s age and ethnic backgrounds, lifestyle factors, and the prevalence of obesity/overweight and type 2 diabetes mellitus.3 The diagnosis of GDM in pregnant women is important, as maternal blood glucose levels have been found to be associated with to a number of negative outcomes for both mothers and their unborn children, including cesarean section, pre-eclampsia, preterm labor, and neonatal birth weight and percent body fat.4 The evolution of coronary artery disease and type 2 diabetes mellitus are 2 long-term complications of GDM in the mother that have received particular attention in previous studies.5,6 With regard to the long-term fetal outcomes, one study reported that GDM was linked to obesity and glucose tolerance in the children.7 Treating GDM between 24 and 31 weeks of gestation has been shown to significantly lower the risk of shoulder dystocia, fetal overgrowth, hypertensive disorders, and cesarean delivery, according to an intervention study.8 Similarly, in pregnant women with GDM use of dietary modifications, regular glucose checks, and insulin treatment from 24 to 34 weeks reported lower occurrence of perinatal complications, better postpartum quality of life, and lower rates of depression according to an interventional study.9 Thus, early detection and management of GDM may be helpful in avoiding negative outcomes for both the mother and the fetus. The first diagnostic criteria of GDM were issued in 1964 and was based on the measurement of oral glucose tolerance.10 Since then, it has undergone a number of modifications, but the oral glucose tolerance test (OGTT) continues to serve as the main diagnostic tool for GDM. Due to the results of the hyperglycemia and adverse pregnancy outcome (HAPO) study, the diagnostic standards for GDM have recently undergone further changes.11,12 This large-scale study was carried out on a heterogenous population of ~25,000 women spanning various cultures, nationalities, and ethnicities, and the findings revealed that high maternal blood glucose levels showed a continuous graded association with increased frequency of several complications for mother and neonate, including preterm delivery, preeclampsia, and neonatal hypoglycemia.11,12 The results were interesting in that they showed that this link was also found for maternal blood glucose levels that were below the diagnostic range for diabetes in the general population.11,12 These results led the International Association of Diabetes in Pregnancy Study Groups (IADPSG) to advise screening for GDM with a 75-g OGTT from 24 to 28 weeks of gestation, with one abnormal result being sufficient for a diagnosis of GDM.13 This screening strategy is accepted by many international groups, including the WHO (2013).13 In addition, the IADPSG guidelines advise initial screening to detect high-risk women at the first follow up based on fasting plasma glucose (FPG), random plasma glucose, or haemoglobin A1c level.13 But there is ongoing discussion regarding the advantages of early screening versus screening after the first 24 weeks of pregnancy.
Recent evidence recommends that GDM should be diagnosed in high-risk patients before 24 weeks of pregnancy, as early onset of GDM is associated with increased risk of gestational hypertension, postpartum hemorrhage, and postpartum glucose abnormalities.14 In comparison to the offspring of mothers in whom GDM was diagnosed after the first 24 weeks of pregnancy, the offspring of mothers diagnosed before 24 weeks were at higher risk of being premature, stillbirth, large for gestational age, and require neonatal intensive care.15 Further, it has been reported that early detection has the potential benefits of avoiding primary cesarean and preventing hypertensive dysfunction and macrosomia.14,15 Therefore, early screening is important for the identification and monitoring of high-risk patients early on, as well as the timely treatment of those diagnosed with GDM before 24 weeks.16 Despite these findings, neither the current World Health Organization guidelines nor the current IADPSG guidelines clearly define the diagnostic criteria for women with abnormal glucose levels detected before 24 weeks of pregnancy or provide information about their management.13,17
The present study aims to contribute to this discussion by comparing the complications associated with early-diagnosed (Ed) versus (vs.) late-diagnosed (Ld) GDM for mothers and infants in order to provide baseline data that might guide future changes in the current recommendations for screening. Further, given that GDM prevalence rate in Saudi Arabia is as high as 24.2%, and there is limited information on the risks of early-onset GDM, the findings will add important data for the region.19
Methods
The current study gathered information by reviewing patient charts from a tertiary hospital in Jeddah, Saudi Arabia. Between January 2020 and March 2023, pregnant women were enrolled. Patients with pre-existing nongestational diabetes and those expecting twins or triplets were excluded, as were patients with incomplete data on their charts. Patients with confirmed abnormal glucose levels according to 75-g OGTT were included. The review and approval of the study protocol was done by the bioethics unit at King Abdulaziz University (approval no. 156-23). The information was obtained from the patients’ medical records, and each patient who visited our center signed a consent form allowing us to use their information for research purposes. The Declaration of Helsinki’s guiding principles were followed when carrying out the study protocol.
Data were collected by reviewing patients’ records at multiple time points. For the initial antenatal visit, data on parity, pre-gestational body mass index (BMI), pre-pregnancy comorbidities, and past obstetric complications were obtained. For the first 2 trimesters, documented evidence of GDM, including OGTT results, was reviewed. For the last trimester, data on the need for insulin to control hyperglycemia, average fasting and postprandial glucose levels, and the occurrence of complications (such as pre-eclampsia and gestational hypertension) were reviewed. In the last stage, data on inpatient admissions, including preterm labor, mode of delivery, maternal birth trauma, and neonatal complications, were examined. Finally, data from postpartum follow-up examinations and data confirming the resolution of GDM were obtained.
At the tertiary care center included in this study, every pregnant woman is tested for GDM. A single-step protocol utilizing a 75-g OGTT is used to screen for GDM beginning at 24 weeks of gestation. Gestational diabetes mellitus is confirmed if one of the following criteria are met: FPG >92 mg/dl, 1-hour plasma glucose >180 mg/dl, or 2-hour plasma glucose >153 mg/dl.13 Pregnant women with obesity, previous macrosomia, or previous GDM who had been lost to follow-up postpartum and had a HbA1c level of <6.5 underwent early 75-g OGTT at first antenatal visit, with the same criteria used to confirm diagnosis.
Statistical analysis
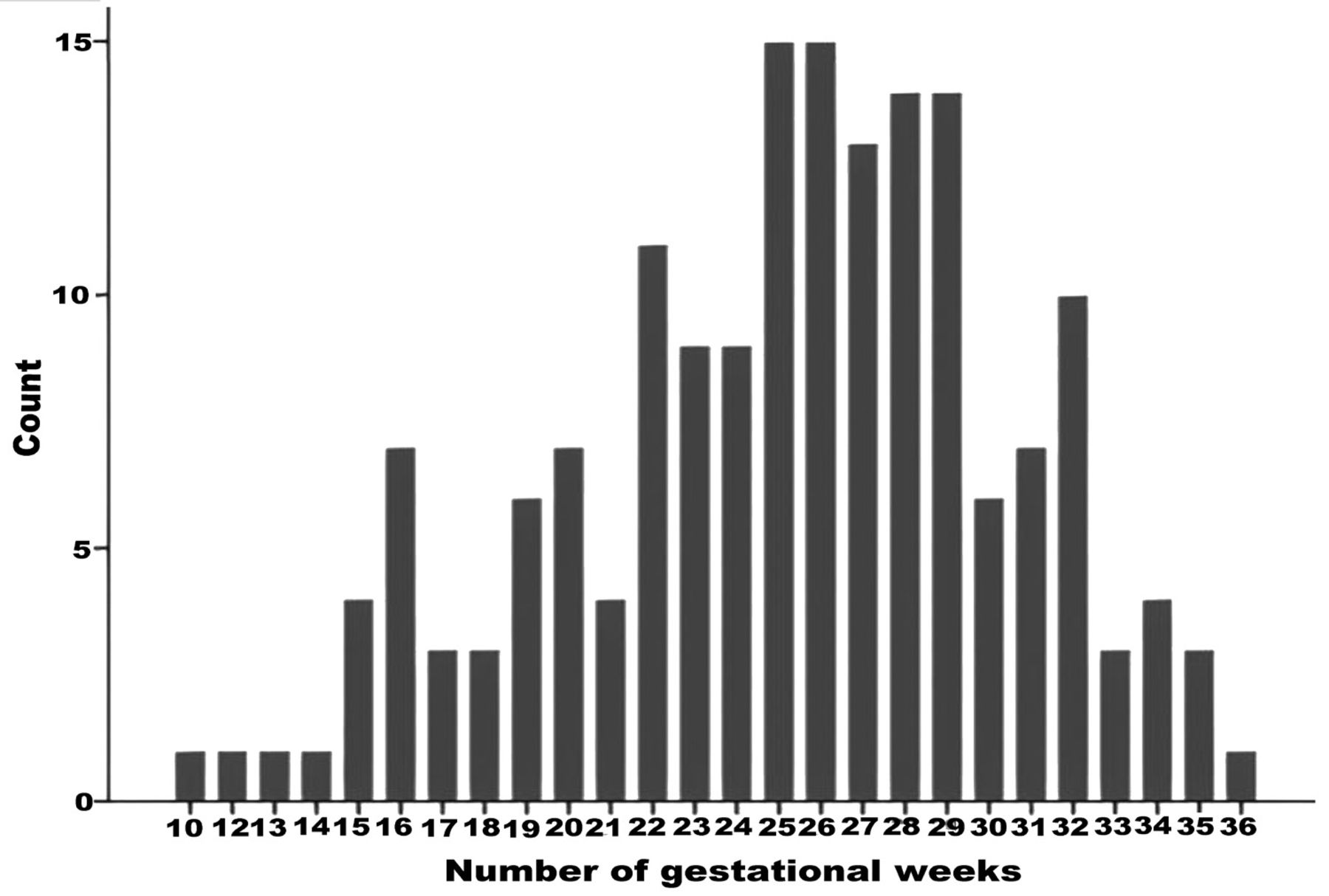
According to gestational age, the frequency of GDM was described (Figure 1). We classified patients according to the time point of diagnosis of GDM into 2 groups: those who underwent early diagnosis (<24 weeks of gestation, Ed-GDM) and those who underwent late diagnosis (>24 weeks of gestation, Ld-GDM). This time point in alignment with previous relevant literature.19,20 The 2 groups were compared with regard to maternal risk factors and obstetric complications. The Shapiro-Wilk and Kolmogorov-Smirnov tests were used to determine whether the distribution of the data was normal or skewed. Chi-square tests and Mann-Whitney tests were used to compare categorical and continuous variables, respectively.
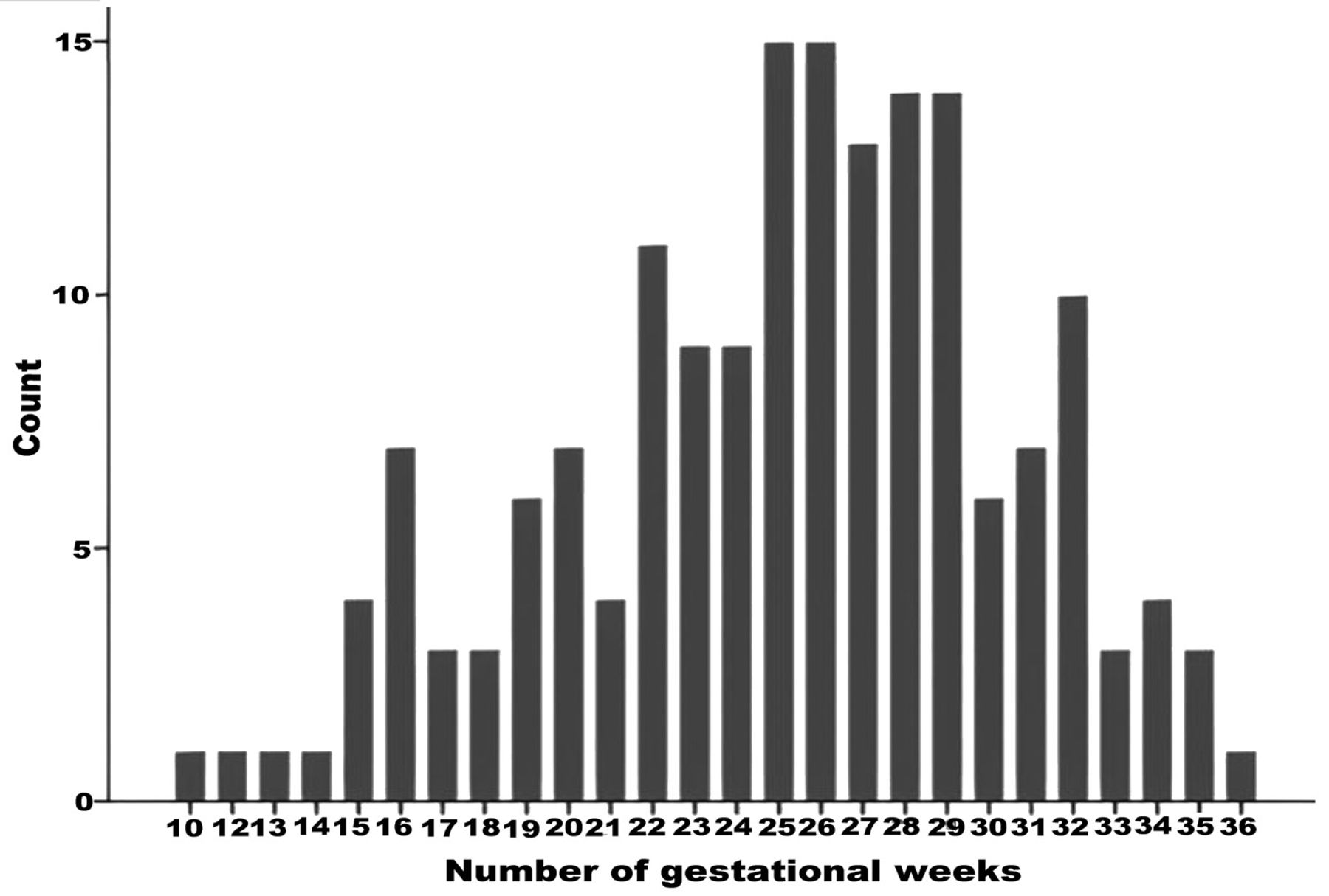
- Number of Number of GDM cases diagnosed per gestational week. cases diagnosed per gestational week.
Next, a binary regression model was used to calculate the adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for each obstetric and neonatal outcome, in order to determine the risks associated with Ed-GDM and Ld-GDM. Pre-eclampsia was confounded by maternal BMI prior to pregnancy, maternal age, parity, pregnancy induction, and the presence of hypertension at the time of pregnancy. Accordingly, the mother’s pre-pregnancy BMI, age, parity, pre-eclampsia, and presence of hypertension were used as cofounder variables for the need for insulin, instrumental delivery, gestational hypertension, maternal birth trauma, preterm labor, macrosomia, and the need for Neonatal intensive care unit (NICU) admission for the infant.
Statistical analysis
Using the Statistical Package for the Social Sciences Statistics for Windows, version 20 (IBM Corp., Armonk, New York, USA) for all statistical analyses were performed. The threshold for statistical significance was set at p=0.05.
Results
Out of the 233 charts that were reviewed, 172 participants’ charts that satisfied the inclusion criteria were used in the current analysis. Fifty nine (34.4%) of the 172 participants were categorized as having Ed-GDM and 113 (65.7%) as having Ld-GDM. The median (interquartile range [IQR]) maternal age in the Ed-GDM group was 34 (8) years, and 35 (8) years in the Ld-GDM group. Furthermore, the median (IQR) interpregnancy interval for Ed-GDM groups was 2 years and 3 years for Ld-GDM groups, (p=0.1). Women with Ed-GDM had a median (IQR) pregestational BMI that was noticeably higher than those with Ld-GDM (29 vs. 27; p=0.05). Gestational diabetes mellitus was diagnosed in previous pregnancies in 72.9% and 51.3% of the women in the Ed-GDM and Ld-GDM groups, respectively, with the difference being significant (p=0.01). However, there was no significant difference in the prevalence of macrosomia in previous pregnancies (Ed-GDM: 10.2%, Ld-GDM: 7.6%, p=0.58). Detailed data for these factors are presented in Table 1.
- Pregestational maternal risk factors.
Insulin was required by 32.2% of Ed-GDM women and 21.2% of Ld-GDM women to control hyperglycemia throughout pregnancy as well as 10.2% of Ed-GDM 2.7% of Ld- GDM patients required a combination of insulin and metformin. The difference in these factors was significant (p=0.01). Instrumental vaginal delivery was performed in 13.5% of Ed-GDM women and 10.1% of Ld-GDM women. A significantly higher number of women in the Ed-GDM than in the Ld-GDM developed gestational hypertension (10.2% vs. 3.5%, p=0.08) and pre-eclampsia (10.2% vs. 1.8%, p =0.02). Intrauterine fetal death (IUFD) occurred in 3 (6.1%) cases in the Ed-GDM but did not occur in the Ld-GDM (p=0.02). Fetal birth weight was significantly higher in the Ed-GDM than in the Ld-GDM (3.1 kg vs. 3.0 kg, p=0.03). The data are presented in detail in Table 2.
- Prenatal maternal and neonatal risk factors.
As shown in Table 3, 54.2% and 60.2% of women in the Ed-GDM and Ld-GDM group did not return for a follow-up visit. Among those who returned for follow-up, a higher percentage of women from the Ed-GDM than from the Ld-GDM developed impaired glucose tolerance (20.3% vs 12.4%) and progressed to overt diabetes (6.8% vs. 3.5%), but the difference was not significant (p=0.36%). Further, maternal weight gain during pregnancy was similar between the groups (p=0.28). However, postpartum BMI was significantly higher in the Ed-GDM than in the Ld-GDM (32 vs. 30, p=0.04).
- Maternal postpartum complications.
Table 4 shows the aOR values for the effect of Ed-GDM on maternal and neonatal complications. The results demonstrate that Ed-GDM is associated with higher risk of pre-eclampsia (aOR: 6.38, 95% CI: 1.17–34.88) and a higher need for insulin to control hyperglycemia (aOR: 2.09; 95% CI: 1.03–4.24).
- Adjusted odds ratios for the impact of early-onset GDM on maternal and neonatal complications.
Discussion
In order to support GDM screening before 24 weeks of gestation, the current study examines the maternal and neonatal risks connected with early detection. The literature on this topic is limited, so the findings will make an important contribution to future modifications of the diagnostic criteria for GDM.
To achieve the study’s goal, 2 groups of pregnant women were divided into: early diagnosed (<24 weeks) and late diagnosed (>24 weeks). This time point has been adopted by similar studies comparing early and late diagnosis of GDM and is based on the currently accepted WHO and IADPGS guidelines.14,15,19-21 In our cohort, 34.4% of the women had early-diagnosed GDM. This is similar to the percentage reported in a recent study from Qatar (34.1%), but much higher than that (0.7%) reported in a cohort from Japan.19,21 However, it is lower than the percentage reported in a recent cohort from Saudi Arabia, in which 71 out of 161 (44%) patients had early-diagnosed GDM.22 In the future, more studies from this region would help shed light on its actual prevalence. A study carried out on an Irish population reported that 18.7% had early-diagnosed GDM, while a retrospective Australian cohort group reported this percentage as 17.3%.14,15 These differences could be attributable to differences in the ethnicities and nationalities of the study cohorts, and they also reflect the wide variation in the prevalence of GDM itself which has been reported in various populations.3
Women in the current cohort who had early diagnosed GDM had significantly higher pregestational BMI than those who had late-diagnosed GDM in terms of the risk factors for early GDM. This is coherent with previous studies which have indicated that high BMI is a risk factor for early-onset GDM and indicates the need for early screening in women with overweight/obesity.14,19-22 But a result of randomized controlled trial reported that early screening for GDM (from 14 to 20 weeks of gestation) in women with obesity failed to reduce the occurrence of perinatal adverse outcomes such as macrosomia, hypertension, shoulder dystocia, and neonatal hypoglycemia.23 Therefore, future research will need to be carried out in larger and more diverse cohorts to determine whether early screening for GDM is indeed beneficial for women with high BMI.
In the current study, we observed that women with early-diagnosed GDM had significantly higher postpartum BMI levels. On the other hand, total maternal weight gain was comparable between the 2 groups, and this could be attributed to the benefits of early diagnosis and dietary modifications. Another factor identified as a significant predictor of early GDM was a history of GDM, and this agrees with the recent study conducted in Saudi Arabia.20 Thus, women with a history of GDM should be considered as having a high risk for GDM and should be screened early on.
With regard to neonatal outcomes, in the present study, the prevalence of IUFD was significantly higher in the early-GDM group, as there were 3 cases of stillbirth as opposed to no cases in the late-GDM group. This finding is in agreement with one of the previous studies on this topic.14 In addition, the recent study from Saudi Arabia indicated that a history of stillbirth was a significant predictor of early GDM.20 However, other results are inconclusive, with one study stating that there was no significant difference in stillbirth rates between the early-GDM and late-GDM groups.21 While another study found that the early-GDM group had a significantly lower stillbirth prevalence.15 Thus, there is insufficient data to suggest that women with early-diagnosed GDM have a higher risk of stillbirth.
The current results show that the early-GDM group had significantly higher fetal weight; however, neither small for gestational age (SGA) nor large for gestational age (LGA) were further investigated. The other reported findings about this are controversial, as 2 studies indicated that early-onset GDM was associated with a higher prevalence of LGA.14,15 Early-onset GDM was linked to a lower prevalence of LGA, according to one study and another study indicated that early-diagnosed GDM was associated with a higher prevalence of SGA.21,25 Thus, more evidence is required to draw conclusions regarding the impact of early-onset GDM on fetal birth weight.
Logistic regression analysis in the present study revealed that pre-eclampsia and the need for insulin showed a significant association with early-diagnosed GDM. In agreement with this, the association of early GDM with a significantly higher prevalence of pre-eclampsia and significantly higher use of insulin has been reported previously.14,15,21 But the other recent study from Saudi Arabia foundno noticeable difference in the prevalence of pre-eclampsia.20 Despite this, given that pre-eclampsia is a serious, and sometimes fatal, prenatal condition characterized by high maternal blood pressure and proteinuria, it is important to screen early for GDM based on the observed high risk of pre-eclampsia in those with early-onset GDM in the present cohort.
The higher use of insulin reported in women with early-onset GDM may reflect the greater need for glycemic control in these women. Maternal glycemic control is important for fetal cardiac function, synchronization of the circadian rhythm, and maintenance of optimal levels of N-terminal pro-brain type natriuretic peptide (which regulates extracellular fluid volume and blood pressure).24-26 In contrast, tight glycemic control could potentially lead to fetal growth retardation.27 Thus, it is important to conduct future investigations into the management of glycemic control in women with early-onset GDM, and this finding also highlights the importance of diagnosing and treating early-onset GDM in a timely way.
Study limitation
Some limitations in the design of this study are its small sample size, the procurement of data from a single center, and the lack of control groups (control group without GDM and control group that did not receive glycemic control interventions). These limitations can be overcome through future studies on larger cohorts recruited from multiple centers that include matched control groups. Besides, several maternal and neonatal adverse events that were previously described to be significantly associated with early-onset GDM, for example, postpartum hemorrhage, and congenital abnormalities, were not examined here. Thus, future studies should include a wider range of both maternal and fetal outcomes.
To conclude, the present findings highlight the risks of early-onset GDM and point to the need for modifications in the current guidelines on the appropriate time point for GDM screen. Depends on the findings, we recommend early screening in women with previous GDM and those with high pregestational BMI.
Acknowledgment
The authors gratefully acknowledge Oxford Science Editing for the language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 20, 2023.
- Accepted June 21, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.