


Abstract
Objectives: To investigate the positive effects of intraperitoneal administration of alpha-lipolic acid (ALA) and dexpanthenol (DXP) on wound healing after tracheal surgery in rats.
Methods: The study was carried out at Necmettin Erbakan University, Konya, Turkey, from January 2014-2019. A total of 30 healthy and adult Sprague-Dawley type female rats were included in the study. For the experiment, rats were randomly divided into 3 groups: ALA group (n=10), DXP group (n=10), and control group (n=10). After trachea surgery, 100 mg/kg/day ALA was given to group ALA and 100 mg/kg/day intraperitoneal DXP to group DXP for 15 days, and the rats were sacrificed on the 21st day. The excised tracheal sections were evaluated and graded for inflammatory cell infiltration, angiogenesis, fibroblast proliferation, collagen deposition, and epithelial regeneration to evaluate wound healing.
Results: Inflammation was found to be less in both the ALA and DXP groups. With the Mann-Whitney test, it was determined that inflammation was less in the ALA group than in the DXP group (C-D [p=0.097] and C-A [p=0.024]). On the other hand, no statistically significant difference was found in epithelial regeneration (p=0.574; >0.05), angiogenesis (p=0.174; >0.05), fibroblast proliferation, and collagen deposition (p=0.102; >0.05).
Conclusion: Alpha-lipolic acid injected intravenously after tracheal reconstruction in patients can prevent restenosis by reducing inflammation without adversely affecting wound healing
The trachea is an organ located between the larynx and the bronchi, approximately 10-13 cm in length in an adult, consisting of 18-22 cartilage rings, located in the neck and thorax. It starts from the level of the 5th cervical vertebra above and descends to the level of the 5th thoracic vertebra below.
Tracheal surgery started in 1881 by Gluck and Zeller in a patient who had been planned to have a laryngectomy in 2 stages, as the first step, by opening the trachea to the skin.1 Tracheal resections and reconstructions are types of operations carried out for benign strictures, perforations, and malignancies of the trachea. Although the best approach to localized lesions in the cervical trachea is the cervical collar incision, it is appropriate to approach lesions in the lower half of the trachea through the 4th intercostal space with a right posterolateral thoracotomy.
Tracheal surgery has some difficulties such as providing the nutrition of the trachea segmentally with terminal vessels, being rich in cartilage tissue, overreacting biologically to foreign tissue, the tension on the anastomosis line after resection, and proximity to vital organs, as well as difficulties due to the anatomical structure and location of the trachea. Many fatal complications can occur after surgery, from minimal granulation and stenosis to complete disruption of the anastomosis due to ischemia.2 Particularly, granulation at the surgical site is a common complication. In order to avoid these complications, a careful surgical technique should be applied in dissection and anastomosis after resection, the ends should be brought together, absorbable sutures should be used, the nodes should be excluded from the lumen, and asepsis and antisepsis should be considered.
In recent years, many experimental studies have been carried out with various agents to minimize granulation tissue. Two of these are alpha-lipolic acid (ALA) and dexpanthenol (DXP). Alpha-lipolic acid is a molecule that is required as a cofactor in energy metabolism in all organisms and has recently been shown to have antioxidant properties.3 Dexpanthenol (provitamin B5) is the precursor of pantothenic acid, one of the B-complex vitamins. It is a molecule that has been observed to accelerate epithelialization and wound healing.4
In our study, we aimed to evaluate the usefulness of these 2 chemical agents in tracheal surgery, by comparing the positive effects of these 2 chemical agents on wound healing, which has been observed in many other tissues in recent experimental studies, with each other and with the control group.
Methods
This experimental study was carried out at the animal laboratory of Necmettin Erbakan University, Konya, Turkey, from January 2014-2019. Our study was started after the approval of the Experimental Animals Ethics Committee (no.: 2009/58). Experiments were carried out using 30 healthy and adult Spraque-Dawley type female rats weighing 200-250g. Rats were fed with standard feed and tap water throughout the experiment. Animals were acclimated to laboratory conditions for one week before the experiment. They were exposed to a 12-hour light and 12-hour dark cycle at a room temperature of 22°C. For the experiment, rats were randomly divided into 3 groups: ALA (Merck KgaA, Darmstadt, Germany) group (n=10), DXP (Merck KgaA, Darmstadt, Germany) group (n=10), and control group (n=10). Rats in all groups were to fast for 8 hours before the procedure. The subjects were anesthetized intramuscularly with 50 mg/kg of ketamine hydrochloride (Pfizer PFE, Kırklareli, Turkey) and 10 mg/kg of xylazine hydrochloride (Merck KgaA, Darmstadt, Germany).
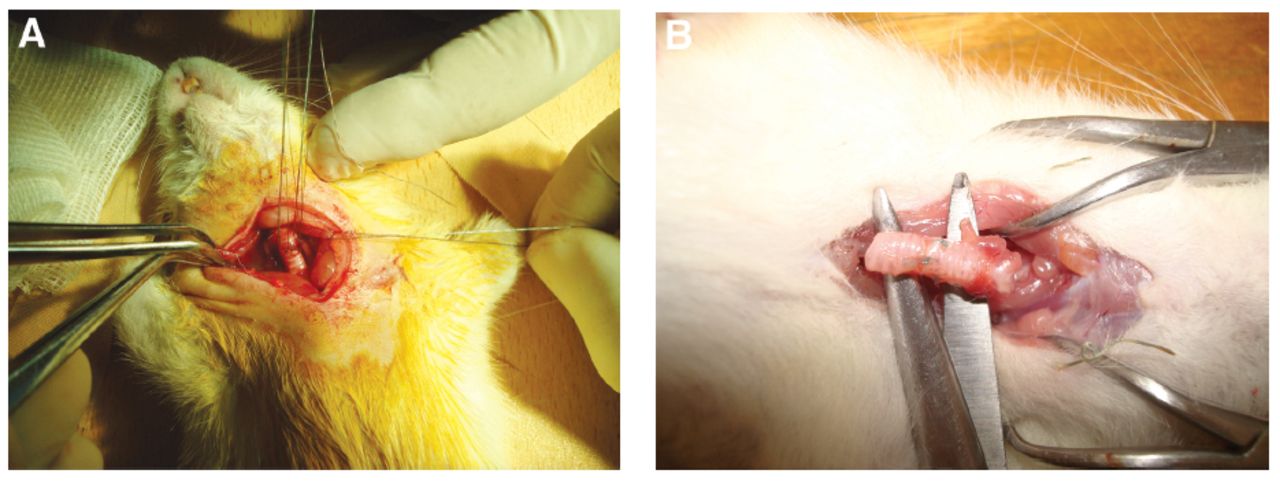
A 2 cm long horizontal cervical skin incision was carried out under sterile conditions by lying in the supine position. After blunt and sharp dissections, the strap muscles were retracted. After the trachea was seen, the anterior tracheal wall was cut with a transverse incision. Afterwards, the incision was sutured one by one with 6/0 polyglactin (absorbable) sutures (Figure 1A). After the layers were duly closed, the skin was sutured one by one with 3/0 silk sutures. Oxygen was continued until the rats woke up. After awakening from anesthesia, 100 mg/kg/day ALA was given to group ALA and 100 mg/kg/day intraperitoneal DXP was given to group DXP for 15 days from the day of operation. Control group did not receive any treatment. A total of 3 rats from each group died during intraoperative and postoperative care. On the 21st postoperative day, the subjects were sacrificed under general anesthesia. Tracheas were excised one cm above and below the sutured tracheal incisions (Figure 1B).

- Images of trachea during the first and second surgery. A) The tracheal incision sutured one by one with a 6/0 polyglactin (absorbable) sutures. B) Tracheal fragment excised one cm above and below the tracheal incision. The anastomotic line appears intact.
Specimens were fixed with a 10% neutral buffered formalin solution. The specimens were then evaluated objectively by a pathologist after hematoxylin-eosin and trichrome staining.
Inflammatory cell infiltration, angiogenesis, fibroblast proliferation, and collagen deposition were examined and graded to evaluate wound healing. Ehrlich/Hunt numerical scale was used for rating: “0” for absence; “1” for occasional presence; “2” for light scattering; “3” for abundance; and “4” for confluence of cells or fibers.5
Epithelial regeneration was evaluated as “0” no epithelium; “1” single-layer epithelium with a partial closure; and “2” stratified epithelium with complete closure (according to Loewen’s study).6
Statistical analysis
All data were recorded as mean and standard deviation (SD). Kruskal-Wallis analysis of variance was carried out for group comparisons. The significance of differences among the groups was determined by a non-parametric Mann-Whitney U-test. Values of p<0.05 were considered significant. All statistics were analyzed with the Statistical Package for the Social Sciences, version 22.0 (IBM Corp., Armonk, NY, USA)
Results
A total of 2 rats in each group died during surgery and one rat died during treatment. No infections or other complications developed in the other rats. They showed normal activity and eating habits until sacrificed.
In the macroscopic examination of the trachea pieces that were removed to include the suture line, it was observed that the anastomosis line was intact, there was no separation or narrowing in the lumen. The prepared specimens were examined histopathologically and epithelial regeneration, inflammatory cell infiltration, angiogenesis, fibroblast proliferation, and collagen deposition were scored. Histopathological scores are shown in Table 1.
- Histological scoring of the cases.
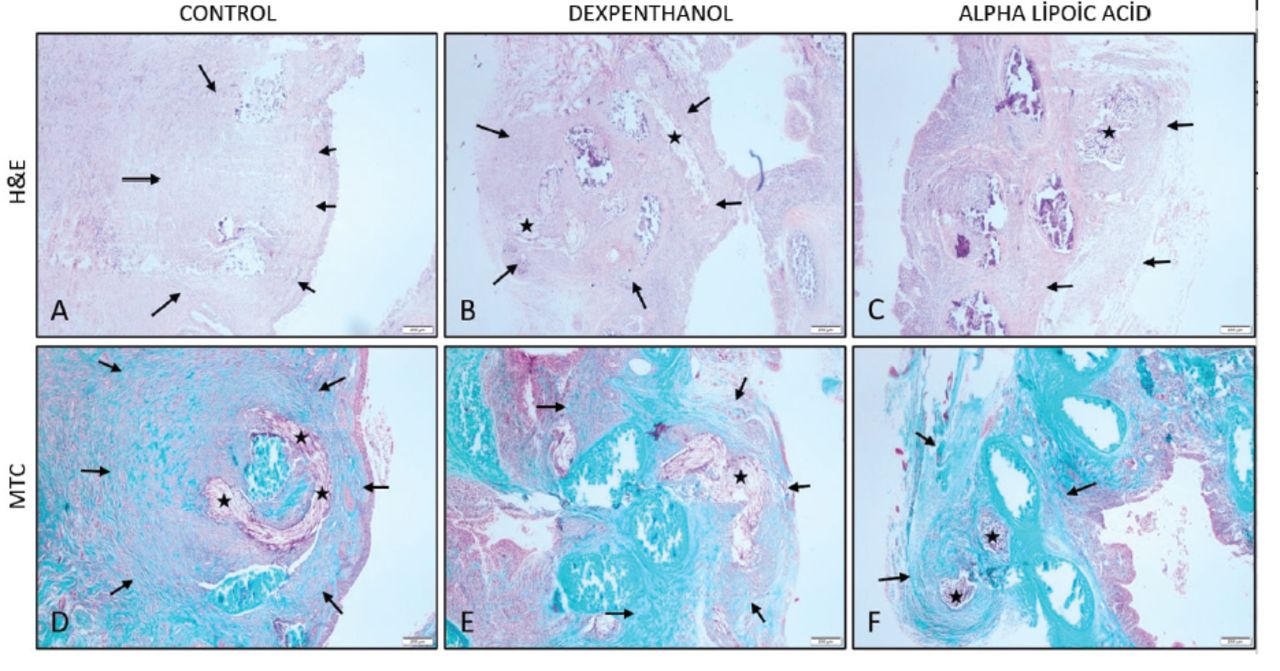
In the comparison of the 3 groups with Kruskal-Wallis, a significant difference was found in inflammation (p=0.036; <0.05). Inflammation was found to be less in both ALA and DXP groups. Therewith it was determined that inflammation was less in the ALA group than in the DXP group in the Mann-Whitney test carried out (control-DXP [p=0.097] and control-ALA [p=0.024]). Collagen deposition was found to be higher in the control group. On the other hand, no statistically significant difference was found in epithelial regeneration (p=0.574; >0.05), angiogenesis (p=0.174; >0.05), and fibroblast proliferation and collagen deposition (p=0.102; >0.05; Figure 2).

- Hematoxylin & eosin (H&E) and Masson’s trichrome staining (MTC) of the anastomosis line. Asterisks denote the suture materials and arrows denote the wound healing zone.
Discussion
Alpha-lipoic acid is a molecule synthesized by all microorganisms, including plants and animals, and has recently demonstrated anti-oxidant characteristics.7 Alpha-lipoic acid is defined as an ideal, unique, and universal antioxidant due to its rapid absorption, its antioxidant effect in both its oxidized and reduced forms, its dissolution in both liquid and lipid phases, and others. Excessive oxidative stress has been implicated in various pathological conditions, including inflammation. There are publications showing the use of ALA’s anti-inflammatory effect for many inflammatory diseases such as encephalomyelitis, rheumatoid arthritis, and others.8 By neutralizing reactive oxygen species and preventing oxidative damage, ALA can reduce the activation of inflammatory pathways and the release of pro-inflammatory molecules. Our study provides evidence for the potential role of ALA-mediated reduction in oxidative stress in attenuating inflammation. Further research is warranted to elucidate the specific mechanisms underlying this relationship and to explore the clinical implications of ALA supplementation in conditions characterized by inflammation and oxidative stress. Dexpanthenol is the alcohol form of pantothenic acid, which is a factor of the vitamin B complex.9 Panthenol is also known as provitamin B5. Dexpanthenol is a synthetic form, not found naturally but converted into pantothenic acid in the body. It is possible to obtain pantothenic acid with a variety of foods. It is abundant in the liver, spleen, egg yolk, yeast, and broccoli. Pantothenic acid participates in the structure of coenzyme A, which is an essential coenzyme for the maintenance of life. Coenzyme A is required in the synthesis of essential oils, cholesterol, steroid hormones, acetylcholine, and melatonin.10 It is used topically in many cosmetic products as an accelerator, protective, moisturizing, and anti-inflammatory on the skin.
We could not find any data in the literature on the use of these 2 chemical agents, which have come to the fore in recent years, for tracheal healing. Preventing postoperative stenosis, which we frequently experience in the thoracic surgery, formed the hypothesis of this study we carried out on rats.
Tracheal resection and reconstruction are frequently applied in tracheal stenoses and malignancies that develop after intubation. In a series of 52 patients in which Mohsen et al11 carried out long segment tracheal resection, the most common reason for surgery was post-intubation tracheal stenosis. The wound healing process begins immediately after tracheal resection and anastomosis at the suture line. The first step in wound healing is the inflammatory reaction, which is the collection of epithelial, endothelial, and inflammatory cells together with platelets and fibroblasts to repair damaged tissue.12 During this healing process, the increased fibroblastic activity causes the formation of retractile fibrous tissue, which causes stenosis and airway obstruction.13 Variables such as operation technique, suture materials used, and others affect the formation of this fibrous tissue.
Complications related to anastomosis, such as granulation tissue in the anastomotic line, stenosis after tracheal resection, and reconstruction cause serious morbidity. In the most comprehensive study on tracheal resection and reconstruction, Wright et al14 reported that 9% of 901 patients had complications related to anastomosis. In our study, in the macroscopic examination of the tracheal pieces removed after sacrificing all the subjects, it was found that the anastomosis line was intact, there was no separation, and no narrowing in the lumen. This showed us that the surgical technique used was suitable for the trachea.
Many studies have been carried out to minimize anastomosis-related morbidity after tracheal surgery. Liman et al12 found that estradiol and progesterone inhibit massive collagen deposition and fibroblast proliferation in tracheal healing and emphasized that this could be used to prevent tracheal stenosis. Hyperbaric oxygen therapy was also used in rats after tracheal anastomoses, and they reported that it increased tracheal healing and reduced the complication rate. Trachea fragments removed in our study were prepared and examined histopathologically. Inflammation was found to be less in both ALA and DXP groups compared to the control group (p=0.036; <0.05). In a study carried out on mice, similar to our study, it was shown that ALA given as 200 mg/kg gavage prevented inflammation, intestinal dysmotility, and diarrhea which are the undesirable effects of an anti-cancer drug called irinotecan, and contributed positively to the treatment process.15 In another study carried out by Altunina et al16 on 112 patients with diabetes mellitus and myocardial infarction history, it was observed that the use of ALA for 4 months caused a significant decrease in the levels of CRP, IL-6, and TNF-alpha, which are inflammation parameters.
Dexpanthenol, which is the alcohol form of pantothenic acid, a factor of the vitamin B complex, is generally known to have an accelerating effect on wound healing, but there are also publications showing its anti-inflammatory effect.17 Compared to DXP, there are many publications emphasizing the anti-inflammatory characteristics of ALA. As a result of the Mann-Whitney test, which we applied to compare the experimental results, we found that ALA reduced inflammation more than DXP. We believe that ALA to be injected intravenously after tracheal reconstruction can prevent restenosis in clinical use by reducing inflammation without adversely affecting wound healing.
Study limitations
Our research focused solely on a specific animal model, which may limit the generalizability of the findings to other species or human populations. The sample size was relatively small, which could impact the statistical power and generalizability of the results. Lastly, due to resource constraints, we were unable to investigate certain variables or factors that could have provided further insights into the phenomenon under study. Despite these limitations, the findings of our research contribute to the existing knowledge in the field and provide a foundation for future studies to build upon. We think that our hypothesis will be supported by human studies in large series on this subject.
In conclusion, we focused on investigating the individual effects of ALA and DXP to avoid potential confounding factors. Individual treatments were examined seperately to provide clearer insights into their efficacy and safety profiles. We did not include the group ALA+DXP in the study due to the lack of previous evidence supporting the synergistic effect of ALA+DXP. The inclusion of an ALA+DXP group can add complexity to the interpretation of the results. If the ALA+DXP combination produces different results compared to individual treatments, it may be difficult to attribute effects to this combination. However, if we had more rats, it would be useful to add the combined effect of these 2 components. We think that our study will be a guide for future research on this subject.
Acknowledgment
The authors gratefully acknowledge Protranslate (www.protranslate.net) for English language editing.
Footnotes
Disclosure. This study was funded by the Scientific Research Projects Unit of Necmettin Erbakan University, Konya, Turkey (project no.# 10401108).
- Received April 18, 2023.
- Accepted July 24, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.